Councillor Deirdre Alden
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Candidates West Midlands 1945-2017
Page | 1 LIBERAL/LIBERAL DEMOCRAT CANDIDATES in the WEST MIDLAND REGION 1945-2017 Constituencies within the counties of Herefordshire, Shropshire, Staffordshire, Warwickshire and Worcestershire INCLUDING SDP CANDIDATES in the GENERAL ELECTIONS of 1983 and 1987 PREFACE As a party member since 1959, based in the West Midlands and a parliamentary candidate and member of the WMLF/WMRP Executive for much of that time, I have been in the privileged position of having met on several occasions, known well and/or worked closely with a significant number of the individuals whose names appear in the Index which follows. Whenever my memory has failed me I have drawn on the recollections of others or sought information from extant records. Seven decades have passed since the General Election of 1945 and there are few people now living with personal recollections of candidates who fought so long ago. I have drawn heavily upon recollections of conversations with older Liberal personalities in the West Midland Region who I knew in my early days with the party. I was conscious when I began work, twenty years ago, that much of this information would be lost forever were it not committed promptly to print. The Liberal challenge was weak in the West Midland Region over the period 1945 to 1959 in common with most regions of Britain. The number of constituencies fought fluctuated wildly; 1945, 21; 1950, 31; 1951, 3; 1955 4. The number of parliamentary constituencies in the region averaged just short of 60, a very large proportion urban in character. Over 1951-55 only one Birmingham constituency was fought, virtually none in the adjoining Black Country conurbation. -
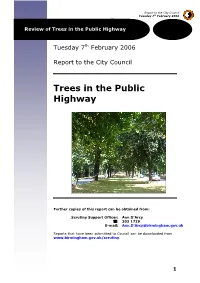
Download: Trees in the Public Highway Scrutiny Review
Report to the City Council Tuesday 7th February 2006 Review of Trees in the Public Highway Tuesday 7th February 2006 Report to the City Council Trees in the Public Highway Further copies of this report can be obtained from: Scrutiny Support Officer: Ann D’Arcy : 303 1729 E-mail: Ann.D’[email protected] Reports that have been submitted to Council can be downloaded from www.birmingham.gov.uk/scrutiny. 1 Report to the City Council Tuesday 7th February 2006 Review of Trees in the Public Highway Contents 1 Summary 6 2 Summary of Recommendations 9 3 Terms of Reference 11 3.1 Reasons for Conducting this Review 11 3.2 The Review Group 12 4 The Wider Benefits of Trees 13 4.1 Introduction 13 4.2 Birmingham’s Legacy of Street Trees 13 4.3 Trees help to Keep us Healthier 13 4.4 Trees Bring Broad Environmental Benefit 14 4.5 Trees can Affect Economic Regeneration 15 4.6 Threats to Trees 15 5 Street Trees in Residential Areas 17 5.1 Introduction 17 5.2 Types of Residential Areas 17 5.3 Threats to Trees from Utility Cable Laying 22 5.4 Insurance Claims 24 5.5 Conclusions on Tree Removal 26 5.6 Planting New Trees in Residential Areas 27 6 Street Trees on Major Routes 31 6.1 Introduction 31 6.2 The Protection of Trees 32 6.3 Development Affecting Street Trees 32 6.4 New Roads in the City 35 6.5 Improving Traffic Flow on Strategic Routes 37 6.6 The Need for More Street Trees on Major Routes 39 7 Tree Management Policy 43 7.1 Introduction 43 7.2 What is Tree Management? 43 7.3 Responsibility for Tree Management 44 7.4 The City Council’s Tree Management -
Pecuniary Interests Relating to Any Items of Business to Be Discussed at This Meeting
