The Haiti Neglected Tropical Diseases (Ntds) Control Program Work Plan and Budget for IMA/RTI Program Year Five October 1, 2010-September 30, 2011
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Electoral Observations in the Americas Series, No
Electoral Observations in the Americas Series, No. 28 Electoral Observation in Haiti Legislative, Municipal, and Local Elections February to July 2000 Secretary General César Gaviria Assistant Secretary General Luigi R. Einaudi Executive Coordinator, Unit for the Promotion of Democracy Elizabeth M. Spehar Electoral Observation in Haiti: legislative, municipal, and local elections, February to July, 2000 / Unit for the Promotion of Democracy. p. ; cm. - (Electoral Observations in the Americas series, no. 28) ISBN 0-8270-4331-7 1. Elections--Haiti. 2. Election monitoring--Haiti. I. Organization of American States. Unit for the Promotion of Democracy. II. Series. OEA/Ser.D/XX SG/UPD/II.28 (E) This publication is part of a series of UPD publications of the General Secretariat of the Organization of American States. The ideas, thoughts, and opinions expressed are not necessarily those of the OAS or its member states. The opinions expressed are the responsibility of the authors. OEA/Ser.D/XX SG/UPD/II.28 13 December 2000 Original: French Electoral Observation in Haiti Legislative, Municipal, and Local Elections February to July 2000 General Secretariat Organization of American States Washington, D.C. 20006 2001 This report was produced under the technical supervision of Orlando Marville, Chief of the Mission, Special Advisor of the Unit for the Promotion of Democracy, and with the assistance of Steve Griner, Deputy Chief of the Mission and, Senior Specialist of the Unit for the Promotion of Democracy (UPD). Design and composition of this publication was done by the Information and Dialogue Section of the UPD, headed by Caroline Murfitt- Eller. Kathryn Stafford helped with the editorial review of this report and Esther Rodriguez with its production. -

USAID/OFDA Haiti Earthquake Program Maps 6/4/2010
EARTHQUAKE-AFFECTED AREAS AND POPULATION MOVEMENT IN HAITI CUBAEARTHQUAKE INTENSITY 73° W 72° W The Modified Mercalli (MMI) Intensity Scale* NORTHWESTNORTHWEST Palmiste N N 20° NORTHWEST 20° ESTIMATED MMI INTENSITY Port-de-Paix 45,862 Saint Louis Du Nord LIGHT SEVERE 4 8 Anse-a-foleur NORTH Jean Rabel 13,531 Monte Cristi 5 MODERATE 9 VIOLENT Le Borgne NORTHWESTNORTHWEST Cap-Haitien NORTHEAST 6 STRONG 10^ EXTREME Bassin-bleu Port-margot Quartier 8,500 Limbe Marin Caracol 7 VERY STRONG Baie-de-Henne Pilate Acul Plaine Phaeton Anse Rouge Gros Morne Limonade Fort-Liberte *MMI is a measure of ground shaking and is different Du Nord Du Nord from overall earthquake magnitude as measured Plaisance Trou-du-nord NORTHNORTH Milot Ferrier by the Richter Scale. Terre-neuve Sainte Suzanne ^Area shown on map may fall within MMI 9 Dondon Grande Riviera Quanaminthe classification, but constitute the areas of heaviest Dajabon ARTIBONITE Du Nord Perches shaking based on USGS data. Marmelade 162,509 Gonaives Bahon Source: USGS/PAGER Alert Version: 8 Ennery Saint-raphael NORTHEASTNORTHEAST HAITI EARTHQUAKE Vallieres Ranguitte Saint Michel Mont Organise 230,000 killed ARTIBONITEARTIBONITE De L'attalaye Pignon 196,595 injured La Victoire POPULATION MOVEMENT * 1,200,000 to 1,290,000 displaced CENTER Source: OCHA 02.22.10 Dessalines Cerca 3,000,000 affected Grande-Saline 90,997Carvajal * Population movements indicated include only Maissade Cerca-la-source individuals utilizing GoH-provided transportation *All figures are approximate. Commune Petite-riviere- Hinche and do not include people leaving Port-au-Prince population figures are as of 2003. de-l'artibonite utilizing private means of transport. -

