Original Articles X-Linked Agammaglobulinaemia in Hong Kong Chinese
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Philippine Airlines' Laboratory and Testing Partners for Philippine Domestic Travel
Philippine Airlines’ Laboratory and Testing Partners for Philippine Domestic Travel RAPID TEST AND RT-PCR TEST PARTNER One Health Medical Services, Inc. ADDRESS: OHM Building, Andrews Avenue (beside PAL Gate 1A), MIAA Zone, Pasay City 1300 LANDLINE: (+632) 8938-6680 to 81 MOBILE: (+639) 66-561-7639 E-MAIL: [email protected] RELEASE OF TEST RESULTS: 20 min for Rapid Tests, 24-48 hrs for RT-PCR Tests RT-PCR TEST PARTNERS Cardinal Santos Medical Center Fe Del Mundo Medical Center ADDRESS: 10 Wilson, Greenhills West, San Juan 1502 ADDRESS: 11 Banawe st. Brgy Dona Josefa, Quezon City LANDLINE: (+632) 8724-3997 LANDLINE: (+632) 8712-0845 loc 1903 and 1601 MOBILE: (+639) 49-333-5489 MOBILE: (+639) 17-5583-726 E-MAIL: [email protected] E-MAIL: [email protected] WEBSITE: www.csmceconsult.com WEBSITE: www.fedelmundo.com.ph RELEASE OF TEST RESULTS: 72-120 hrs RELEASE OF TEST RESULTS: 48-72 hrs Kaiser Medical Center New World Diagnostics WEBSITE: https://appointments.kaisermedcenter.com/pal WEBSITE: https://www.nwdi.com.ph/ RELEASE OF TEST RESULTS: 24 hrs RELEASE OF TEST RESULTS: 48-72 hrs (excl. Sun) MAKATI CITY QUEZON CITY ADDRESS: G/F King's Court Building 1, 2129 Don Chino ADDRESS: 205 D. Tuazon Street, Brgy. Maharlika, Roces Avenue, Makati City Quezon City, Philippines LANDLINE: (+632) 8804-9988 LANDLINE: (+632) 8790-8888, local 218 or 225 MOBILE: (+639) 17-577-3886 MOBILE: OIC – Laboratory Manager Gretchen Catli: E-MAIL: [email protected] (+639) 17-530-1143, Sales & Marketing Manager Rio E. Barrozo: (+639) 16-453-5662 MANILA CITY E-MAIL: [email protected], ADDRESS: G/F Robinsons Place Ermita, Manila [email protected] LANDLINE: (+632) 8353-0495 MOBILE: (+639) 17-183-5488 QUEZON CITY E-MAIL: [email protected] ADDRESS: G/F Hipolito Bldg. -

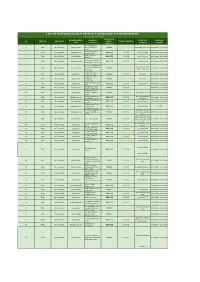
2015Suspension 2008Registere
LIST OF SEC REGISTERED CORPORATIONS FY 2008 WHICH FAILED TO SUBMIT FS AND GIS FOR PERIOD 2009 TO 2013 Date SEC Number Company Name Registered 1 CN200808877 "CASTLESPRING ELDERLY & SENIOR CITIZEN ASSOCIATION (CESCA)," INC. 06/11/2008 2 CS200719335 "GO" GENERICS SUPERDRUG INC. 01/30/2008 3 CS200802980 "JUST US" INDUSTRIAL & CONSTRUCTION SERVICES INC. 02/28/2008 4 CN200812088 "KABAGANG" NI DOC LOUIE CHUA INC. 08/05/2008 5 CN200803880 #1-PROBINSYANG MAUNLAD SANDIGAN NG BAYAN (#1-PRO-MASA NG 03/12/2008 6 CN200831927 (CEAG) CARCAR EMERGENCY ASSISTANCE GROUP RESCUE UNIT, INC. 12/10/2008 CN200830435 (D'EXTRA TOURS) DO EXCEL XENOS TEAM RIDERS ASSOCIATION AND TRACK 11/11/2008 7 OVER UNITED ROADS OR SEAS INC. 8 CN200804630 (MAZBDA) MARAGONDONZAPOTE BUS DRIVERS ASSN. INC. 03/28/2008 9 CN200813013 *CASTULE URBAN POOR ASSOCIATION INC. 08/28/2008 10 CS200830445 1 MORE ENTERTAINMENT INC. 11/12/2008 11 CN200811216 1 TULONG AT AGAPAY SA KABATAAN INC. 07/17/2008 12 CN200815933 1004 SHALOM METHODIST CHURCH, INC. 10/10/2008 13 