Guidelines for Biological Treatment of Schizophrenia, Part 2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 De Juan Et Al
US 200601 10428A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 de Juan et al. (43) Pub. Date: May 25, 2006 (54) METHODS AND DEVICES FOR THE Publication Classification TREATMENT OF OCULAR CONDITIONS (51) Int. Cl. (76) Inventors: Eugene de Juan, LaCanada, CA (US); A6F 2/00 (2006.01) Signe E. Varner, Los Angeles, CA (52) U.S. Cl. .............................................................. 424/427 (US); Laurie R. Lawin, New Brighton, MN (US) (57) ABSTRACT Correspondence Address: Featured is a method for instilling one or more bioactive SCOTT PRIBNOW agents into ocular tissue within an eye of a patient for the Kagan Binder, PLLC treatment of an ocular condition, the method comprising Suite 200 concurrently using at least two of the following bioactive 221 Main Street North agent delivery methods (A)-(C): Stillwater, MN 55082 (US) (A) implanting a Sustained release delivery device com (21) Appl. No.: 11/175,850 prising one or more bioactive agents in a posterior region of the eye so that it delivers the one or more (22) Filed: Jul. 5, 2005 bioactive agents into the vitreous humor of the eye; (B) instilling (e.g., injecting or implanting) one or more Related U.S. Application Data bioactive agents Subretinally; and (60) Provisional application No. 60/585,236, filed on Jul. (C) instilling (e.g., injecting or delivering by ocular ion 2, 2004. Provisional application No. 60/669,701, filed tophoresis) one or more bioactive agents into the Vit on Apr. 8, 2005. reous humor of the eye. Patent Application Publication May 25, 2006 Sheet 1 of 22 US 2006/0110428A1 R 2 2 C.6 Fig. -

Enhancement of Acetylcholinesterase Inhibitory Activity for the Soft Coral Associated Fungus Aspergillus Unguis SPMD-EGY by Media Composition
Int. J. Pharm. Sci. Rev. Res., 41(2), November - December 2016; Article No. 64, Pages: 349-357 ISSN 0976 – 044X Research Article Enhancement of Acetylcholinesterase Inhibitory Activity for the Soft Coral Associated Fungus Aspergillus unguis SPMD-EGY by Media Composition Faten K. Abd El-Hady1*, Mohamed S. Abdel-Aziz2, Ahmed M.A. Souleman3, Zeinab A. El-Shahid1, Kamel H. Shaker4 1Chemistry of Natural Products Department, National Research Center, Egypt. 2Department of Microbial Chemistry, National Research Center, Egypt. 3Department of Phytochemistry and Plant Systematic, National Research Center, Egypt. 4Chemistry of Natural Compounds Department, National Research Center, Egypt. *Corresponding author’s E-mail: [email protected] Accepted on: 24-09-2016; Finalized on: 30-11-2016. ABSTRACT The soft coral fungus, Aspergillus unguis SPMD-EGY, was grown on different media to select the potential medium producing significant high acetyl-cholinesterase (AChE) inhibitory activity. Extract from Rice solid medium exhibited the highest inhibitory activity of AChE followed by PYMG medium in static conditions (culture filtrate and mycelia). Potato dextrose broth (PD) showed no AChE inhibitory activity but moderate activity was found with DOX broth medium under static conditions (culture filtrate and mycelia). Comparative study has been done for PYMG medium and our previous work. The chemical composition of the potent extracts was evaluated using GC/MS analysis. Rice solid medium extract (RS, 89% AChE inhibitory activity) solely contains nitrogenous compounds, fatty acids and their esters. PYMG medium(PY, 85% activity) showed the presence of two major compounds: 1,3-bis[2-hydroxyphenyl]-2-propen-1-one (33.6%) and D-friedoolean-14-en-3-one (39.8%), mild presence for the compounds 1,6,7-trimethyl-3-phenyl-9H-xanthen-9-one (3%) and 2,4,4’-trihydroxy-chalcone (3.2%). -