Members are reminded that they must declare all relevant pecuniary and non- pecuniary interests relating to any items of business to be discussed at this meeting BIRMINGHAM CITY COUNCIL CITY COUNCIL TUESDAY, 12 JULY 2016 AT 14:00 HOURS IN COUNCIL CHAMBER, COUNCIL HOUSE, VICTORIA SQUARE, BIRMINGHAM, B1 1BB A G E N D A 1 NOTICE OF RECORDING Lord Mayor to advise that this meeting will be webcast for live or subsequent broadcast via the Council's Internet site ( www.birminghamnewsroom.com ) and that members of the press/public may record and take photographs. The whole of the meeting will be filmed except where there are confidential or exempt items. 2 MINUTES 5 - 56 To confirm and authorise the signing of the Minutes of the Meeting of the Council held on 14 June 2016. 3 LORD MAYOR'S ANNOUNCEMENTS To receive the Lord Mayor's announcements and such communications as the Lord Mayor may wish to place before the Council. 4 PETITIONS (15 minutes allocated) To receive and deal with petitions in accordance with Standing Order 8. As agreed by Council Business Management Committee a schedule of outstanding petitions is available electronically with the published papers for the meeting and can be viewed or downloaded. 5 QUESTION TIME (90 minutes allocated) To deal with oral questionsPage in 1 accordance of 228 with Standing Order 9(B) A. Questions from Members of the Public to any Cabinet Member or District Committee Chairman (20 minutes) B. Questions from any Councillor to a Committee Chairman or Lead Member of a Joint Board (20 minutes) C. -
Pecuniary Interests Relating to Any Items of Business to Be Discussed at This Meeting
Members are reminded that they must declare all relevant pecuniary and non- pecuniary interests relating to any items of business to be discussed at this meeting BIRMINGHAM CITY COUNCIL ANNUAL MEETING OF THE CITY COUNCIL TUESDAY, 23 MAY 2017 AT 16:00 HOURS IN COUNCIL CHAMBER, COUNCIL HOUSE, VICTORIA SQUARE, BIRMINGHAM, B1 1BB A G E N D A 1 NOTICE OF RECORDING Lord Mayor to advise that this meeting will be webcast for live or subsequent broadcast via the Council's Internet site (www.birminghamnewsroom.com ) and that members of the press/public may record and take photographs except where there are confidential or exempt items. 2 DECLARATIONS OF INTEREST This is a standard item included on agendas at all first meetings in the Municipal Year. Members are reminded that they must declare all relevant pecuniary and non-pecuniary interests relating to any items of business to be discussed at this meeting. If a pecuniary interest is declared a Member must not speak or take part in that agenda item. Any declarations will be recorded in the minutes of the meeting. 3 MINUTES 5 - 54 To note the public section of the Minutes of the meeting of the Council held on 4 April 2017. 4 ANNUAL REPORT OF THE LORD MAYOR 2016/2017 55 - 80 (15 minutes) To receive the annual report of the Lord Mayor. Page 1 of 94 5 ANNOUNCEMENT OF LORD MAYOR'S AWARDS 6 ELECTION OF THE LORD MAYOR 2017/18 To elect the Lord Mayor. NB. A short break will follow to allow for the robing of the Lord Mayor. -

Candidates West Midlands
Page | 1 LIBERAL/LIBERAL DEMOCRAT CANDIDATES in PARLIAMENTARY ELECTIONS in the WEST MIDLAND REGION 1945-2015 ALL CONSTITUENCIES WITHIN THE COUNTIES OF HEREFORDSHIRE SHROPSHIRE STAFFORDSHIRE WARWICKSHIRE WORCESTERSHIRE INCLUDING SDP CANDIDATES in the GENERAL ELECTIONS of 1983 and 1987 COMPILED BY LIONEL KING 1 Page | 2 PREFACE As a party member since 1959, based in the West Midlands and a parliamentary candidate and member of the WMLF/WMRP Executive for much of that time, I have been in the privileged position of having met on several occasions, known well and/or worked closely with a significant number of the individuals whose names appear in the Index which follows. Whenever my memory has failed me I have drawn on the recollections of others or sought information from extant records. Seven decades have passed since the General Election of 1945 and there are few people now living with personal recollections of candidates who fought so long ago. I have drawn heavily upon recollections of conversations with older Liberal personalities in the West Midland Region who I knew in my early days with the party. I was conscious when I began work, twenty years ago, that much of this information would be lost forever were it not committed promptly to print. The Liberal challenge was weak in the West Midland Region over the period 1945 to 1959 in common with most regions of Britain. The number of constituencies fought fluctuated wildly; 1945, 21; 1950, 31; 1951, 3; 1955 4. The number of parliamentary constituencies in the region averaged just short of 60, a very large proportion urban in character. -

