2020 Pharmacy Benefits
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Migraine Specialty Care Program Tm
MIGRAINE SPECIALTY CARE PROGRAM TM Phone: 833-796-6470 • Fax: 844-841-3401 Community Led Specialty Pharmacy Care 1 PATIENT INFORMATION: 2 PRESCRIBER INFORMATION: Name: ___________________________________________________ Name: ___________________________________________________ Address: _________________________________________________ Address: _________________________________________________ City: _________________________ State: ____ Zip: ____________ City: _________________________ State: ____ Zip: ____________ Phone: ___________________ Alt. Phone: ____________________ Phone: _____________________ Fax: _______________________ Email: ____________________________________________________ NPI: ________________________ DEA: _______________________ DOB: ___________ Gender: M F Caregiver: _____________ Tax I.D.: __________________________________________________ Height: ________ Weight: ________ Allergies: ________________ Office Contact: __________________ Phone: __________________ 3 STATEMENT OF MEDICAL NECESSITY: (Please Attach All Medical Documentation) Prior Failed Indicate Drug Name v10.0_060821 Length of Symptoms: ___________________________ ICD-10: _________________________ Treatments: and Length of Treatment: Other diagnosis _______________ Number of Migraine Days per month: ________________ Preventative: Headache Days per month: _________________ Migraine Hours per day: __________________ ACE-I/ARBs ___________________ Patient has been evaluated and does not have medication overuse headache? No Yes Antiepileptics ___________________ -

California Essential Drug List
California Essential Drug List The Essential Drug List (formulary) includes a list of drugs covered by Health Net. The drug list is updated at least monthly and is subject to change. All previous versions are no longer in effect. You can view the most current drug list by going to our website at www.healthnet.com. Refer to Evidence of Coverage or Certificate of Insurance for specific cost share information. For California Individual & Family Plans: Drug Lists Select Health Net Large Group – Formulary (pdf). For Small Business Group: Drug Lists Select Health Net Small Business Group – Formulary (pdf). NOTE: To search the drug list online, open the (pdf) document. Hold down the “Control” (Ctrl) and “F” keys. When the search box appears, type the name of your drug and press the “Enter” key. If you have questions or need more information call us toll free. California Individual & Family Plans (off-Exchange) If you have questions about your pharmacy coverage call Customer Service at 1-800-839-2172 California Individual & Family Plans (on-Exchange) If you have questions about your pharmacy coverage call Customer Service at 1-888-926-4988 Hours of Operation 8:00am – 7:00pm Monday through Friday 8:00am – 5:00pm Saturday Small Business Group If you have questions about your pharmacy coverage call Customer Service at 1-800-361-3366 Hours of Operation 8:00am – 6:00pm Monday through Friday Updated September 1, 2021 Health Net of California, Inc. and Health Net Life Insurance Company are subsidiaries of Health Net, LLC and Centene Corporation. Health Net is a registered service mark of Health Net, LLC Table of Contents What If I Have Questions Regarding My Pharmacy Benefit? ................................... -

DDT Cover/Back April 2006.Qx
March 2007 Vol 7 No 3 www.drugdeliverytech.com IN THIS ISSUE INTERVIEW WITH DPT’S PRESIDENT MR. PAUL JOHNSON In Situ Gel Systems 30 Mitan Gokulgandhi, BPharm Dharmesh M. Modi, MPharm COX-II Microspheres 38 Lakshmi Sivasubramanian Madhumathi Seshadri Undermining CEO’s 82 John A. Bermingham FEATURING Parkinson’s Disease 59 Steven Damon Yogi R. Patel The science & business of specialty pharma, biotechnology, and drug delivery Specialty Pharma Indices 64 Dr. Barath Christopher Avani Amin, Josef Bossart, PhD Shankar Robinson, PhD Drug Delivery’s PhD Current Status of Clinical Trials Increasing New Ways to Non-Invasive In Asia 68 Importance to Partner With Insulin Delivery Ames Gross, MBA Big Pharma & the Federal Technologies Specialty Pharma Government Momoko Hirose March 2007 Vol 7 No 