Comprehensive Review on the Interaction Between Natural Compounds and Brain Receptors: Benefits and Toxicity
European Journal of Medicinal Chemistry 174 (2019) 87e115 Contents lists available at ScienceDirect European Journal of Medicinal Chemistry journal homepage: http://www.elsevier.com/locate/ejmech Review article Comprehensive review on the interaction between natural compounds and brain receptors: Benefits and toxicity * Ana R. Silva a, Clara Grosso b, , Cristina Delerue-Matos b,Joao~ M. Rocha a, c a Centre of Molecular and Environmental Biology (CBMA), Department of Biology (DB), University of Minho (UM), Campus Gualtar, P-4710-057, Braga, Portugal b REQUIMTE/LAQV, Instituto Superior de Engenharia do Instituto Politecnico do Porto, Rua Dr. Antonio Bernardino de Almeida, 431, P-4249-015, Porto, Portugal c REQUIMTE/LAQV, Grupo de investigaçao~ de Química Organica^ Aplicada (QUINOA), Laboratorio de polifenois alimentares, Departamento de Química e Bioquímica (DQB), Faculdade de Ci^encias da Universidade do Porto (FCUP), Rua do Campo Alegre, s/n, P-4169-007, Porto, Portugal article info abstract Article history: Given their therapeutic activity, natural products have been used in traditional medicines throughout the Received 6 December 2018 centuries. The growing interest of the scientific community in phytopharmaceuticals, and more recently Received in revised form in marine products, has resulted in a significant number of research efforts towards understanding their 10 April 2019 effect in the treatment of neurodegenerative diseases, such as Alzheimer's (AD), Parkinson (PD) and Accepted 11 April 2019 Huntington (HD). Several studies have shown that many of the primary and secondary metabolites of Available online 17 April 2019 plants, marine organisms and others, have high affinities for various brain receptors and may play a crucial role in the treatment of diseases affecting the central nervous system (CNS) in mammalians. -

NIDA Drug Supply Program Catalog, 25Th Edition
RESEARCH RESOURCES DRUG SUPPLY PROGRAM CATALOG 25TH EDITION MAY 2016 CHEMISTRY AND PHARMACEUTICS BRANCH DIVISION OF THERAPEUTICS AND MEDICAL CONSEQUENCES NATIONAL INSTITUTE ON DRUG ABUSE NATIONAL INSTITUTES OF HEALTH DEPARTMENT OF HEALTH AND HUMAN SERVICES 6001 EXECUTIVE BOULEVARD ROCKVILLE, MARYLAND 20852 160524 On the cover: CPK rendering of nalfurafine. TABLE OF CONTENTS A. Introduction ................................................................................................1 B. NIDA Drug Supply Program (DSP) Ordering Guidelines ..........................3 C. Drug Request Checklist .............................................................................8 D. Sample DEA Order Form 222 ....................................................................9 E. Supply & Analysis of Standard Solutions of Δ9-THC ..............................10 F. Alternate Sources for Peptides ...............................................................11 G. Instructions for Analytical Services .........................................................12 H. X-Ray Diffraction Analysis of Compounds .............................................13 I. Nicotine Research Cigarettes Drug Supply Program .............................16 J. Ordering Guidelines for Nicotine Research Cigarettes (NRCs)..............18 K. Ordering Guidelines for Marijuana and Marijuana Cigarettes ................21 L. Important Addresses, Telephone & Fax Numbers ..................................24 M. Available Drugs, Compounds, and Dosage Forms ..............................25 -

Implications of Dopamine D3 Receptor for Glaucoma: In-Silico and In-Vivo Studies
International PhD Program in Neuropharmacology XXVI Cycle Implications of dopamine D3 receptor for glaucoma: in-silico and in-vivo studies PhD thesis Chiara Bianca Maria Platania Coordinator: Prof. Salvatore Salomone Tutor: Prof. Claudio Bucolo Department of Clinical and Molecular Biomedicine Section of Pharmacology and Biochemistry. University of Catania - Medical School December 2013 Copyright ©: Chiara B. M. Platania - December 2013 2 TABLE OF CONTENTS ACKNOWLEDGEMENTS............................................................................ 4 LIST OF ABBREVIATIONS ........................................................................ 5 ABSTRACT ................................................................................................... 7 GLAUCOMA ................................................................................................ 9 Aqueous humor dynamics .................................................................. 10 Pharmacological treatments of glaucoma............................................ 12 Pharmacological perspectives in treatment of glaucoma ..................... 14 Animal models of glaucoma ............................................................... 18 G PROTEIN COUPLED RECEPTORS ....................................................... 21 GPCRs functions and structure ........................................................... 22 Molecular modeling of GPCRs ........................................................... 25 D2-like receptors ............................................................................... -