Birmingham City Council Or a Head from Signing a Petition to Sharing Some Questions to Answer in Where Did It Start? Teacher at School
Raising Your Voice: Digital Storytelling to Create Change + Section Name • 1 TABLE OF CONTENTS PART I Say It Loud! Creating Powerful Digital Stories for Change CHAPTER 1 CHAPTER 2 CHAPTER 3 CHAPTER 4 CHAPTER 5 CHAPTER 6 The Power of Crafting A Strong Building Blocks of Choosing Your Why Digital? Type of Digital Storytelling Storytelling Narrative Good Storytelling Story for Inspiring Social Change 6 14 20 26 30 32 2 • Section Name When we’re born, our world is very small. Sometimes it only extends to our family and the four walls around us. But as we grow, the world grows with us. First we get to know our neighbourhood, and then we’re off to school where we meet new people and see new things almost everyday. As we experience the world, we notice more and more. Many things make us happy, proud, and excited. Other things make us sad, frustrated, or angry – the kinds of things that you wish you could change. The truth is that YOU ARE POWERFUL. Everyone, no matter how young or Part I: old, possesses the power to have a positive impact on the world around them. And each of us has a role to play in making the world a better place. Most of the time this starts with finding our voice – discovering a way to Say It Loud! make ourselves, our opinions and our stories heard. In today’s world, sharing stories is one way we can connect with each other Creating to fight for change. Technology has made this easier than ever – giving us a platform on social media and the Internet to communicate to others beyond Powerful our living rooms, classrooms and communities. -
Birmingham City Council Held on Tuesday 6 December 2016 at 1400 Hours in the Council Chamber, Council House, Birmingham
MEETING OF BIRMINGHA M CITY COUNCIL 6 DECEMBER 2016 MINUTES OF THE MEETING OF BIRMINGHAM CITY COUNCIL HELD ON TUESDAY 6 DECEMBER 2016 AT 1400 HOURS IN THE COUNCIL CHAMBER, COUNCIL HOUSE, BIRMINGHAM PRESENT:- Lord Mayor (Councillor Carl Rice) in the Chair. Councillors Muhammad Afzal Mick Finnegan Mary Locke Uzma Ahmed Des Flood Ewan Mackey Mohammed Aikhlaq Jayne Francis Majid Mahmood Deirdre Alden Matthew Gregson Karen McCarthy Robert Alden Carole Griffiths James McKay Nawaz Ali Peter Griffiths Gareth Moore Tahir Ali Paulette Hamilton Yvonne Mosquito Sue Anderson Andrew Hardie Brett O’Reilly Gurdial Singh Atwal Roger Harmer John O’Shea Mohammed Azim Kath Hartley David Pears Susan Barnett Barry Henley Robert Pocock David Barrie Penny Holbrook Victoria Quinn Bob Beauchamp Des Hughes Hendrina Quinnen Matt Bennett Jon Hunt Chauhdry Rashid Kate Booth Mahmood Hussain Habib Rehman Steve Booton Shabrana Hussain Fergus Robinson Marje Bridle Timothy Huxtable Gary Sambrook Mick Brown Mohammed Idrees Rob Sealey Alex Buchanan Zafar Iqbal Shafique Shah Sam Burden Ziaul Islam Mike Sharpe Andy Cartwright Meirion Jenkins Sybil Spence Tristan Chatfield Simon Jevon Claire Spencer Zaker Choudhry Julie Johnson Stewart Stacey Debbie Clancy Brigid Jones Ron Storer John Clancy Carol Jones Martin Straker-Welds Lynda Clinton Josh Jones Sharon Thompson Lyn Collin Nagina Kauser Paul Tilsley Maureen Cornish Tony Kennedy Karen Trench John Cotton Ansar Ali Khan Lisa Trickett Ian Cruise Changese Khan Anne Underwood Basharat Dad Mariam Khan Margaret Waddington 2281 City Council – 6 December 2016 Phil Davis Narinder Kaur Kooner Ian Ward Diane Donaldson Chaman Lal Mike Ward Peter Douglas Osborn Mike Leddy Fiona Williams Barbara Dring Bruce Lines Ken Wood Neil Eustace John Lines Alex Yip Mohammed Fazal Keith Linnecor Waseem Zaffar ************************************ NOTICE OF RECORDING 18752 The Lord Mayor advised that the meeting would be webcast for live and subsequent broadcasting via the Council’s internet site and that members of the Press/Public may record and take photographs. -
