A Doctors' Open Letter to Daniel Andrews a Dozen Melbourne
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

70% of Victorians Approve of the Way Premier Andrews Is Handling His
Article No. 8518 Available on www.roymorgan.com Link to Roy Morgan Profiles Thursday, 10 September 2020 70% of Victorians approve of the way Premier Andrews is handling his job, but 76% say the Victorian Government should compensate small business The third Roy Morgan Snap SMS survey on Victoria’s Stage 4 restrictions shows 70% approval of Premier Daniel Andrews. However, a large majority (76%) of Victorians say the Victorian Government should provide compensation to all small businesses in Victoria forced to close by the Victorian Government’s COVID restrictions - only 24% say they should not. For the first time in three weeks of surveying a majority of Victorians 53% (up 6% in a week) say Melbourne residents should now be able to visit the homes of immediate family members. A rising majority of 67% (up 10%) of older Victorians aged 65+, say Melburnians should be able to visit the homes of their immediate family. This is despite being the age group at the greatest risk during the pandemic. Other groups, in which majorities say Melburnians should be able to visit their immediate families, include Melburnians (54%), Victorians aged under 35 (51%), aged 50-64 (54%), men (57%) and L-NP supporters (69%). Melburnians are far more likely than Country Victorians to want to be able to travel more than 5km from their home, visit their families and for the night-time curfew in Melbourne to end. Importantly, a slim majority of 51% of Melburnians now say they should be free to travel more than 5km from their home – up from 45% a week ago. -

Three Education Ministers with Public Primary School Backgrounds
AUSTRALIAN COUNCIL FOR THE DEFENCE OF GOVERNMENT SCHOOLS PRESS RELEASE 582# THREE EDUCATION MINISTERS WITH PUBLIC PRIMARY SCHOOL BACKGROUNDS : Rewards for the Public School Vote in the Victorian Election? Although the private, religious school lobby attempted to influence the outcome of the recent Victorian election, it was the disaffected public school voters, particularly in the neglected developing suburbs and inner city that decided the outcome. Education was a key election issue, with Labor making significant commitments to increase support and funding for public TAFEs, schools and preschools. However, it should be noted that Labor also attempted to ‘buy’the religious vote with a promise of $120 m for expanded facilities. James Merlino, like the Labor Party is Janus faced – facing both ways. Yet when the Catholic Education Office instructed Catholic parents to put the Greens last in the inner city electorates, they did the Greens a great service. Two members from those electorates are now sitting in the Victorian Parliament. And the victorious Labor Party has had the sense to replace the ex-Catholic school principal and administrator, Liberal Education Minister Dixon, with someone who has at least a primary school public education- James Merlino. Deputy Premier Merlino is joined by two other Ministers who have public school experiences. They are: Steve Herbert as Minister for Skills and Training and Jenny Mikakos as Minister for Children and Families, Youth Affairs 1 DOGS note the following CVs for the three Labor Ministers involved with education: 1. JAMES MERLINO: James Merlino was born 19 August 1972. He notes that he attended St Edmonds Public School 1978-1984 , Mt Lilydale College 1985-1990 and received a BA (Hons) 1996 (The University of Melbourne). -
The Essential Report 10 August 2020
The Essential Report 10 August 2020 ESSENTIALMEDIA.COM.AU ESSENTIALMEDIA.COM.AU The Essential Report Date: 10/08/2020 Prepared By: Essential Research Data Supplied by: Our researchers are members of the Australian Market and Social Research Society. Page 2 / 24 ESSENTIALMEDIA.COM.AU About this poll This report summarises the results of a fortnightly omnibus conducted by Essential Research with data provided by Qualtrics. The survey was conducted online from 6th to 9th August 2020 and is based on 1,010 respondents. The methodology used to carry out this research is described in the appendix at the end of the report. Note that due to rounding, not all tables necessarily total 100% and subtotals may also vary. Page 3 / 24 ESSENTIALMEDIA.COM.AU Performance of Scott Morrison Q Do you approve or disapprove of the job Scott Morrison is doing as Prime Minister? Aug’20 Jul’20 Jun’20 May’20 Apr’20 Mar’20 Feb’20 Jan’20 Dec’19 Nov’19 Oct’19 Sep’19 TOTAL: Approve 66% 63% 65% 64% 59% 41% 39% 40% 45% 45% 47% 49% TOTAL: Disapprove 23% 27% 26% 27% 31% 49% 52% 52% 43% 41% 38% 36% Don’t know 11% 10% 8% 9% 10% 10% 9% 8% 13% 13% 15% 15% Base (n) 1,010 1,054 1,059 1,093 1,069 1,096 1,056 1,081 1,035 1,075 1,088 1,093 Federal Voting Intention Total Labor Coalition Greens TOTAL: Other Strongly approve 24% 15% 46% 2% 14% Approve 42% 40% 45% 39% 47% Disapprove 14% 20% 4% 37% 16% Strongly disapprove 9% 15% 2% 17% 10% Don’t know 11% 10% 4% 5% 14% TOTAL: Approve 66% 56% 91% 40% 61% TOTAL: Disapprove 23% 35% 6% 54% 26% Base (n) 1,010 311 413 78 94 - The Prime Minister’s approval rating is on par with the previous month, now at 66% compared to 63% in July. -