3 PUBLISHER/PRESIDENT Ralph Vitaro EXECUTIVE EDITORIAL DIRECTOR Dan Marino, MSc [email protected] CREATIVE DIRECTOR Shalamar Q. Eagel CONTROLLER Debbie Carrillo CONTRIBUTING EDITORS Cindy H. Dubin Debra Bingham Jason McKinnie TECHNICAL OPERATIONS Mark Newland EDITORIAL SUPPORT Nicholas D. Vitaro ADMINISTRATIVE SUPPORT Kathleen Kenny Corporate/Editorial Office 219 Changebridge Road, Montville, NJ 07045 Tel: (973)299-1200 Fax: (973) 299-7937 www.drugdeliverytech.com Advertising Sales Offices East & Midwest Victoria Geis - Account Executive Cheryl S. Stratos - Account Executive 103 Oronoco Street, Suite 200 Alexandria, VA 22314 Tel: (703) 212-7735 Fax: (703) 548-3733 E-mail: [email protected] E-mail: [email protected] West Coast Warren -
Medication Permission Form
CHARDON LOCAL SCHOOLS MEDICATION PERMISSION FORM Student Name :__________________________________________ Grade/Class _______ Teacher :______________________ School ____________________ Student Address:____________________________________________________________________________ Date of Birth____________________________ TO BE COMPLETED BY HEALTH CARE PROVIDER Please print clearly and complete ALL sections. Time/Frequency Adverse Reaction to Report to (Include minimum time Physician and/or Special Name of Medication Dose Route (circle) Interval for prn dosing) Reason for Medication Start Date Stop Date Instructions Tablet/Capsule PO Liquid PO _________________ __/__/__ ___/___/___ Inhaler/Nebulizer OR OR Other__________ As needed every __hrs. ___ End of School year Tablet/Capsule PO Liquid PO _________________ __/__/__ ___/___/___ Inhaler/Nebulizer OR OR Other__________ As needed every __hrs ___ End of School year EPINEPHRINE AUTOINJECTOR Not Applicable SELF -CARRY AUTHORIZATION Yes, as the prescriber I have determined that this student is capable of possessing and using this autoinjector appropriately and have provided the student with training in the proper use of the autoinjector. ASTHMA INHALER Not Applicable SELF -CARRY AUTHORIZATION Yes, as the prescriber I have determined that this student to capable of possessing and using this inhaler appropriately and have provided the student with training in the proper use of the inhaler. Reminder note for prescriber: ORC 3313.718 requires backup epinephrine autoinjector and best practice recommends backup asthma inhaler Health Care Provider Name _______________________________________ Health Care Provider Signature: ______________________________________ Date_________________ Phone Number: _______________________________________ Fax Number: _________________________________________ TO BE COMPLETED BY PARENT OR GUARDIAN I authorize an employee of the school board to administer the above medication. I understand that additional parent/prescriber signed statements will be necessary if the dosage of medication is changed. -
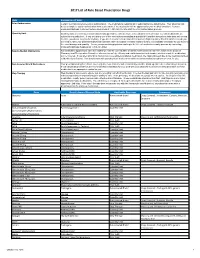
2017 List of Rule Based Prescription Drugs
2017 List of Rule Based Prescription Drugs Rule Explanation of Rule Prior Authorization Certain medications require a prior authorization. The medications requiring prior authorization are listed below. Your physician will need to complete a prior authorization form to determine if the medication will be approved for your medical condition. Contact EnvisionRXOptions Customer Service Help Desk at 1-800-361-4542 to start the Prior Authorization process. Quantity Limit Quantity limits are clinically recommended limits put in place to help ensure safe utilization of medication. Certain medications are subject to a quantity limit. If you are taking one of the medications mandating a quantity limit and the amount you take does not exceed the limit, you do not need to do anything. If you are in need of a medication that requires a higher quantity than that which is listed, you will need to have your prescribing physician submit a letter of medical necessity explaining why it is medically necessary for you to be on the exact dosage and quantity. You or your prescribing physician can begin the letter of medical necessity process by contacting EnvisionRXOptions Helpdesk at 1-800-361-4542. New-to-Market Medications Any medication approved to enter the market will only be covered after a clinical review decision has been made by the Envision Pharmacy and Therapeutics Committee who reviews safety, efficacy and cost information to determine whether or not the medication will be covered. If you attempt to fill or claim a non-covered New-to-Market medication, the claim will reject due to the medications New- to-Market classification. -