CS200804199 1129 GOLDEN BRIDGE INTL INC. 03/19/2008 14 CS200809641 12-STAR REALTY DEVELOPMENT CORP. 06/24/2008 15 CS200828395 138 YE SEN FA INC. 07/07/2008 16 CN200801915 13TH CLUB OF ANTIPOLO INC. 02/11/2008 17 CS200818390 1415 GROUP, INC. 11/25/2008 18 CN200805092 15 LUCKY STARS OFW ASSOCIATION INC. 04/04/2008 19 CS200807505 153 METALS & MINING CORP. 05/19/2008 20 CS200828236 168 CREDIT CORPORATION 06/05/2008 21 CS200812630 168 MEGASAVE TRADING CORP. 08/14/2008 22 CS200819056 168 TAXI CORP. -
NAST · up College of Forestry Join Hands with Royal Society of London on Collaborative Study of Rain Forest Ecology
NATIONAL ACADEMY OF SCIENCE AND TECHNOLOGY National Science and TedmoloaY Authority National Scientists: Juan S. Salcedo, Jr., M.D. Alfredo C. Santos, Dr. phil GrE!lorio Y. Zara, Dr. Sci· Fe del Mundo, M.D. Eduardo A. Quiaumbing, Ph.D. Executive Council Paulo C. Campos - President Alfredo V. Lagmay - Vice-President . \ Tito A. Mijares - Secretary Alfredo C. Santos - Member Carmen C. Velasquez - Member " Academicians : Teodoro A. Agoncillo, Litt. D. (honoris causa) Encarnacion Alzona, Ph.D. elare R. Baltazar, Ph.D. Julian Banzon, Ph.D. Luz O. Belardo, Ph.D. Paulo C. Campos, M.D. Magdalena C. Cantoria, Ph.D. Amando M. Dalisay, Ph.D. Conrado S. Dayrit, M.D. Jose Encarnacion, Jr., Ph.D. Pedro B. Escuro, Ph.D. Raymundo A. Favila, Ph.D. Francisco M. Fronda, Ph.D. Emerita V. de Guzman, Ph.D. Bienvenido O. Juliano, Ph.D. Alfredo V. Lagmay, Ph.D. Cecilio F. Lopez, Dr. PhiL· Melecio S. Magno, Ph.D, Fe del Mundo, M.D. Tito A. Mijares, Ph.D. GeminiaDO T. de Ocampo, M.D. Eduardo A. Quisumbing, Ph.D. Jose N. Rodriguez, M.D.· Casimiro del Rosario, Ph.D. Juan S. Salcedo, Jr., M.D. Alfredo C. Santos, Dr. PhiL Francisco O. Santos, Ph.D. Joventino D. Soriano, Ph.D. Clara Y. Lim-Sylianco, Ph.D. Dioscoro i. Umall, Ph.D. ' Carmen C. Velasquez, Ph.D. GrE!lorio T. Velasquez, Ph.D. Gregorio Y: Zan, Ph.D •• ·deceased Philippines to Host First Meeting of Vol. 4 No.1, March, 1982 Asean Scientists by End of '82 NAST Head Elected Chairman Asean Scientists convened in Kuala Malaysian Scientific Association (MSA), (1) the rich diversity of natural resour Lumpur, March 13-15 in an effort to who earlier invited the Academy offi ces both on land (especially low form an organization to link scientists cials to Kuala Lumpur. -

Sarah J. De Los Reyes, MD, MPH, DPCOM, FPAPSHPI Primary & Aesthetic Skin Health/ Epidemiology/ Occupational Health & Safety Home: 3524 Vigan St
Sarah J. De los Reyes, MD, MPH, DPCOM, FPAPSHPI Primary & Aesthetic Skin Health/ Epidemiology/ Occupational Health & Safety Home: 3524 Vigan St. Sta. Mesa, Manila, 1016 Offices: Suite 216 MAB, Dr. Fe Del Mundo Medical Center 11 Banawe corner Cardiz Streets, Quezon City Rustan Marketing Corporation 3F Midland Buendia Bldg., Sen G. Puyat Ave., Makati City Phone: (+632) 731-1802;890-97-03; 714-5109 Mobile: (+63917) 856-2427 ; (+63998) 855-0733 E-Mail: [email protected] Birthdate: 10 May, 1977 Nationality: Filipino Current Country of Residence: Philippines TIN: 226-145-698-000 