The Effects of Donepezil, an Acetylcholinesterase Inhibitor, on Impaired Learning and Memory in Rodents
Original Article Biomol Ther 26(3), 274-281 (2018) The Effects of Donepezil, an Acetylcholinesterase Inhibitor, on Impaired Learning and Memory in Rodents Chang Yell Shin1,2, HaeSun Kim1, KwangHo Cha1, Dong Han Won1, JiYun Lee2, Sun Woo Jang1,* and Uy Dong Sohn2,* 1Research Institute of Dong-A ST Co., Ltd., Yongin 17073, 2College of Pharmacy, Chung-Ang University, Seoul 06974, Republic of Korea Abstract A previous study in humans demonstrated the sustained inhibitory effects of donepezil on acetylcholinesterase (AChE) activity; however, the effective concentration of donepezil in humans and animals is unclear. This study aimed to characterize the effective concentration of donepezil on AChE inhibition and impaired learning and memory in rodents. A pharmacokinetic study of done- pezil showed a mean peak plasma concentration of donepezil after oral treatment (3 and 10 mg/kg) of approximately 1.2 ± 0.4 h and 1.4 ± 0.5 h, respectively; absolute bioavailability was calculated as 3.6%. Further, AChE activity was inhibited by increasing plasma concentrations of donepezil, and a maximum inhibition of 31.5 ± 5.7% was observed after donepezil treatment in hairless rats. Plasma AChE activity was negatively correlated with plasma donepezil concentration. The pharmacological effects of done- pezil are dependent upon its concentration and AChE activity; therefore, we assessed the effects of donepezil on learning and memory using a Y-maze in mice. Donepezil treatment (3 mg/kg) significantly prevented the progression of scopolamine-induced memory impairment in mice. As the concentration of donepezil in the brain increased, the recovery of spontaneous alternations also improved; maximal improvement was observed at 46.5 ± 3.5 ng/g in the brain. -
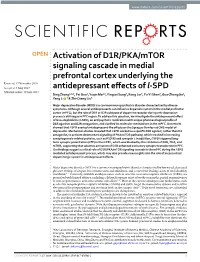
Activation of D1R/PKA/Mtor Signaling Cascade in Medial
www.nature.com/scientificreports OPEN Activation of D1R/PKA/mTOR signaling cascade in medial prefrontal cortex underlying the Received: 17 November 2016 Accepted: 3 May 2017 antidepressant effects ofl -SPD Published: xx xx xxxx Bing Zhang1,2,3, Fei Guo1, Yuqin Ma1,2, Yingcai Song3, Rong Lin3, Fu-Yi Shen3, Guo-Zhang Jin1, Yang Li 1 & Zhi-Qiang Liu3 Major depressive disorder (MDD) is a common neuropsychiatric disorder characterized by diverse symptoms. Although several antidepressants can influence dopamine system in the medial prefrontal cortex (mPFC), but the role of D1R or D2R subtypes of dopamine receptor during anti-depression process is still vague in PFC region. To address this question, we investigate the antidepressant effect of levo-stepholidine (l-SPD), an antipsychotic medication with unique pharmacological profile of D1R agonism and D2R antagonism, and clarified its molecular mechanisms in the mPFC. Our results showed that l-SPD exerted antidepressant-like effects on the Sprague-Dawley rat CMS model of depression. Mechanism studies revealed that l-SPD worked as a specific D1R agonist, rather than D2 antagonist, to activate downstream signaling of PKA/mTOR pathway, which resulted in increasing synaptogenesis-related proteins, such as PSD 95 and synapsin I. In addition, l-SPD triggered long- term synaptic potentiation (LTP) in the mPFC, which was blocked by the inhibition of D1R, PKA, and mTOR, supporting that selective activation of D1R enhanced excitatory synaptic transduction in PFC. Our findings suggest a critical role of D1R/PKA/mTOR signaling cascade in the mPFC during thel -SPD mediated antidepressant process, which may also provide new insights into the role of mesocortical dopaminergic system in antidepressant effects. -