Medi-Cal Formulary May 2020
Formulary Medi-Cal MAY 2020 The IEHP Medi-Cal Formulary is subject to change throughout the year. All previous versions of the formulary are no longer in effect once a new formulary is available. The IEHP Medi-Cal Formulary can be found at: www.iehp.org/en/members/medical Last Updated: 04/17/2020 Inland Empire Health Plan (IEHP) Medi-Cal Formulary Table of Contents A . Foreword ..................................................................................................................... 2 B. IEHP Member Services .............................................................................................. 2 C. How to Use the Formulary .......................................................................................... 2 D. Prescription Coverage ................................................................................................. 3 D1. Quantity Limits .................................................................................................... 3 D2. Step Therapy ........................................................................................................ 3 E. Filling a Prescription and IEHP’s Pharmacy Network ............................................... 4 F. Definitions ................................................................................................................... 4 G. List of Covered Drugs .............................................................................................. 10 H. Index ....................................................................................................................... -

Inhalation Drug Delivery Devices: Technology Update
Medical Devices: Evidence and Research Dovepress open access to scientific and medical research Open Access Full Text Article REVIEW Inhalation drug delivery devices: technology update Mariam Ibrahim Abstract: The pulmonary route of administration has proven to be effective in local and Rahul Verma systemic delivery of miscellaneous drugs and biopharmaceuticals to treat pulmonary and non- Lucila Garcia-Contreras pulmonary diseases. A successful pulmonary administration requires a harmonic interaction between the drug formulation, the inhaler device, and the patient. However, the biggest single Department of Pharmaceutical Sciences, College of Pharmacy, problem that accounts for the lack of desired effect or adverse outcomes is the incorrect use The University of Oklahoma Health of the device due to lack of training in how to use the device or how to coordinate actuation Sciences Center, Oklahoma City, and aerosol inhalation. This review summarizes the structural and mechanical features of OK, USA aerosol delivery devices with respect to mechanisms of aerosol generation, their use with different formulations, and their advantages and limitations. A technological update of the current state-of-the-art designs proposed to overcome current challenges of existing devices is also provided. Keywords: pulmonary delivery, asthma, nebulizers, metered dose inhaler, dry powder inhaler Introduction Inhalation therapy has been used for thousands of years, albeit in a different form and use. Inhalation therapy was practiced by ancient civilizations in Egypt, Greece, India, and People’s Republic of China as evidenced by different artifacts displayed in museums, that may be considered the first used inhalation devices.1,2 Currently, inhalation therapy is the best option for lung diseases like asthma, cystic fibrosis, and chronic obstructive pulmonary disease (COPD). -

Olodaterol Monograph