United Nations Development Programme Country: Haiti PROJECT DOCUMENT
United Nations Development Programme Country: Haiti PROJECT DOCUMENT Project Title: Increasing resilience of ecosystems and vulnerable communities to CC and anthropic threats through a ridge to reef approach to BD conservation and watershed management ISF Outcome: 2.2: environmental vulnerability reduced and ecological potential developed for the sustainable management of natural and energy resources based on a decentralised territorial approach UNDP Strategic Plan Environment and Sustainable Development Primary Outcome: 3: mechanisms for climate change adaptation are in place Expected CP Outcomes: See ISF outcome Expected CPAP Output (s) 1. Priority watersheds have increased forest cover 2. National policies and plans for environmental and natural resource management integrating a budgeted action plan are validated 3. Climate change adaptation mechanisms are put in place. Executing Entity/Implementing Partner: Ministry of Environment Implementing Entity/Responsible Partners: United Nations Development Programme Brief Description This project will deliver help to reduce the vulnerability of poor people in Haiti to the effects of climate change, while at the same time conserving threatened coastal and marine biodiversity. Investments in climate- proofed and socially-sustainable BD conservation strategies, within the context of the National Protected Areas System (NPAS), will enable coastal and marine ecosystems to continue to generate Ecosystem-Based Adaptation (EBA) services; while additional investment of adaptation funds in the watersheds -

Focus on Haiti
FOCUS ON HAITI CUBA 74o 73o 72o ÎLE DE LA TORTUE Palmiste ATLANTIC OCEAN 20o Canal de la Tortue 20o HAITI Pointe Jean-Rabel Port-de-Paix St. Louis de Nord International boundary Jean-Rabel Anse-à-Foleur Le Borgne Departmental boundary Monte Cap Saint-Nicolas Môle St.-Nicolas National capital Bassin-Bleu Baie de Criste NORD - OUEST Port-Margot Cap-Haïtien Mancenille Departmental seat Plaine Quartier Limbé du Nord Caracol Fort- Town, village Cap-à-Foux Bombardopolis Morin Liberté Baie de Henne Gros-Morne Pilate Acul Phaëton Main road Anse-Rouge du Nord Limonade Baie Plaisance Milot Trou-du-Nord Secondary road de Grande Terre-Neuve NORD Ferrier Dajabón Henne Pointe Grande Rivière du Nord Sainte Airport Suzanne Ouanaminthe Marmelade Dondon Perches Ennery Bahon NORD - EST Gonaïves Vallières 0 10 20 30 40 km Baie de Ranquitte la Tortue ARTIBONITE Saint- Raphaël Mont-Organisé 0 5 10 15 20 25 mi Pointe de la Grande-Pierre Saint Michel Baie de de l'Attalaye Pignon La Victoire Golfe de la Gonâve Grand-Pierre Cerca Carvajal Grande-Saline Dessalines Cerca-la-Source Petite-Rivière- Maïssade de-l'Artibonite Hinche Saint-Marc Thomassique Verrettes HAITI CENTRE Thomonde 19o Canal de 19o Saint-Marc DOMINICAN REPUBLIC Pointe Pointe de La Chapelle Ouest Montrouis Belladère Magasin Lac de ÎLE DE Mirebalais Péligre LA GONÂVE Lascahobas Pointe-à-Raquette Arcahaie Saut-d'Eau Baptiste Duvalierville Savenette Abricots Pointe Cornillon Jérémie ÎLES CAYÉMITES Fantasque Trou PRESQU'ÎLE Thomazeau PORT- É Bonbon DES BARADÈRES Canal de ta AU- Croix des ng Moron S Dame-Marie la Gonâve a Roseaux PRINCE Bouquets u Corail Gressier m Chambellan Petit Trou de Nippes â Pestel tr Carrefour Ganthier e Source Chaude Baradères Anse-à-Veau Pétion-Ville Anse d'Hainault Léogâne Fond Parisien Jimani GRANDE - ANSE NIPPES Petite Rivières Kenscoff de Nippes Miragoâne Petit-Goâve Les Irois Grand-Goâve OUEST Fonds-Verrettes L'Asile Trouin La Cahouane Maniche Camp-Perrin St. -

