60Fd5fd200e081c439b83d85540
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Poverty Map Report
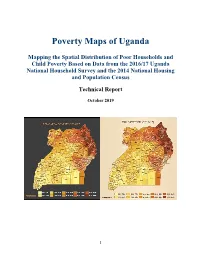
Poverty Maps of Uganda Mapping the Spatial Distribution of Poor Households and Child Poverty Based on Data from the 2016/17 Uganda National Household Survey and the 2014 National Housing and Population Census Technical Report October 2019 1 Acknowledgement This technical report presents the results of the Uganda poverty map update exercise, which was conducted by the Uganda Bureau of Statistics (UBOS) in close collaboration with UNICEF and the World Bank. The core task team at UBOS consisted of Mr. James Muwonge (Director of Socio-Economic Surveys), Mr. Justus Bernard Muhwezi (Manager of Geo-Information Services), Mr. Stephen Baryahirwa (Principal Statistician and Head of the Household Surveys Unit), Mr. Vincent Ssennono (Principal Statistician and Head of the Methodology and Analysis Unit), and Mr. Adriku Charles (Senior Geo-Information Officer). The core task team at the World Bank consisted of Dr. Nobuo Yoshida (Lead Economist), Dr. Carolina Mejia-Mantilla (Uganda Country Poverty Economist), Dr. Minh Cong Nguyen (Senior Economist) and Ms. Miyoko Asai (Consultant). Dr. Nobuo Yoshida and Dr. Minh Cong Nguyen supervised the exercise and ensured that the latest international experience and technical innovations were available to the team. The core task team in UNICEF consisted of Dr. Diego Angemi (Chief Social Policy and Advocacy), Mr. Arthur Muteesasira (Information Management and GIS Officer), and Ms. Sarah Kabaija (Monitoring and Evaluation Specialist). The team benefited from the support and guidance provided by Dr. Robin D. Kibuka(Chairman of the Board, UBOS), Ms. Doreen Mulenga (Country Representative, UNICEF), Mr. Antony Thompson (Country Manager, World Bank), and Dr. Pierella Paci (Practice Manager, World Bank). -

Dairy Development in Uganda
DAIRY DEVELOPMENT IN UGANDA MinistryThe Republic of Agriculture of Uganda Animal Industry and Fisheries (MAAIF) Food and Agriculture A Review of Uganda’s Dairy Industry Organization of the United Nations Dairy Development Authority (DDA) Author: David Balikowa National Consultant, GOU/FAO Dairy Project, TCP/UGA/3202(D); Senior Business Advisor, TechnoServe/East Africa Dairy Development Project (EADD) March 2011 i TABLE OF CONTENTS LIST OF TABLES .................................................................................................................................. v LIST OF FIGURES ................................................................................................................................ v ACRONYMS AND ABBREVIATIONS .....................................................................................................vi EXECUTIVE SUMMARY ...................................................................................................................... vii CHAPTER 1 ........................................................................................................................................ 1 1. INTRODUCTION ......................................................................................................................... 1 1.1 Geographical Location of Uganda ....................................................................................... 1 1.2 Contribution of Agriculture to the National Economy ......................................................... 1 1.3 Historical Overview of -

DOWNLOAD IPC Uganda Acutefi Situation
REPORT OF THE INTEGRATED FOOD SECURITY PHASE CLASSIFICATION ANALYSIS FOR UGANDA PREPARED BY UGANDA IPC TECHNICAL WORKING GROUP January 2016 1 Table of Contents Table of Contents .................................................................................................................................... 2 Acronyms ................................................................................................................................................. 4 CHAPTER ONE .......................................................................................................................................... 6 1.0 FOOD SECURITY ANALYSIS METHODOLOGY AND SCOPE ............................................................ 6 1.1 Background .......................................................................................................................................... 6 1.2 IPC Approach ....................................................................................................................................... 6 1.3 Acute Food Insecurity Analysis- November 2015 to April 2016 ................................................... 7 1.4 Methodology ....................................................................................................................................... 7 1.5 Limitations ........................................................................................................................................... 8 1.6 Summary Findings .............................................................................................................................. -