SSS: 34-5166764-6 PHILHEATH: 08-252-282-363 PROFILE STATEMENT: An experienced and motivated professional who is able to work in a pro-active environment, makes extensive use of her skills and knowledge while concurrently enhancing and expanding them. Accomplishments in primary & aesthetic skin health, epidemiology, policy writing, occupational health and safety, as well as research management and scientific writing in the field of skin health, HIV and nutrition. EDUCATION April-August, 2015 Philippine College of Occupational Medicine, Inc. Advanced Diplomate Courses April 28-May 7, 2014 College of Public Health, University of the Philippines, Manila 71st Postgraduate Course in Occupational Health and Safety April 2013 National Skin Centre, Singapore Clinical Dermatology Course for Family Physicians November 2011-November 2012 Medical Skin Health Training Foundation, Inc. Clinical & Aesthetic Dermatology Training May 4-15 2009 College of Public Health, University of the Philippines, Manila- SEAMEO-TropMed Regional Center for Public Health, Hospital Administration, Environmental and Occupational Health International Course on Advanced Epidemiology June 2007 University of the Philippines, Manila Master of Public Health (Epidemiology Tracking) April 2001 University of Santo Tomas Doctor of Medicine April 1997 De La Salle University, Manila Bachelor of Science, Major in Biology Curriculum Vitae of Sarah J. -

Academy News 1983
Academy News A Quarterly Newsletter Published by The National Academy of Science and Techno-logy VOLUME 5, NOS. 1-4 ISSN 0115-4095 1983 January- December CONTENTS DFG-NAST Accord Signed .. ...... ... .. .. ... ...... ... .... .. .... 3 Indian Academy Signs Exchange Agreement . ..... ... .... .. .. .. ........ .4 Hughes on Respiratory Adaptation of Invertebrates .. ... .... ...... ....... 5 Four Academicians to 15th Pacific Science Congress . .. .. .... .. .... ...... 5 Delhi Meet of Scientists to Tackle Role of Scientific ·Societies in National Development .. ... .... .... .. .. .. .. ... ... .. 7 India's Savant Here .. ... ...... ........ .. ... ... ..... .. .. ..... ... .. 7 Dr. C.R . Rao, Universally Renowned Mathematician and Statistician Here . .... .. .......... ..... .. ... .. ...... .. ... .. 8 The Proposed Ph .D. Program in Statistics for the Country .. .. ..... .. 8 Essential Oils from Apitong .. ... .... .... ......... .. ..... .. ... 13 Com mercia! Session ... .............. .......... .. .. .... .. .... ... 13 International Workshop on Essential Oils . ......... .. .... .. .. .... 14 Caucus on ASEAN Organization on S & T for Development . .. .... .... .. 15 The New Academicians ..... ..... ....... .. ...... .. .. ......... 17 Umali Named Member of Executive Council . ................... .. .. .. ... 25 Memorial Lectures in Honor of Dr. Casimiro del Rosario . ... ............ .... 26 The History of the PhiliQpine Weather Bureau . .. ... ... .. .. ... .... .. .. .. 28 Dr. Francisco 0. Santos, Academician Passes Away .. .. -
List of Licensed Covid-19 Testing Laboratory in the Philippines