Annual Review 2017 / 2018
Annual Review 2017 / 2018 The Birmingham Civic Society Message from Geoff Cole Chairman, Birmingham Trees for Life This winter we paid tribute to our former colleague and founder the late Councillor and former Lord Mayor Ray Hassall, who passed away in 2017. Ray’s Wood was planted at Perry Hall Park with the help of Ray’s colleagues and friends, Civic Society Trustees and the Friends of Perry Hall Park. The Lord Mayor planted our 70,000th tree in memory of Ray - we hope this is a fitting tribute to his work with BTFL, as well as his wider contribution to Perry Barr and the City. We have also been delighted to help the Birmingham Civic Society celebrate its Centenary with several planting events at parks with a historical association with the Society – more about these later in this review. Following the loss of the Broad Street plane tree reported in last year’s review, Birmingham City Council set up a special Committee to review its existing policy for trees and make recommendations. The result was a completely new Tree Policy which was unanimously approved by the Council, which offers much greater protection to the City’s trees. As a member of BTFL’s Committee, Cllr. Fiona Williams proved to be a staunch voice for trees, and led the Scrutiny Committee which heard the evidence. Along with the work of another BTFL Committee member, Simon Needle, in developing the recommendations, this process has resulted in a significant increase in awareness of the value of trees, the threats to them and the challenges to planting and protecting trees, and how these matters should be managed. -

Annual Review 2016 / 2017
Annual Report 2017 25/9/17 08:38 Page 1 The Birmingham Civic Society Annual Review 2016 / 2017 Annual Report 2017 25/9/17 08:38 Page 2 Message from Geoff Cole Chairman, Birmingham Trees for Life In a year which another significant milestone was reached – that of planting our 60,000th tree in Birmingham – we were also met with the sad loss of one of BTFL’s founders, Councillor Ray Hassall, former Lord Mayor of Birmingham. Cllr. Hassall was instrumental in the setting up of BTFL in 2006. Having worked with him for many years, I would like to pay a personal tribute to Ray, which you will find on page 3. BTFL’s collaboration with the Woodland Trust was officially ‘launched’ by the Lord Mayor, Councillor Carl Rice, at a wonderful tree planting event at Cofton Park in March. We are delighted to be partnered with the Woodland Trust as they start to work more in urban areas, and look forward to our relationship developing over the coming years. We once again enjoyed the support of staff from Deutsche Bank Birmingham; this season, they asked us to involve a different group of young people in the events they supported, so we invited disadvantaged young people being helped by Platinum Housing Care to join us at the three Deutsche Bank sponsored events. Our active programme of school and community involvement continues, with 476 schoolchildren from 21 schools and a college involved in tree planting in the 2016-17 season, as well as 19 other children at Saturday events. A number of Friends groups joined us on site, and at Acocks Green Recreation Ground, the local Scout Troop were also very enthusiastic participants. -

Study Visit Report