Assessment of Haitian Coffee Value Chain
Assessment of Haitian Coffee Value Chain Fernando Rodríguez, Nora Patricia Castañeda, Mark Lundy A participatory assessment of coffee chain actors in southern Haiti assessment Copyright © 2011 Catholic Relief Services Catholic Relief Services 228 West Lexington Street Baltimore, MD 21201-3413 USA Cover photo: Coffee plants in Haiti. CRS staff. Download this and other CRS publications at www.crsprogramquality.org Assessment of HAitiAn Coffee VAlue Chain A participatory assessment of coffee chain actors in southern Haiti July 12–August 30, 2010 Table of Contents Abbreviations and Acronyms . iii 1 Executive Summary. IV 2 Introduction. 1 3 Relevance of Coffee in Haiti. 1 4 Markets . 4 5 Coffee Chain Analysis. 5 6 Constraints Analyses. 17 7 Recommendations . 19 Glossary . 22 References . 24 Annexes . 25 Annex 1: Problem Tree. 25 Annex 2: Production Solution Tree. 26 Annex 3: Postharvest Solution Tree . 27 Annex 4: Marketing Solution Tree. 28 Annex 5: Conclusions Obtained with Workshops Participants. 29 Figures Figure 1: Agricultural sector participation in total GDP. 1 Figure 2: Coffee production. 3 Figure 3: Haitian coffee exports. 4 Figure 4: Coffee chain in southern Haiti. 6 Figure 5: Potential high-quality coffee municipalities in Haiti. 9 Tables Table 1: Summary of chain constraints and strategic objectives to address them. IV Table 2: Principal coffee growing areas and their potential to produce quality coffee. 2 Table 3: Grassroots organizations and exporting regional networks. 3 Table 4: Land distribution by plot size . 10 Table 5: Coffee crop area per department in 1995 . 10 Table 6: Organizations in potential high-quality coffee municipalities. 12 Table 7: Current and potential washed coffee production in the region . -

WFP News Video: Haiti November 2019
WFP News Video: Haiti November 2019 Location: Gonaives, Chansolme, Nord-Ouest department, Port au Prince Haiti Shot: 23rd, 25th – 26th, 29th November 2019 TRT: 03:12 Shotlist :00-:07 GV’s trash covered streets in Gonaives. Gonaives, Haiti Shot: 26 Nov 2019 :07-:26 Shots of health centre waiting room. Nutritionist Myriam Dumerjusten attends to 25 year-old mother of four Alectine Michael and checks her youngest child, 8 month-old Jacqueline for malnutrition. Gonaives, Haiti Shot: 26 Nov 2019 :26-:30 SOT Nutritionist Myriam Dumerjusten (French) “It’s a lack of food and a lack of economic means.” Gonaives, Haiti Shot: 26 Nov 2019 :30-:40 A convoy of 9 WFP trucks carry emergency food for a distribution to vulnerable people living in a remote rural area in Haiti Nord-Ouest department. The department is considered one of the most food insecure in the country according to a recent government study. Trucks arrive in Chansolme’s school compound where a large crowd awaits for the food distribution. Nord-Ouest department, Haiti Shot: 23 Nov 2019 :40-:52 Via Cesare Giulio Viola 68/70, 00148 Rome, Italy | T +39 06 65131 F +39 06 6590 632/7 WFP food is off-loaded from the trucks and organised by WFP staff to facilitate the distribution by groups of 4 people. Chansolme, Nord-Ouest department Shot: 23 Nov 2019 :52-1:07 People line up to confirm their ID before distribution. Priority is given to elderly people, pregnant women and handicapped who will be the first in line to receive the food assistance. -
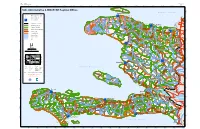
")Un ")Un ")Un ")Un ")Un ")Un ")Un ")Un ")Un ")Un