LIST OF LICENSED COVID-19 TESTING LABORATORY IN THE PHILIPPINES ( as of November 26, 2020) OWNERSHIP MUNICIPALITY / NAME OF CONTACT LICENSE REGION PROVINCE (PUBLIC / TYPE OF TESTING # CITY FACILITY NUMBER VALIDITY PRIVATE) Amang Rodriguez 1 NCR Metro Manila Marikina City Memorial Medical PUBLIC Cartridge - Based PCR 8948-0595 / 8941-0342 07/18/2020 - 12/31/2020 Center Asian Hospital and 2 NCR Metro Manila Muntilupa City PRIVATE rRT PCR (02) 8771-9000 05/11/2020 - 12/31/2020 Medical Center Chinese General 3 NCR Metro Manila City of Manila PRIVATE rRT PCR (02) 8711-4141 04/15/2020 - 12/31/2020 Hospital Detoxicare Molecular 4 NCR Metro Manila Mandaluyong City PRIVATE rRT PCR (02) 8256-4681 04/11/2020 - 12/31/2020 Diagnostics Laboratory Dr. Jose N. Rodriguez Memorial Hospital and (02) 8294-2571; 8294- 5 NCR Metro Manila Caloocan City PUBLIC Cartridge - Based PCR 08/13/2020 - 12/31/2020 Sanitarium 2572 ; 8294-2573 (GeneXpert)) Lung Center of the 6 NCR Metro Manila Quezon City PUBLIC rRT PCR 8924-6101 03/27/2020 - 12/31/2020 Philippines (LCP) Lung Center of the 7 NCR Metro Manila Quezon City Philippines PUBLIC Cartridge - Based PCR 8924-6101 05/06/2020 - 12/31/2020 (GeneXpert) Makati Medical Center 8 NCR Metro Manila Makati City PRIVATE rRT PCR (02) 8888-8999 04/11/2020 - 12/31/2020 (HB) Marikina Molecular 9 NCR Metro Manila Marikina City PUBLIC rRT PCR 04/30/2020 - 12/31/2020 Diagnostic laboratory Philippine Genome 10 NCR Metro Manila Quezon City Center UP-Diliman PUBLIC rRT PCR 8981-8500 Loc 4713 04/23/2020 - 12/31/2020 (NHB) Philippine Red Cross - (02) 8790-2300 local 11 NCR Metro Manila Mandaluyong City PRIVATE rRT PCR 04/23/2020 - 12/31/2020 National Blood Center 931/932/935 Philippine Red Cross - 12 NCR Metro Manila City of Manila PRIVATE rRT PCR (02) 8527-0861 04/14/2020 - 12/31/2020 Port Area Philippine Red Cross 13 NCR Metro Manila Mandaluyong City Logistics and PRIVATE rRT PCR (02) 8790-2300 31/12/2020 Multipurpose Center Research Institute for (02) 8807-2631; (02) 14 NCR Metro Manila Muntinlupa City Tropical Medicine, Inc. -

List of Accredited Hospital
LIST OF ACCREDITED HOSPITAL Tel no: (02) 831.6511, (02) 831.6512 LUZON (02) 831.6514 Fax no.: (02) 831.4788 Coordinator: Dr. Araceli Jo NATIONAL CAPITAL REGION (NCR) MWFSAT 3-5pm TTH 10-12nn rm 301 CALOOCAN CITY MANDALUYONG ACEBEDO GENERAL HOSPITAL DR. VICTOR R. POTENCIANO MEDICAL CENTER 849 General Luis St. Bagbaguin , Caloocan City 163 EDSA, Mandaluyong City Tel no.: (02) 893.5363, (02) 404.4181 Tel no.: (02) 531.4911 – 19, (02) 531.4921 – 24 (02) 400.1272 Fax no.: (02) 531.4659 Fax no.: (02) 983.5363 Coordinator: Dr. Telly S. Cheng Coordinator: Dr. Eddie Acebedo MON-SAT 9-3pm rm 218 PROCEED TO OPD MANILA CITY MANILA CENTRAL UNIVERSITY FILEMON D. TANCHOCO MEDICAL FOUNDATION, INC CHINESE GENERAL HOSPITAL Samson Road , EDSA, Caloocan City 286 Blumentritt St., Sta Cruz, Manila City Tel no.: (02) 367.2031, (02) 366.9589 Tel no.: (02) 711.4141-51, (02) 743.1471 Fax no.: (02) 361.4664 Fax no.: (02) 743.2662 Coordinator: Dr. Ma. Rosario E. Bonagua