Over Policing; the Need for Execuitive Accountability During the Covid-19 Crisis
Inquiry into the Victorian Government's Response to the COVID-19 Pandemic Submission no. 20 OVER POLICING; THE NEED FOR EXECUITIVE ACCOUNTABILITY DURING THE COVID-19 CRISIS JACQUELINE WRIGHT I INTRODUCTION Following the Victorian Government’s health response to the COVID-19 pandemic, the Public Accounts and Estimates Committee have commenced a public inquiry to consider the effectiveness of the Victorian Government approach.1 This submission addresses the terms of reference of the inquiry by considering the lack of transparency surrounding Victoria’s over policing of vulnerable communities in response to the COVID-19 crisis. This submission considers this lack of transparency around the policing of assembly and movement, in light of executive responsibility as a principle of public law. This submission argues that the Victorian response to the COVID-19 crisis lacks transparency and effective reporting necessary for executive accountability. II EXECUTIVE AUTHORITY Whilst it is important for the Executive Government to be capable of and empowered to respond to a crisis be it war, natural disaster, financial crisis,2 or indeed a health emergency, a level of accountability is essential to prevent an executive power grab. In ascertaining the scope of power of the executive, the cautionary words of Dixon J come to mind: History and not only ancient history, shows that in countries where democratic institutions have been unconstitutionally superseded, it has been done not seldom by those holding the executive power. Forms of government may need -

Help Save Quality Disability Services in Victoria HACSU MEMBER CAMPAIGNING KIT the Campaign Against Privatisation of Public Disability Services the Campaign So Far
Help save quality disability services in Victoria HACSU MEMBER CAMPAIGNING KIT The campaign against privatisation of public disability services The campaign so far... How can we win a This is where we are up to, but we still have a long way to go • Launched our marginal seats campaign against the • We have been participating in the NDIS Taskforce, Andrews Government. This includes 45,000 targeted active in the Taskforce subcommittees in relation to phone calls to three of Victoria’s most marginal seats the future workforce, working on issues of innovation quality NDIS? (Frankston, Carrum and Bentleigh). and training and building support against contracting out. HACSU is campaigning to save public disability services after the Andrews Labor • Staged a pre-Christmas statewide protest in Melbourne; an event that received widespread media • We are strongly advocating for detailed workforce Government’s announcement that it will privatise disability services. There’s been a wide attention. research that looks at the key issues of workforce range of campaign activities, and we’ve attracted the Government’s attention. retention and attraction, and the impact contracting • Set up a public petition; check it out via out would have on retention. However, to win this campaign, and maintain quality disability services for Victorians, dontdisposeofdisability.org, don’t forget to make sure your colleagues sign! • We have put forward an important disability service we have to sustain the grassroots union campaign. This means, every member has to quality policy, which is about the need for ongoing contribute. • HACSU is working hard to contact families, friends and recognition of disability work as a profession, like guardians of people with disabilities to further build nursing and teaching, and the introduction of new We need to be taking collective and individual actions. -