HAITI: 1:900,000 Map No: ADM 012 Stock No: M9K0ADMV0712HAT22R Edition: 2 30' 74°20'0"W 74°10'0"W 74°0'0"W 73°50'0"W 73°40'0"W 73°30'0"W 73°20'0"W 73°10'0"W 73°0'0"W 72°50'0"W 72°40'0"W 72°30'0"W 72°20'0"W 72°10'0"W 72°0'0"W 71°50'0"W 71°40'0"W N o r d O u e s t N " 0 Haiti: Administrative & MINUSTAH Regional Offices ' 0 La Tortue ! ° 0 N 2 " (! 0 ' A t l a n t i c O c e a n 0 ° 0 2 Port de Paix \ Saint Louis du Nord !( BED & Department Capital UN ! )"(!\ (! Paroli !(! Commune Capital (!! ! ! Chansolme (! ! Anse-a-Foleur N ( " Regional Offices 0 UN Le Borgne ' 0 " ! 5 ) ! ° N Jean Rabel " ! (! ( 9 1 0 ' 0 5 ° Mole St Nicolas Bas Limbe 9 International Boundary 1 (!! N o r d O u e s t (!! (!! Department Boundary Bassin Bleu UN Cap Haitian Port Margot!! )"!\ Commune Boundary ( ( Quartier Morin ! N Commune Section Boundary Limbe(! ! ! Fort Liberte " (! Caracol 0 (! ' ! Plaine 0 Bombardopolis ! ! 4 Pilate ° N (! ! ! " ! ( UN ( ! ! Acul du Nord du Nord (! 9 1 0 Primary Road Terrier Rouge ' (! (! \ Baie de Henne Gros Morne Limonade 0 )"(! ! 4 ! ° (! (! 9 Palo Blanco 1 Secondary Road Anse Rouge N o r d ! ! ! Grande ! (! (! (! ! Riviere (! Ferrier ! Milot (! Trou du Nord Perennial River ! (! ! du Nord (! La Branle (!Plaisance ! !! Terre Neuve (! ( Intermittent River Sainte Suzanne (!! Los Arroyos Perches Ouanaminte (!! N Lake ! Dondon ! " 0 (! (! ' ! 0 (! 3 ° N " Marmelade 9 1 0 ! ' 0 Ernnery (!Santiag o \ 3 ! (! ° (! ! Bahon N o r d E s t de la Cruz 9 (! 1 ! LOMA DE UN Gonaives Capotille(! )" ! Vallieres!! CABRERA (!\ (! Saint Raphael ( \ ! Mont -
Using Behavioral Insights to Improve Disaster Preparedness, Early
Public Disclosure Authorized USING BEHAVIORAL INSIGHTS TO IMPROVE DISASTER Public Disclosure Authorized PREPAREDNESS, EARLY WARNING AND RESPONSE MECHANISMS IN HAITI Public Disclosure Authorized Public Disclosure Authorized CONTENTS 1 Introduction 6 2 Methodology and description of data 9 3 Background and Context 13 4 Disaster Risk Management in Haiti 20 4.1 Operating model 20 4.2 Roles and key actors 22 4.3 Preparedness process 22 4.4 Communication channels 23 4.5 Evacuation process 23 5 Key Insights on Barriers to Evacuation 25 5.1 Obstacle 1: EWS Messages Do Not Arrive 25 5.2 Obstacle 2: People Do Not Understand EWS Messages 27 5.3 Obstacle 3: People Struggle to Internalize Risk 29 5.4 Obstacle 4: People Lack Access to Resources and Shelters to Evacuate 30 5.5 Obstacle 5: People Prefer Not to Evacuate 30 6 Ideas to Nudge People to Evacuate to A Safe Place on Time 34 7 Conclusion 39 Bibliography 41 Appendix 1 – Field Study Methodology and Diagnostic Activities 43 Appendix 2 – Hurricane classification 45 ACKNOWLEDGEMENTS his report was prepared by a World Bank team composed of Jime- na Llopis (Behavioral Scientist, Poverty & Equity GP), Emilie Perge T (Economist, Poverty & Equity GP), Zeina Afif (Senior Social Scientist, Poverty & Equity GP), Claudia Soto Orozco (Disaster Risk Management Spe- cialist, Social, Urban Rural and Resilience GP), Lace Padilla (Consultant, Pov- erty & Equity GP), Jessica Hsu (Consultant, Poverty & Equity GP) with inputs from Cecile Lorillou (Consultant, Social, Urban Rural and Resilience GP); Ali Alwahti (Consultant, Social, Urban Rural and Resilience GP), Roland Brad- shaw (Senior Disaster Risk Management Specialist, Social, Urban Rural and Resilience GP), and Giovanni Michele Toglia (Consultant, Social, Urban Rural and Resilience GP) with overall guidance from Oscar Calvo-Gonzalez (Prac- tice Manager, Poverty & Equity GP), Raju Singh (Program Leader, LCC8C), and Pierre-Xavier Bonneau (Program Leader, LCC8C). -

Haiti Study Abroad 2018 Water, Environmental Issues, and Service Learning May 20 (19 in GR) to June 19