Coordinator: Dr. Edwin Ong MTW 3:00PM-5:00PM MON-FRI 9-12nn rm 336 PROCEED TO INDUSTRIAL CLINIC DE OCAMPO MEMORIAL MEDICAL CENTER MARTINEZ MEMORIAL HOSPITAL 2921 Nagtahan St., cor. Magsaysay Blvd, Manila City 198 A. Mabini St., Maypajo, Caloocan City Tel no.: (02) 715.1892, (02) 715.0967 Tel no.: (02) 288.8862 ,(02) 288.8863 Coordinator: Dr. Aloysius Timtiman Fax no.: (02) 288.8861 MTWTHF 9:30-4:30 / S 9:30-1:00pm Coordinator: Dr. Santos del Rio PROCEED TO OPD MON-SAT 9:00am-12:00nn/ PROCEED TO OPD HOSPITAL OF THE INFANT JESUS NODADO GENERAL HOSPITAL - CALOOCAN 1556 Laong-Laan Road,Sampaloc Manila City Area - A Camarin, Caloocan City Tel no.: (02)731.2771, (02) 731.2832 Tel no.: (02) 962.8021 Coordinator: Dr. -

PSEUDOMONAS Infections in Hospitalized Infants and Children
Tram. Nor. A cud. Sci &- Tech (Phils.) 1985.7.- 14]·152 PSEUDOMONAS INFECfIONS IN HOSPITALIZED INFANTS AND CHILDREN METRO MANILA 1984 Fe del Mundo, Jaime Santos and Cynthia Santos Lungsod ng Kabalatll'l Children's HospilOi Quezon City. Phl1ipphtes ABSTRACT In 1984 out of 6,270 total pediatric admissions at lungsod ng K<lb<ltaan (LnK) Children's HospitaJ) Metro Manila, 171 had positive cuJtUfes for Pseudo monas aeruginv..w. with neonates as the most commonly affected. Symptomll;lo[ogy and blood counls were not significant cnough to be considered diagnostic, Positive cultures from speLimcm, parlicularly the blood, was th~ only fmding that clinched the- diagnosis, just as it was 10 }'cars ago in a study at the Philippine C..eneml Hospital. Se.nsjtivity tests showed changes from previous reports; to some extent this may have been due to a difference in presently available antibiotics. As mortality is still high and the diagnosis still complicated and costly, time-test.ed simple prcvcntiv\: mC,ilsures :He important. Introduction Infections caused by the ubiquitous Pseudomonas especially the opportunis tic pathogenic to man, Pseudomonas aeruginosa, are not in the top morbidity and mortality lists anywhere. Yet these continue to be considered dreadful diseases which cause considerable concern in hospitals and to those deeply concerned with I he health of children. It is known that the disease commonly affects neonates particularly the debilitated or critically ill, who need nasogastric tubes, suction and humidifying apparatus Or assisted ventilation. It is also often observed among malnourished children or those who have chronic iHness requiring prolonged antibiotics or im muno.suppressive treatments. -

The National Scientists National Scientists (1978-1989)
The National Scientists National Scientists (1978-1989) Year Recipient Specialty Remarks 1978 Juan S. Salcedo, Jr., M.D. Nutrition and Public died October 25, 1988 Health 1978 Alfredo C. Santos, Dr. phil. Physical Chemistry 1978 Gregorio Y. Zara, D.Sc., Engineering and Inventions died October 15, 1978 1980 Fe del Mundo Pediatrics 1980 Eduardo A. Quisumbing. Ph.D. Plant Taxonomy, died August 23, 1986 Systematics and Morphology 1982 Geminiano T. de Ocampo, M.D. Ophthalmology died September 