AUSTRALIAN EDUCATION UNION Victorian Labor
AUSTRALIAN EDUCATION UNION Victorian Branch Victorian Labor MPs We want you to email the MP in the electoral district where your school is based. If your school is not in a Labor held area then please email a Victorian Labor upper house MP who covers your area from the separate list below. Click here if you need to look it up. Email your local MP and cc the Education Minister and the Premier Legislative Assembly MPs (lower house) ELECTORAL DISTRICT MP NAME MP EMAIL MP TELEPHONE Albert Park Martin Foley [email protected] (03) 9646 7173 Altona Jill Hennessy [email protected] (03) 9395 0221 Bass Jordan Crugname [email protected] (03) 5672 4755 Bayswater Jackson Taylor [email protected] (03) 9738 0577 Bellarine Lisa Neville [email protected] (03) 5250 1987 Bendigo East Jacinta Allan [email protected] (03) 5443 2144 Bendigo West Maree Edwards [email protected] 03 5410 2444 Bentleigh Nick Staikos [email protected] (03) 9579 7222 Box Hill Paul Hamer [email protected] (03) 9898 6606 Broadmeadows Frank McGuire [email protected] (03) 9300 3851 Bundoora Colin Brooks [email protected] (03) 9467 5657 Buninyong Michaela Settle [email protected] (03) 5331 7722 Activate. Educate. Unite. 1 Burwood Will Fowles [email protected] (03) 9809 1857 Carrum Sonya Kilkenny [email protected] (03) 9773 2727 Clarinda Meng -
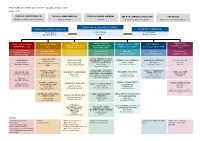
DPC-Org-Chart-April-2021.Pdf
DEPARTMENT OF PREMIER AND CABINET— ORGANISATIONAL CHART 12 April 2021 THE HON. DANNY PEARSON THE HON. JAMES MERLINO THE HON. DANIEL ANDREWS THE HON. GABRIELLE WILLIAMS TIM PALLAS Minister for Government Services Deputy Premier Premier Minister for Aboriginal Affairs Minister for Industrial Relations DEPARTMENT OF PREMIER AND CABINET RECOVERY TRACKING & ANALYTICS OFFICE OF THE SECRETARY Marcus Walsh Jeremi Moule Jane Gardam Executive Director Secretary Executive Director CABINET, SOCIAL POLICY & INDUSTRIAL LEGAL, LEGISLATION & DIGITAL VICTORIA ECONOMIC POLICY & STATE FIRST PEOPLES— COMMUNICATIONS & INTERGOVERNMENTAL RELATIONS VICTORIA GOVERNANCE (LLG) (DV) PRODUCTIVITY (EPSP) STATE RELATIONS (FPSR) CORPORATE (CCC) RELATIONS (SPIR) (IRV) Toby Hemming Vivien Allimonos Vivien Allimonos Kate Houghton Tim Ada Elly Patira Matt O’Connor Deputy Secretary & A/ Chief Executive Officer Deputy Secretary Deputy Secretary Deputy Secretary A/ Deputy Secretary Deputy Secretary General Counsel CYBERSECURITY COVID COORDINATION & GOVERNANCE CABINET OFFICE PERFORMANCE / FAMILIES, ECONOMIC DEVELOPMENT ABORIGINAL VICTORIA PRIVATE SECTOR John O’Driscoll Vicky Hudson FAIRNESS & HOUSING Sophie Colquitt Tim Kanoa Lissa Zass Chief Information Security Rachel Cowling Executive Director Lucy Toovey A/ Executive Director Executive Director Director Officer A/ Executive Director Executive Director DIGITAL DESIGN & EDUCATION / JUSTICE / TREATY / ABORIGINAL OFFICE OF THE COMMUNITY SECURITY & ECONOMIC STRATEGY PUBLIC SECTOR INNOVATION CORPORATE GOVERNANCE AFFAIRS POLICY -