Download PDF (131K)
doi: 10.2169/internalmedicine.6261-20 Intern Med 60: 2251-2254, 2021 http://internmed.jp 【 CASE REPORT 】 Cholinergic Crisis Owing to Distigmine Bromide Complicated by Hyperosmolar Hyperglycemic State Kazumasa Kotake 1, Atsuhito Tone 2, Satoko Watanabe 2, Mayumi Senoo 2, Mitsuhiro Kaneto 2, Yusuke Imai 2, Sanae Teshigawara 2, Yasuhiro Kawakami 1 and Tatsuaki Nakatou 2 Abstract: Distigmine bromide is widely used to treat neurogenic bladder and causes cholinergic crisis, a serious side effect. We herein report about a patient with distigmine bromide-induced cholinergic crisis complicated by a hyperosmolar hyperglycemic state (HHS). On admission, the patient was diagnosed with HHS based on the medical history and laboratory test results. However, she also had bradycardia, miosis, and low plasma cholinesterase activity. We later found that she had received distigmine bromide, which led to a diagnosis of cholinergic crisis. We suggest that the exacerbation of pathology, including HHS, can cause cholinergic crisis in patients receiving distigmine bromide. Key words: distigmine bromide, cholinergic crisis, hyperosmolar hyperglycemic state, bradycardia, miosis, low plasma cholinesterase activity (Intern Med 60: 2251-2254, 2021) (DOI: 10.2169/internalmedicine.6261-20) ness. Her activities of daily living required full assistance, Introduction and her food intake had been gradually decreasing for the preceding few days; however, her condition worsened after Distigmine bromide is classified as a cholinesterase in- lunch on the day of admission. She had a history of type 2 hibitor and is used for the treatment of underactive neuro- diabetes, hypertension, dementia, neurogenic bladder, cata- genic bladder. In older adults, detrusor contractility, urine ract, angina, Meniere’s disease, disc herniation, and colorec- flow, and bladder sensation are significantly reduced. -

(12) Patent Application Publication (10) Pub. No.: US 2006/0058336A1 Nakanishi Et Al
US 20060058336A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2006/0058336A1 Nakanishi et al. (43) Pub. Date: Mar. 16, 2006 (54) PHARMACEUTICAL COMPOSITION FOR Publication Classification TREATMENT OF DRUG DEPENDENCE (51) Int. Cl. (76) Inventors: Shigetada Nakanishi, Kyoto-shi (JP); A6IK 31/4745 (2006.01) Takatoshi Hikida, Baltimore, MD A6IK 31/473 (2006.01) (US); Ira Pastan, Potomac, MD (US) A6IK 31/47 (2006.01) C d Add A6IK 31/4178 (2006.01) orrespondence Address: A6IK 31/407 (2006.01) BRCH STEWART KOLASCH & BRCH (52) U.S. Cl. ......................... 514/297; 514/310; 514/397; PO BOX 747 514/411 FALLS CHURCH, VA 22040-0747 (US) (21)21) AppAppl. No.: 10/493,4889 (57) ABSTRACT (22) PCT Filed: Feb. 26, 2004 (86) PCT No.: PCT/P04/02301 The present invention relates to the use of a medicinal Substance capable of enhancing or disinhibiting the actions Related U.S. Application Data of acetylcholine, and provides a pharmaceutical composition for treating drug dependence comprising Said Substance as (60) Provisional application No. 60/449,868, filed on Feb. an active ingredient, and a method of treating drug depen 27, 2003. dence using the Same. Patent Application Publication Mar. 16, 2006 Sheet 1 of 7 US 2006/0058336A1 Fig 1 ÁeM??edö?6Jau?uedopo?quu??osºuu9ul y--No.````*auquedoqbº O\/]LIA}} C?ksne10nN suequunooe eu||0?.0|Á?90W Patent Application Publication Mar. 16, 2006 Sheet 2 of 7 US 2006/0058336A1 Fig 2 Before After conditioningBefore conditioningAfter conditioning conditioning 8 O 500 6 O O 4. O -50 O 2 O O -1000 O -15 a T-tg F. -