2, 1987 1982 Casimiro del Rosario, Ph.D. Ph ysics, Astronomy and died September 15, 1982 Meteorology 1982 Gregorio T. Velasquez, Ph.D. Phycology died July 29 , 1989 1983 Francisco M. Fronda, Ph. D. Animal Husbandry died February 17, 1986 1983 Francisco O. Santos, Ph. D. Human Nutrition and posthumous Agricultural Chemistry died February 19,1983 1983 Carmen C. Velasquez, Ph.D. Parasitology 1985 Teodoro A. Agoncillo, Litt. D. (h. c. ) Philippine History posthumous died January 14, 1985 1985 Encarnacion A. Alzona, Ph. D. Philippine History 1985 Hilario D.G. Lara, M.D., Dr. P.lL Public Health died December 18, 1987 1986 Julian A. Banzon, Ph.D. Chemistry died September 14,1988 1986 Dioscoro L. Umal~ Ph.D. Agriculture and Rural Development 1987 Luz Olivero.. Belardo, Ph.D. Phytochemistry 1987 Jose Encarnacion, Jr., Ph.D, Economics 1988 Alfredo V. Lagm,y, Ph. D. Experimental Psychology 1989 Paulo C. Capros. M.D . Nuclear Medicine 141 NATIONAL SCIENTISTS Rank and Title of National Scientist Conferment of the rank and title of National Scientist by the President of the Re public is the highest honor given to a man of science in the Philippines. -

Directory for Covid-19
CATHOLIC BISHOPS’ CONFERENCE OF THE PHILIPPINES – EPISCOPAL COMMISSION ON HEALTH CARE DIRECTORY FOR COVID-19 DIRECTORY OF NATIONAL GOVERNMENT AGENCIES ORGANIZATIONS CONTACT DETAILS Department of Health (02) 894-COVID (02) 894-26843 For PLDT, SMART, SUN, and TnT Subscriber (COVID-19 HOTLINE) 1555 Telimed Management Inc., and Medgate Hotline (02) 8424-1724 Global TeleHealth, Inc. (KonsultaMD) (02) 7798-8000 National Center for Mental Health (02) 8531-9001 (02) 899-USAP (8727) 0917-899USAP (8727) Research Institute for Tropical Medicine (02) 8807-2631 Philippine Red Cross 1158 / 143 For COVID-19 concerns, psychosocial support and restoring family links 1158 Emergency Hotline 911 Philippine National Police 117 Presidential Complaint Center 8888 Presidential Anti-Corruption Commission 0906-692-7324 Metropolitan Manila Development Authority 136 Land Transportation Office (02) 8922-9061 Department of Education 0928-871-8053 (Smart) 470 General Luna Street, Catholic Bishops’ Conference of the Philippines (CBCP) Compound, Intramuros, Manila (+632) 8 926-31-47 [email protected] CATHOLIC BISHOPS’ CONFERENCE OF THE PHILIPPINES – EPISCOPAL COMMISSION ON HEALTH CARE DIRECTORY FOR COVID-19 0915-205-3244 (Globe) Region 1 0998-583-5732 (072) 682-2324 loc. 119 Region 2 0917-504-7971 0906-682-8208 0917-166-8600 078) 304-3855 Region 3 (045) 598-8580 CALABARZON 0977-827-6112 (02) 8682-5773 (02) 8631-4070 0917-840-8381 Region 5 0999-682-4775 0920-925-5833 Region 6 (033) 336-2816 Region 7 (032) 414-7399 Region 8 (053) 323-3156 Region 9 0998-280-8852 0919-353-9158 -

Repurposed Antiviral Drugs for COVID-19 – Interim WHO SOLIDARITY Trial Results