Minority Rights Group International, Maragoli Community Association
JOINT SUBMISSION TO THE OFFICE OF THE HIGH COMMISSIONER FOR HUMAN RIGHTS ON THE OCCASION OF UGANDA’S 3RD CYCLE UNIVERSAL PERIODIC REVIEW, 40TH SESSION, JANUARY-FEBRUARY 2022 Submission by Minority and Indigenous Groups Report on Health and Education, July 2021 Joint Submission by: Minority Rights Group International, Maragoli Community Association, Benet Lobby Group, North Karamoja Indigenous Minority Group Platform, African International Christian Ministries, United Organization for Batwa Development in Uganda, Action for Batwa Empowerment Group, Eliana R’s and Jamp Banyabindi Foundation, Buliisa District Union of persons with Disabilities, Tapac Integrated Development Organization, Mount Elgon Benet Ogiek Group Organization. 1 CO-SUBMITTING ORGANISATIONS Organization Address Organization Contact Person Maragoli P.O Box 34 Kigumba, Mwale Paul Community Kiryandongo District. 0777 313 677 Association [email protected] (MCA) Maragoli Community Association (MCA) is a non-governmental organization Founded in 1998 and registered as a CBO in 2016. MCA was Formed to Fight For recognition oF the Maragoli as one oF the indigenous communities in Uganda. In addition to citizenship recognition, MCA works towards ensuring that Maragoli community members enjoy Full rights to social services such as health and education and other political rights like any other citizens oF Uganda. MCA currently operates in the districts oF Kiryandongo, Masindi, Hoima, Bugiri and Iganga. African [email protected] Nabimanya Precious Arinda International www.aicmuganda.org 0773 300 302 Christian www.aicm.org.uk Ministries (AICM) P.O. Box: 459 Kampala , Uganda African International Christian Ministry (AICM) is a non-governmental, non-denominational, nonpartisan and a non-proFit making organization which was Founded in 1983. -

A Super-Efficiency Data Envelope Analysis Model Bruno Yawe
Hospital Performance Evaluation in Uganda: A Super-Efficiency Data Envelope Analysis Model Bruno Yawe Makerere University Standard Data Envelope Analysis models result in a large fraction of the observations becoming 100 percent efficient. The article measures the technical efficiency of 25 district referral hospitals from three regions of Uganda over the 1999-2003 period. It applies a super-efficiency Data Envelopment Analysis model. The application of a super-efficiency model was occasioned by the failure of standard data envelopment analysis models to rank the efficient set of hospitals which attain an efficiency score of unity. The results of the standard data envelopment analysis models indicate the existence of different degrees of technical and scale inefficiency in Uganda’s district referral hospitals. With the super-efficiency model, a ranking of the efficient units is possible. When super- efficiency models are executed, hospitals can be ranked and categorised into four groups: strongly super-efficient; super-efficient; efficient and inefficient. 1. Introduction 1 Since the early 1980s, Data Envelopment Analysis (DEA) has been used as an alternative method of classification to evaluate the relative efficiency of independent homogenous units which use the same inputs to produce the same outputs (Cooper, Seiford and Tone, 2000). However, a serious inconvenience in the utilisation of DEA as a method of classification is the possibility of having units tied with relative efficiency equal to 100 percent. That is, units at the frontier of relative efficiency. Various authors have tackled this inconvenience using various devices to break the tie, such as crossed evaluation (Green et al., 1996), super- efficiency (Anderson and Peterson, 1993) or assurance regions (Cooper et al., 2000), among others. -
In Uganda, but Full Equality with Men Remains a Distant Reality
For more information about the OECD Development Centre’s gender programme: [email protected] UGANDA www.genderindex.org SIGI COUNTRY REPORT Social Institutions & Gender Index UGANDA SIGI COUNTRY REPORT UGANDA SIGI COUNTRY Uganda SIGI Country Report The opinions expressed and arguments employed in this document are the sole property of the authors and do not necessarily reflect those of the OECD, its Development Centre or of their member countries. This document and any map included herein are without prejudice to the status of or sovereignty over any territory, to the delimitation of international frontiers and boundaries and to the name of any territory, city or area. © OECD 2015 UGANDA SIGI COUNTRY REPORT © OECD 2015 FOREWORD – 3 Foreword Uganda’s economic and political stability over the past two decades has brought unprecedented opportunities to address social inequalities and improve the well-being of citizens. Investments in key human development areas have reaped benefits in poverty reduction, and seen some improvements on a range of socio-economic indicators: but is everyone benefiting? Ugandan women and girls have partially benefited from these trends. New laws and measures to protect and promote women’s economic, political and human rights have been accompanied by impressive reductions in gender gaps in primary and secondary education and greater female political participation. Yet, wide gender gaps and inequalities remain, including in control of assets, employment and health. Economic development may have improved the status quo of women in Uganda, but full equality with men remains a distant reality. Tackling the discriminatory social norms that drive such gender inequalities and ensuring that women can equally benefit from Uganda’s development were twin objectives of this first in-depth country study of the OECD Social Institutions and Gender Index (SIGI). -