Inquiry Into the Victorian Government's Response to the COVID-19 Pandemic
PARLIAMENT OF VICTORIA Public Accounts and Estimates Committee Inquiry into the Victorian Government’s response to the COVID-19 pandemic Parliament of Victoria Public Accounts and Estimates Committee Ordered to be published VICTORIAN GOVERNMENT PRINTER February 2021 PP No 203, Session 2018-2021 ISBN 978 1 922425 18 8 (print version), 978 1 922425 19 5 (PDF version) Committee membership CHAIR DEPUTY CHAIR Lizzie Blandthorn Richard Riordan Sam Hibbins David Limbrick Pascoe Vale Polwarth Prahran South Eastern Metropolitan Gary Maas Danny O’Brien Pauline Richards Tim Richardson Narre Warren South Gippsland South Cranbourne Mordialloc Ingrid Stitt Nina Taylor Bridget Vallence Western Metropolitan Southern Metropolitan Evelyn PAEC member until PAEC member from 13 October 2020 14 October 2020 ii Public Accounts and Estimates Committee About the Committee Functions The Public Accounts and Estimates Committee is a joint parliamentary committee constituted under the Parliamentary Committees Act 2003 (the Act). The Committee comprises ten members of Parliament drawn from both Houses of Parliament. The Committee carries out investigations and reports to Parliament on matters associated with the financial management of the State. Its functions under the Act are to inquire into, consider and report to the Parliament on: • any proposal, matter or thing concerned with public administration or public sector finances • the annual estimates or receipts and payments and other Budget papers and any supplementary estimates of receipts or payments presented to the Assembly and the Council • audit priorities for the purposes of the Audit Act 1994. The Committee also has a number of statutory responsibilities in relation to the Office of the Auditor-General and Parliamentary Budget Office. -

Clicking Here
Victorian Election 2018: Exit Poll Victorian State Election 2018: Exit Poll November 28, 2018 Methodology The following graphs are based on two virtual focus groups. The first of 90 voters in this year’s Victorian election which was selected from a larger group of 186 respondents to reflect voting intentions based on the results of the election as displayed on the Victorian Electoral Commission’s website on Monday November 26, 2018. The second from responses to a previous survey undertaken between November 10 and November 16, 2018 resulting in a virtual focus group of 100. Details of that report can be downloaded from here1. Results should be taken as indicative in that the sample is not properly randomised, but it is unlikely that groups are completely unrepresentative. The second poll was conducted from Saturday November 24 through to Sunday November 25, 2018 using our online panel of over 13,000 Australian voters. Quantitative analysis was undertaken using Microsoft Excel. Qualitative analysis was undertaken using Leximancer. For further information contact Graham Young 0411 104 801. 1https://aip.asn.au/2018/11/qualitative-polling-on-victorian-election/ 1 Victorian State Election 2018: Exit Poll November 28, 2018 Executive Summary Mixed and baked in Victoria Daniel Andrews’ boil-over result in Victoria was unheralded by any of the polling organisations, including ours. This is probably a result of a significant part of the swing occurring late in the election. In our initial analysis we relied on Newspoll for voting intention across the whole population, which at that stage last polled Victoria in April 20182. -

Extract from Book 14)
PARLIAMENT OF VICTORIA PARLIAMENTARY DEBATES (HANSARD) LEGISLATIVE ASSEMBLY FIFTY-EIGHTH PARLIAMENT FIRST SESSION Wednesday, 7 October 2015 (Extract from book 14) Internet: www.parliament.vic.gov.au/downloadhansard By authority of the Victorian Government Printer The Governor The Honourable LINDA DESSAU, AM The Lieutenant-Governor The Honourable Justice MARILYN WARREN, AC, QC The ministry Premier ......................................................... The Hon. D. M. Andrews, MP Deputy Premier and Minister for Education .......................... The Hon. J. A. Merlino, MP Treasurer ....................................................... The Hon. T. H. Pallas, MP Minister for Public Transport and Minister for Employment ............ The Hon. J. Allan, MP Minister for Small Business, Innovation and Trade .................... The Hon. P. Dalidakis, MLC Minister for Industry, and Minister for Energy and Resources ........... The Hon. L. D’Ambrosio, MP Minister for Roads and Road Safety, and Minister for Ports ............. The Hon. L. A. Donnellan, MP Minister for Tourism and Major Events, Minister for Sport and Minister for Veterans .................................................. The Hon. J. H. Eren, MP Minister for Housing, Disability and Ageing, Minister for Mental Health, Minister for Equality and Minister for Creative Industries ........... The Hon. M. P. Foley, MP Minister for Emergency Services, and Minister for Consumer Affairs, Gaming and Liquor Regulation .................................. The Hon. J. F. Garrett, MP Minister for Health and Minister for Ambulance Services .............. The Hon. J. Hennessy, MP Minister for Training and Skills .................................... The Hon. S. R. Herbert, MLC Minister for Local Government, Minister for Aboriginal Affairs and Minister for Industrial Relations ................................. The Hon. N. M. Hutchins, MP Special Minister of State .......................................... The Hon. G. Jennings, MLC Minister for Families and Children, and Minister for Youth Affairs ..... -