This page will be deleted before publication, and replaced by the Journal’s cover page Supplementary online material for Repurposed antiviral drugs for COVID-19 – interim WHO SOLIDARITY trial results 1 Repurposed antiviral drugs for COVID-19 – interim WHO SOLIDARITY trial results Contents list for supplementary online material Page 3 Membership: Writing Committee; Data and Safety Monitoring Committee 4 Membership: International Steering Committee and its Executive Group 5 National investigators and researchers 12 Data managers, statistical analysts and WHO trial co-ordination team 12 Other collaborators in participating countries 14 Acknowledgements 15 Supp. Table S1. Treatment allocation vs respiratory support in hospital in patients not ventilated at entry and eventually discharged alive 16 Supp. Table S2. Use of corticosteroids and other non-study drugs 17 Supp. Table S3. Multivariate analysis simultaneously estimating all 4 treatment effects 18 Supp. Fig S1. Effects on 28-day in-hospital mortality of (a) Remdesivir, (b) Hydroxychloroquine, (c) Lopinavir, (d) Interferon 19 Supp. Fig S2. Effects of Remdesivir on the 28-day risk of death from any cause, subdivided by Respiratory support at entry 20 Supp. Fig S3. Effects of Hydroxychloroquine on the 28-day risk of death from any cause, subdivided by Respiratory support at entry 21 Supp. Fig S4. Effects of Lopinavir on the 28-day risk of death from any cause, subdivided by Respiratory support at entry 22 Supp. Fig S5. Effects of Interferon on the 28-day probability of death from any cause, subdivided by Respiratory support at entry 23 Supp. Fig S6. RRs of any death, Remdesivir vs Control, by entry characteristics 24 Supp. -
Ectopic Murmurs
Official Publication of the FAR EASTERN UNIVERSITY Dr Nicanor Reyes Jr School of Medicine Alumni Foundation ECTOPIC MURMURS Volume 22 Number 9 September 2011 Opinions and articles published herein are those of the authors and do not necessarily reflect that of the FEUDNSM Alumni Foundation GOODBYE REMEMBERING DR FE DEL MUNDO 62 DR FE DEL MUNDO CELSO DEL MUNDO MD The world has lost an icon, who LINDA G BARRANDA MD had cared thousand of sick children, She was called by Dr Fe Del Mundo was our Message from the the Almighty consultant at Lungsod ng BOARD CHAIRMAN Lord to live with Kabataan and in her hospital angels and Have you ever noticed how named after saints. things in life her in The long lasting turn out legacy of virtues, Quezon CELSO DEL and knowledge, right, no MUNDO MD City when I matter how she left behind, was a Will always be with us, her you think medical clerk students, to continue her noble they should in 1983- task. LINDA have been? BARRANDA MD 84 and later My life is a Nobody can replace a woman with as a medical such wit and intelligence, prime Intern in 1996-1997. She had inspired all her students, to PEPITO C example. As I did not take pediatrics RIVERA MD follow her footsteps, When I was a To care for ailing babies and at FEU because I transferred surgical resident at the old FEU children and gave them the to Bicol Christian College of Hospital in Morayta Manila, I precious life, Medicine (BCCM) in Legazpi And enjoy the life of good health, was the only single resident in City, I did not become her through her caring and love.