Environment & Energy Sector Dashboard Q4 2020
Environment & Energy Dashboard Quarter 4 Uganda Refugee Response Plan (RRP) 2020-2021 January - December 2020 ENVIRONMENT OVERVIEW Objective 1: Environment and natural resources protected and restored and green livelihoods promoted using a catchment-based approach With support from the Office of the Prime Minister, partners including district local governments continued to jointly implement environmental activities such as community mobilization and sensitization, environmental restoration and protection, raising tree seedlings, tree growing and maintenance and green livelihoods such as beekeeping, agroforestry and support to nursery operators albeit the challenges of COVID-19 pandemic and associated restrictions. NFA continued maintenance activities for the 422 hectares restored in 2019 in the Central Forest Reserves (CFRs) of Eria and Era in Obongi district and Bugoma in Kikuube district. An additional 49 hectares of bamboo were planted in Era CFR to replace the areas affected by fires as part environmental restoration activities, bringing the cumulative restored area to 471 ha. Approximately 6.25 million assorted tree seedlings were raised across the 13 different nursery sites and by end of Q4 2020, 83% of these seedlings had been distributed to beneficiaries for planting with the remaining 122,741 seedlings unplanted because some of them became overgrown during the Covid-19 restrictions, losses from disease and insufficient water during the maintenance to Season II and the ungrafted fruit seedlings. The established community woodlots across the operation were mainly maintained using agroforestry approaches such as taungya system where the trees are intercropped with food crops for the refugees and host communities who weed their crops while simultaneously weeding the woodlots. -
Feed the Future Uganda 2015 Zone of Influence Interim Assessment Report October 2015
Feed the Future Uganda 2015 Zone of Influence Interim Assessment Report October 2015 Prepared for the United States Agency for International Development, USAID Contract Number GS-23F-8144H/AID-OAA-M-12-00006, Feed the Future FEEDBACK Recommended Citation: Feed the Future FEEDBACK. 2015. Feed the Future Uganda 2015 Zone of Influence Interim Assessment Report. Rockville, MD: Westat. USAID Bureau for Food Security Contact: [email protected] Westat Contact: Detra Robinson, MA, PMP, Chief of Party 1600 Research Boulevard Rockville, MD 20850 Tel: (301) 738-3653 Email: [email protected] Table of Contents List of Acronyms ................................................................................................................ viii Executive Summary .............................................................................................................. ix Background ...................................................................................................... ix Interim Assessment Indicators .................................................................... ix Interim Assessment Data Sources ............................................................... x Summary of Key Findings ............................................................................... x Household Economic Status ............................................................ x Women’s Empowerment in Agriculture Index Indicators ............................................................................ xi Hunger and Dietary Intake ............................................................ -
The Life and Times of the Institutional Capacity Building Project in The
The Life and Times of the Institutional Capacity Building Project in the Health Sector in Uganda Lessons learned in leadership and management i The Life and Times of the Institutional Capacity-Building Project in the Health Sector in Uganda The Life and Times of the Institutional Capacity-Building Project in the Health Sector in Uganda Julius Balinda, Hans Beks, Isaac Ezati, James Ikabat, Eric Kakoole, Resty Kamya, Florence Kebirungi, Abassi Mansour, Ronald Miria Ocaatre, Richard Obeti, Bernard Odu, David Okia, Charles Olaro, Jimmy Opigo, Jakor Oryema, Damian Rutazaana, Martin Ssendyona Anke van der Kwaak and Marjolein Dieleman (eds) BTC Uganda and the Ministry of Health Uganda November 2015 Kampala, Uganda i The Life and Times of the Institutional Capacity-Building Project in the Health Sector in Uganda Colofon: Belgian Technical Cooperation BTC – Uganda Lower Kololo Terrace Plot 1B P.O. Box 40131 Kampala, Uganda Ministry of Health Lourdel Road, Nakasero, Uganda Ministry of Health Royal Tropical Institute (KIT) P. O. Box 95001 1090 HA Amsterdam The Netherlands This is an open access publication distributed under theterms of the Creative Commons Attribution Licence which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited. © 2015 BTC Uganda Edited by Jon Stacey, The Write Effect, Oxford, UK Photos: BTC Uganda Cover photo: BTC Uganda ii iii The Life and Times of the Institutional Capacity-Building Project in the Health Sector in Uganda The Life and Times of the Institutional Capacity-Building Project in the Health Sector in Uganda Contents Acknowledgements Dr Asuman Lukwago ................................. vi Foreword Dr Isaac Alidria-Ezati .............................................. -
Rebounding from the Brink of Extinction
CLIMATE-SMART AGRICULTURE REBOUNDING FROM THE BRINK OF EXTINCTION: Commercial production of milk amongst pastoralists for climate change resilience in Uganda ABOUT CTA The Technical Centre for Agricultural and Rural Cooperation (CTA) is a joint international institution of the African, Caribbean and Pacific (ACP) Group of States and the European Union (EU). CTA operates under the framework of the Cotonou Agreement and is funded by the EU. For more information on CTA, visit www.cta.int Photos cover, p. 9, p. 25, p. 31: © Shutterstock All other photos: © Authors © CTA, 2018. ISBN 978-92-9081-637-9 DISCLAIMER This work has been made with the financial assistance of the European Union. However, it remains under the sole responsibility of its author(s) and never reflects CTA’s or its co- publisher’s or European Union’s opinions or statements whatsoever nor as well the opinion of any country or State member. The user should make his/her own evaluation as to the appropriateness of any statements, argumentations, experimental technique or method as described in the work. This work is the intellectual property of CTA and its co-publishers. Its dissemination is encouraged for private study, research, teaching, under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/legalcode), provided that appropriate acknowledgement is made: - of CTA’s copyright, in accordance with the license Creative Commons 4.0, and of EU financing, by including the name of the author, the title of the article and the following notice “© CTA 2018 EU financing”, - and that CTA’s or its co-publishers or EU’s endorsement of authors’ views, products or services is not implied in any way, by including the standard CTA disclaimer. -