Haiti Study Abroad 2018 Water, Environmental Issues, and Service Learning May 20 (19 in GR) to June 19 May 19th 4-6 pm - Pizza, Packing, and Parents party in Niemeyer MPR. Delta Air Lines 1369 20MAY Grand Rapids / Atlanta 8:10A 10:04A Delta Air Lines 685 20MAY Atlanta / PAP 11:20A-2:32P Delta Air Lines 684 19JUN PAP / Atlanta 3:30P-6:45P Delta Air Lines 1433 19JUN Atlanta / Grand Rapids 9:44P-11:43P OVERVIEW: • Saturday May 19, 4:00-6:00 pm Pizza, Packing, and Parent party Niemeyer Multipurpose Room, parents and friends invited. • Sunday, May 20th 6:00 am meet at Gerald R. Ford (GRR) Airport in Grand Rapids • Sunday, May 20th 8:10 am depart on Delta Flight DL 1369 • May 20th to May 23rd Staying at the Le Plaza Hotel, Port-au-Prince. • May 24th to May 26th Trip to Jacmel staying at Amitie Hotel. • May 27th travel to Deschapelles via PAP and airport stop at Moulin sur Mer museum en- route. • May 27 to June 10 Staying at HAS in Deschapelles, Haiti • June 11 to June 13 at UCI in Central Plateau (Pignon) • June 14 to June 18 in Cap Haitian at Auberge du Picolet Hotel • June 18 travel to PAP and stay at Servotel in Port au Prince • June 19 return flight to GRR FOR EMERGENCY CONTACT: Dr. Peter Wampler, Director ([email protected]): (US) (616) 638-2043 (cell) or (616) 331-2834 (office message) or +509 _____________ (Haiti Cell phone) Kelly McDonell, Assistant Director ([email protected]): (US) 248-459-4063 or (616) 331-8155 (office message) or +509 __________________ (Haiti Cell phone) Elena Selezneva (Padnos International Center) 616-331-3898 Rachel Fort (Hôpital Albert Schweitzer) + 509 3424-0465 (Haiti) [email protected] Leah Steele (Hôpital Albert Schweitzer) + 509 3735-8012 (Haiti) [email protected] Mahamat Koutami Adoum (HAS) + 509 3418-0700 (Haiti) [email protected] US Embassy Duty Officer in Haiti: +509 2229-8000 Boulevard du 15 October Tabarre 41, Route de Tabarre Port au Prince, Haiti Page 1 of 8 Daily Itinerary (subject to change as conditions warrant): Date Activity Contact Saturday, May 19 Pizza, packing, and Dr. -

Post-Disaster Assessment on the Feasibility of Organizing Free and Fair Elections in Haiti
POST-DISASTER ASSESSMENT ON THE FEASIBILITY OF ORGANIZING FREE AND FAIR ELECTIONS IN HAITI Sophie LAGUENY, Chief of Party Rudolf DEROSE, National Consultant March – April 2010 By Sophie Lagueny & Rudolf Dérose This publication was produced by IFES for the U.S. Agency for International Development concerning Associate Cooperative Agreement No. 521-A-00-08-00008-00, under Leader Cooperative Agreement No. DGC-A-00-01-00004-00. The opinions expressed herein are those of the authors and do not necessarily reflect the views of the United States Agency for International Development or the United States Government. Post-Disaster Assessment on the Feasibility of Organizing Free and Fair Elections in Haiti By Sophie Lagueny and Rudolf Dérose March – April 2010 Post-Disaster Assessment on the Feasibility of Organizing Free and Fair Elections in Haiti By Sophie Lagueny and Rudolf Dérose © 2010 by IFES. All rights reserved. IFES 1850 K. Street, Fifth Floor Washington, D.C. 20006 U.S.A. Notice of rights All rights reserved. No part of this report can be reproduced or transmitted in any form by any means without the prior permission of the publisher. Printed in the United States of America. ISBN: 1-931459-50-9 TABLE OF CONTENTS EXECUTIVE SUMMARY i I. MANDATE 1 II. BACKGROUND 1 III. STRATEGY 2 IV. RESULTS OF INTERVIEWS 3 V. ANALYSIS AND POSSIBLE SCENARIOS 4 1) The Terms of Office of the Elected Officials According to the Constitution Of 1987 and Its Provisions 5 2) The Current Status Of The Elected Officials’ Terms Of Office 8 3) Three Possible Scenarios 10 VI. -
Pdf | 332.53 Kb