Biol. Pharm. Bull. 42(7): 1064-1068 (2019)
1064 Biol. Pharm. Bull. 42, 1064–1068 (2019) Vol. 42, No. 7 Review Effects of Distigmine on the Mechanical Activity of Urinary Bladder Smooth Muscle Keisuke Obara* and Yoshio Tanaka Department of Chemical Pharmacology, Faculty of Pharmaceutical Sciences, Toho University; 2–2–1 Miyama, Funabashi, Chiba 274–8510, Japan. Received February 28, 2019; accepted April 24, 2019 Distigmine bromide (distigmine) is a reversible carbamate cholinesterase (ChE) inhibitor. Its principle clinical application is in the treatment of myasthenia gravis. Distigmine is also used as a remedy for dysuria and glaucoma. Its effectiveness in the management of dysuria has been demonstrated in several clinical re- ports. Distigmine may improve (enhance) urinary bladder smooth muscle (UBSM) contraction during mic- turition by inhibiting acetylcholine (ACh) decomposition. However, the pharmacological effects of distigmine on UBSM have not been adequately studied so far. In this review article, we summarize the reported effects of distigmine on the contractile responses elicited by exogenous and endogenous ACh in isolated UBSM preparations. We also discuss the effects of distigmine on the UBSM basal tone and the contractile response of UBSM to ATP, which is co-released with ACh from parasympathetic nerve terminals. Key words distigmine bromide; urinary bladder smooth muscle; cholinesterase inhibitor; acetylcholine; adenosine triphosphate 1. INTRODUCTION 2. EFFECTS OF DISTIGMINE ON UBSM CONTRAC- TILE RESPONSES ELICITED BY EXOGENOUS CON- Distigmine bromide (distigmine) -

12.2% 122,000 135M Top 1% 154 4,800
View metadata, citation and similar papers at core.ac.uk brought to you by CORE We are IntechOpen, provided by IntechOpen the world’s leading publisher of Open Access books Built by scientists, for scientists 4,800 122,000 135M Open access books available International authors and editors Downloads Our authors are among the 154 TOP 1% 12.2% Countries delivered to most cited scientists Contributors from top 500 universities Selection of our books indexed in the Book Citation Index in Web of Science™ Core Collection (BKCI) Interested in publishing with us? Contact [email protected] Numbers displayed above are based on latest data collected. For more information visit www.intechopen.com Chapter Anticholinesterases Zeynep Özdemir and Mehmet Abdullah Alagöz Abstract Acetylcholinesterase (AChE) and butyrylcholinesterase (BChE) are known serine hydrolase enzymes responsible for the hydrolysis of acetylcholine (ACh). Although the role of AChE in cholinergic transmission is well known, the role of BChE has not been elucidated sufficiently. The hydrolysis of acetylcholine in the synaptic healthy brain cells is mainly carried out by AChE; it is accepted that the contribution to the hydrolysis of BChE is very low, but both AChE and BChE are known to play an active role in neuronal development and cholinergic transmission. Myasthenia gravis (MG) is a muscle disease characterized by weakness in skeletal muscles and rapid fatigue. Anticholinesterases, which are not only related to the immune origin of the disease but also have only symp- tomatic benefit, have an indispensable role in the treatment of MG. Pyridostigmine, distigmine, neostigmine, and ambenonium are the standard anticholinesterase drugs used in the symptomatic treatment of MG. -
Handbook of Schizophrenia Spectrum Disorders, Volume III
Handbook of Schizophrenia Spectrum Disorders, Volume III Michael S. Ritsner Editor Handbook of Schizophrenia Spectrum Disorders, Volume III Therapeutic Approaches, Comorbidity, and Outcomes 123 Editor Michael S. Ritsner Technion – Israel Institute of Technology Rappaport Faculty of Medicine Haifa Israel [email protected] ISBN 978-94-007-0833-4 e-ISBN 978-94-007-0834-1 DOI 10.1007/978-94-007-0834-1 Springer Dordrecht Heidelberg London New York Library of Congress Control Number: 2011924745 © Springer Science+Business Media B.V. 2011 No part of this work may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, microfilming, recording or otherwise, without written permission from the Publisher, with the exception of any material supplied specifically for the purpose of being entered and executed on a computer system, for exclusive use by the purchaser of the work. Printed on acid-free paper Springer is part of Springer Science+Business Media (www.springer.com) Foreword Schizophrenia Spectrum Disorders: Insights from Views Across 100 years Schizophrenia spectrum and related disorders such as schizoaffective and mood dis- orders, schizophreniform disorders, brief psychotic disorders, delusional and shared psychotic disorders, and personality (i.e., schizotypal, paranoid, and schizoid per- sonality) disorders are the most debilitating forms of mental illness, worldwide. There are 89,377 citations (including 10,760 reviews) related to “schizophrenia” and 2118 (including 296 reviews) related to “schizophrenia spectrum” in PubMed (accessed on August 12, 2010). The classification of these disorders, in particular, of schizophrenia, schizoaf- fective and mood disorders (referred to as functional psychoses), has been debated for decades, and its validity remains controversial.