Regional Development for Amuru and Nwoya Districts
PART 1: RURAL ROAD MASTER PLANNIN G IN AMURU AND NWOYA DISTRICTS SECTION 2: REGIONAL DEVELOPMENT FOR AMURU AND NWOYA DISTRICTS Project for Rural Road Network Planning in Northern Uganda Final Report Vol.2: Main Report 3. PRESENT SITUATION OF AMURU AND NWOYA DISTRICTS 3.1 Natural Conditions (1) Location Amuru and Nwoya Districts are located in northern Uganda. These districts are bordered by Sudan in the north and eight Ugandan Districts on the other sides (Gulu, Lamwo, Adjumani, Arua, Nebbi, Bulisa, Masindi and Oyam). (2) Land Area The total land area of Amuru and Nwoya Districts is about 9,022 sq. km which is 3.7 % of that of Uganda. It is relatively difficult for the local government to administer this vast area of the district. (3) Rivers The Albert Nile flows along the western border of these districts and the Victoria Nile flows along their southern borders as shown in Figure 3.1.2. Within Amuru and Nwoya Districts, there are six major rivers, namely the Unyama River, the Ayugi River, the Omee River, the Aswa River, Tangi River and the Ayago River. These rivers are major obstacles to movement of people and goods, especially during the rainy season. (4) Altitude The altitude ranges between 600 and 1,200 m above sea level. The altitude of the south- western area that is a part of Western Rift Valley is relatively low and ranges between 600 and 800 m above sea level. Many wild animals live near the Albert Nile in the western part of Amuru and Nwoya Districts and near the Victoria Nile in the southern part of Nwoya District because of a favourable climate. -

UGANDA Landscape Analysis September 2016
Integrating Gender and Nutrition within Agricultural Extension Services UGANDA Landscape Analysis September 2016 Source: Bobby Neptune (www.feedthefuture.gov) Uganda Landscape Analysis © INGENAES This work is licensed under a Creative Commons Attribution 3.0 Unported License. Users are free: • To share — to copy, distribute and transmit the work. (without participant contact information) • To remix — to adapt the work. Under the following conditions: • Attribution — users must attribute the work to the authors but not in any way that suggests that the authors endorse the user or the user’s use of the work. Technical editing and production by Joyous Tata and Amanda Childress-Kannan. This report was produced as part of the United States Agency for International Development (USAID) and US Government Feed the Future project “Integrating Gender and Nutrition within Extension and Advisory Services” (INGENAES). www.ingenaes.illinois.edu Leader with Associates Cooperative Agreement No. AID-OAA-LA-14-00008. The report was made possible by the generous support of the American people through USAID. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States government. Uganda Landscape Analysis UGANDA Landscape Analysis First Edition published in September, 2016 Prepared by: Michael Wallace, University of California, Davis Uganda Landscape Analysis Acronyms AERC African Economic Research Consortium ACDI Agricultural Cooperative Development International AGRUFIN Agriculture and Rural Finance