Annual Report 2014-15
V C O S S A N N U A L R E P O R T 2 0 1 4 - 2 0 1 5 1 From the President 2 From the CEO 3 Advocate for social justice 5 Reports published and submissions made 6 Build a strong community sector 8 Strengthen our public presence 10 VCOSS blogs and media releases 12 Collaborate for greater impact 14 Sustain a healthy organisation 15 VCOSS Board 2014–15 16 Staff, Funders, Partners and Supporters 17 VCOSS Members 2014–15 18 Treasurer’s report 19 Financial statements For more information about VCOSS or to become a member, contact: Victorian Council of Social Service Level 8, 128 Exhibition Street, Melbourne, Victoria, 3000 T: +61 3 9235 1000 Freecall: 1800 133 340 F: 03 9654 5749 W: www.vcoss.org.au E: [email protected] Twitter: @vcoss Authorised by: Emma King, Chief Executive Officer © Copyright 2015 Victorian Council of Social Service Printing: Officeworks Design: Louisa Roubin Enquiries: Kellee Nolan, Publications Editor E: [email protected] ISSN 1324 8588 ABN 23 005 014 988 1 From the President Both the present and the future have been firmly on the agenda at VCOSS this year. We have advocated strongly for social justice, while also casting our view forward to develop a strategy that strengthens the community’s voice against poverty and inequality into the future. On behalf of the board I would like to express our appreciation for the efforts of all VCOSS staff, under the outstanding leadership of our Chief Executive Officer Emma King, and our new Deputy Chief Executive Officer Mary Sayers, for their work in partnership with members and people with lived experience of poverty and disadvantage, to present wide-ranging policy, research and solutions, and create a powerful voice against poverty and inequality. -
Department of Premier and Cabinet 2015 16 Annual Report
Image provided courtesy of the Victorian Parliament The Victorian Parliament House lit in rainbow colours as a tribute to the victims of the Orlando shootings on 12 June 2016. In the Victorian Parliament on 24 May 2016, the Hon. Daniel Andrews MP made a formal apology to Victoria’s gay community for historic convictions under unjust laws against homosexual acts. The Department of Premier and Cabinet is committed to fostering LGBTI equality and working with other agencies, partners and citizens to improve the lives of LGBTI Victorians. DPC’s Equality branch fosters and promotes lesbian, gay, bisexual, transgender and intersex (LGBTI) equality in the Victorian community. The branch provides advice and support to the Premier, the Minister for Equality and the Victorian Commissioner for Gender and Sexuality to drive whole-of-government LGBTI policy. TABLE OF CONTENTS SECTION ONE: Overview 3 SECTION TWO: Our performance 16 SECTION THREE: Financial statements 42 SECTION FOUR: Appendices 101 SECTION ONE: OVERVIEW 1 Accountable officer’s declaration In accordance with the Financial Management Act 1994, I am pleased to present the Department of Premier and Cabinet’s annual report for the year ending 30 June 2016. Chris Eccles Secretary September 2016 2 DEPARTMENT OF PREMIER AND CABINET 2015–16 ANNUAL REPORT SECTION ONE Overview Accountable officer’s declaration 2 ABOUT US 4 Our vision 4 Departmental objectives 4 Our values 5 Who we are 6 Our services 6 OUR MINISTERS 7 Premier of Victoria 7 Special Minister of State 7 Minister for Multicultural