150 route de Ferney, P.O. Box 2100 1211 Geneva 2, Switzerland Appeal Tel: 41 22 791 6033 Fax: 41 22 791 6506 E-mail: [email protected] Haiti Coordinating Office Emergency Response to Hurricanes Fay, Gustav, Hanna & Ike - LAHT81 Revision 1 Appeal Target: US$ 1,429,428 Balance Requested from ACT Alliance US$ 5,750 Geneva, 15 October 2009 Dear Colleagues, From August 15 to September 8, 2008 all 10 departments of Haiti were hit by 1 or more of 4 tropical storms and hurricanes, namely Fay, Gustav, Hanna and Ike. The damage was extensive. According to the official statistics of October 2008, 793 people were killed, and 310 persons reported missing. Altogether 165,337 families have been affected, 22,702 houses destroyed and 84,625 damaged. School opening which was due on September 8th was postponed by government decree for one month due to complete/partial destruction of school structures, affecting at least 40,000 children. Some schools were used as temporary shelters. Agricultural land and crops were destroyed and a significant amount of livestock lost. Infrastructure, such as water and sanitation, telephone and electrical systems, roads and bridges were damaged making access to many areas impossible and hampering aid efforts, economic activities, access to food and health care. The ACT alliance responded to the disaster as soon as a rapid assessment could be done through a preliminary appeal issued on 10 September 2008. Detailed assessments resulted in the issuing of the full appeal on 11 November 2008. Christian Aid is working together with its partners KORAL and GRAMIR. -
FY21 Q2 Country Updates
Act to End NTDs | East FY21 Q2 Monthly Updates January 1, 2021–March 31, 2021 Cooperative Agreement No. 7200AA18CA00040 Prepared for Rob Henry, AOR Office of Infectious Diseases U.S. Agency for International Development 1300 Pennsylvania Avenue, NW Washington DC, 20532 Prepared by RTI International 3040 Cornwallis Road Post Office Box 12194 Research Triangle Park, NC 27709-2194 Act to End NTDs | East Program Overview The U.S. Agency for International Development Act to End Neglected Tropical Diseases (NTDs) | East Program supports national NTD programs in reaching World Health Organization goals for NTD control and elimination through proven, cost-effective public health interventions. The Act to End NTDs | East (Act | East) Program also provides critical support to countries on their journey to self-reliance, helping them create sustainable programming for NTD control within robust and resilient health systems. The Act | East Program is being implemented by RTI International with a consortium of partners, led by RTI International and including includes The Carter Center; Fred Hollows Foundation; IMA World Health; Light for the World; Results for Development (R4D); Save the Children; Sightsavers; and Women Influencing Health, Education, and Rule of Law (WI-HER). ii Act | East Country Updates for USAID January–March 2021 January 2021 DRC Act | East Partner: RTI International Total population: 85,281,024 (2018 [est.]) COP: [Redacted] Districts: 519 districts RTI HQ Team: [Redacted] Endemic diseases (# ever endemic districts): Trachoma (65) TABLE: Activities supported by USAID in FY21 Trachoma Mapping Trachoma baseline mapping: 28 EUs, November-January 2021 MDA 1 HZ (Pweto), January 2021 TIS: 1 HZ (Kilwa), October 2020 DSAs (#EUs) TSS: 0 MERLA N/A HSS N/A Summary and explanation of changes made to table above since last month: • None Highlights: • The data for 26 EUs surveyed in the Kasai, Kasai Central, Kwilu and Kwango provinces in December were uploaded to Tropical Data for preliminary analysis and cleaning.