Lead authors: Julie Hervé and Marianna Kajantie Version n. 1 Date 21/03/2016 Study visit report Study Visit Birmingham, 8 - 10.02.2016 TABLE OF CONTENTS 1. Executive Summary ...................................................................................... 3 2. Programme ............................................................................................... 6 3. Methodology and tools used .......................................................................... 11 4. Key topics presented and learning points .......................................................... 12 5. Initiatives presented .................................................................................. 14 6. Lessons learnt .......................................................................................... 18 7. Conclusions ............................................................................................. 28 A. Annex 1: List of participants ......................................................................... 29 B. Annex 2: Presentations (from local actors and/or experts) ..................................... 32 Study visit in Birmingham – 8-10.02.2016 2 1. Executive Summary The sixth visit of the Culture for Cities and Regions project took place in Birmingham on 8-10 February 2016. Selected participants came from Aarhus, Antwerp, Barcelona, Brussels, Espoo, Helsinki, Kuopio, Lublin, Manchester, Seine Maritime, Tampere, and Turin. In their application form to attend the visit in Birmingham participants felt the need improve knowledge -

Officers Report
Committee Date: 27/11/2014 Application Number: 2014/06455/PA Accepted: 15/09/2014 Application Type: Householder Target Date: 10/11/2014 Ward: Perry Barr 127 Dyas Avenue, Great Barr, Birmingham, B42 1HJ Erection of two storey side & rear extension, and single storey rear extension, and replacement detached garage to rear Applicant: Ramzan Sharif c/o Agent Agent: Mr Hussain Tariq 218-220 Windsor Street, Nechells, Birmingham, B7 4NE Recommendation Approve Subject To Conditions 1. Proposal 1.1. Consent is sought for the erection of a two storey side and rear extension, and single storey rear extension. 1.2. The proposed extension would measure 4m in width from the side wall of the main house and would extend 4.5m beyond the main rear wall at ground floor, and 3m deep at first floor. The proposal would be designed with a hipped roof and include a single storey bay window feature to the front. The development would provide a ground floor granny flat and wet room for an elderly family member, and a new family kitchen would be provided at the rear, and a study, two additional bedrooms and en suite shower room at first floor. 1.3. A new replacement detached garage is also proposed to the rear of the site. The garage would measure 5.7m x 3.9m and would be designed with a pitched roof at a maximum height of 3.6m (2.4m to eaves) 1.4. In addition to the above, a new vehicular hardstanding is shown on the submitted plans; this has been indicated to be laid out with permeable materials. -

Local Authorities
Authorities-A-F.qxd 02/09/2013 12:52 Page 82 LOCAL AUTHORITIES BEXLEY L Community Planning: Mrs Maureen Holkham, Deputy Director - London Borough of Bexley, (The London Borough of Bexley), Corporate Policy & Communications, Bexley Civic Offices, Bexley Civic Offices, Broadway, Bexleyheath DA6 7LB 020 Broadway, Bexleyheath DA6 7LB 020 3045 3608 020 8294 8303 7777 020 8301 2661 [email protected] 6863 maureen.holkham@bexley,gov.uk www.bexley.gov.uk Community Safety: Mr Mark Usher, Community Safety Co- FACTS & FIGURES ordinator, Bexley Civic Offices, Broadway, Bexleyheath DA6 7LB Police Authority: Metropolitan Police Authority 020 3045 3580 020 8294 6226 Health Authority: NHS London [email protected] Learning and Skills Council: South East Parliamentary Constituencies: Bexleyheath & Crayford, Erith Computer Management: Mr Tony Allen, Deputy Director (ICT), and Thamesmead, Old Bexley and Sidcup Bexley Civic Offices, Broadway, Bexleyheath DA6 7LB 020 EU Constituencies: South East 3045 4904 020 3045 5444 [email protected] Election Frequency: Elections are of whole council Twinning: Evry (France); Neheim-Husten (Germany) Consumer Protection and Trading Standards: Mr David Bryce- Smith, Deputy Director - Development, Housing & Community, PRINCIPAL OFFICERS Bexley Civic Offices, Broadway, Bexleyheath DA6 7LB 020 Chief Executive: Mr Will Tuckley, Chief Executive, Bexley Civic 3045 5718 020 8308 7897 [email protected] Offices, Broadway, Bexleyheath DA6 7LB 020 3045 3232 020 8294 6024 [email protected]