Olodaterol Monograph Olodaterol (Striverdi Respimat) National Drug Monograph VA Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives The purpose of VA PBM Services drug monographs is to provide a comprehensive drug review for making formulary decisions. Updates will be made when new clinical data warrant additional formulary discussion. Documents will be placed in the Archive section when the information is deemed to be no longer current. FDA Approval Information Description/Mechan Olodaterol is a long-acting beta2-adrenergic agonist (LABA). Binding to and activating ism of Action beta2-adrenoceptors in the airways results in stimulation of intracellular adenyl cyclase, an enzyme that mediates the synthesis of cyclic-3’, 5’ adenosine monophosphate (cAMP). Elevated levels of cAMP induce bronchodilation by relaxation of airway smooth muscle cells. Indication(s) Under Long-term once daily maintenance bronchodilator treatment of airflow obstruction in Review patients with COPD including chronic bronchitis and/or emphysema Dosage Form(s) Inhalation spray for oral inhalation via Respimat (a soft-mist inhaler) Under Review The soft-mist inhalers (SMI) provide multi-dose medication using liquid formulations similar to that used in nebulizers and are propellant-free. Presently, Respimat is the only SMI commercially available for clinical use. The soft mist is released at a slower velocity and has more prolonged spray duration than the mist produced from pressurized metered dose inhalers (pMDIs). Pressurized MDIs require coordination of actuation with inhalation which may be difficult for some patients partly due to the rapid speed at which the drug is delivered and the short duration of the mist. -

Preventive Drug List
navitus.com Share a Clear View Preventive Drug List Updated July 2021 Your health plan is making an effort to reduce your health care costs by giving you tools to help you stay healthy and productive. Below are the medications included on your Preventive Drug List. These medications help protect against or manage some high risk medical conditions. Taking these medications as directed by your prescriber can help avoid serious health problems. That may mean fewer doctor visits and hospitalizations, reducing your total health care costs. In the drug list below, generic drugs are shown in lowercase type. Brand name drugs are shown in uppercase type. Antiasthmatic/Bronchodilators theophylline soln ADVAIR DISKUS INHALER *generic Wixela only for wixela inhaler *brand Advair Diskus only for non-HDHP plans* HDHPs* ADVAIR HFA INHALER Anticoagulant albuterol/ipratropium neb soln ELIQUIS TAB aminophylline tab PRADAXA CAP ARNUITY ELLIPTA INHALER warfarin tab ASMANEX HFA INHALER XARELTO TAB ASMANEX INHALER Antidiabetics budesonide inh susp acarbose tab FLOVENT DISKUS INHALER chlorpropamide tab FLOVENT HFA INHALER glimepiride tab fluticasone/salmeterol inhaler glipizide ER tab ipratropium neb soln glipizide tab METAPROTERENOL SYRUP glipizide/metformin tab montelukast chew tab glyburide micronized tab montelukast tab glyburide tab THEOCHRON glyburide/metformin tab theophylline CR tab metformin ER tab theophylline ER tab metformin tab • Note: The list is subject to change and not all drugs listed may be covered on your formulary. Please refer to your Navitus -

Connecticut Medicaid
ACNE AGENTS, TOPICAL ‡ ANGIOTENSIN MODULATOR COMBINATIONS ANTICONVULSANTS, CONT. CONNECTICUT MEDICAID (STEP THERAPY CATEGORY) AMLODIPINE / BENAZEPRIL (ORAL) LAMOTRIGINE CHEW DISPERS TAB (not ODT) (ORAL) (DX CODE REQUIRED - DIFFERIN, EPIDUO and RETIN-A) AMLODIPINE / OLMESARTAN (ORAL) LAMOTRIGINE TABLET (IR) (not ER) (ORAL) Preferred Drug List (PDL) ACNE MEDICATION LOTION (BENZOYL PEROXIDE) (TOPICAL)AMLODIPINE / VALSARTAN (ORAL) LEVETIRACETAM SOLUTION, IR TABLET (not ER) (ORAL) • The Connecticut Medicaid Preferred Drug List (PDL) is a BENZOYL PEROXIDE CREAM, WASH (not FOAM) (TOPICAL) OXCARBAZEPINE TABLET (ORAL) listing of prescription products selected by the BENZOYL PEROXIDE 5% and 10% GEL (OTC) (TOPICAL) ANTHELMINTICS PHENOBARBITAL ELIXIR, TABLET (ORAL) Pharmaceutical and Therapeutics Committee as efficacious, BENZOYL PEROXIDE 6% CLEANSER (OTC) (TOPICAL) ALBENDAZOLE TABLET (ORAL) PHENYTOIN CHEW TABLET, SUSPENSION (ORAL) safe and cost effective choices when prescribing for HUSKY CLINDAMYCIN PH 1% PLEGET (TOPICAL) BILTRICIDE TABLET (ORAL) PHENYTOIN SOD EXT CAPSULE (ORAL) A, HUSKY C, HUSKY D, Tuberculosis (TB) and Family CLINDAMYCIN PH 1% SOLUTION (not GEL or LOTION) (TOPICAL)IVERMECTIN TABLET (ORAL) PRIMIDONE (ORAL) Planning (FAMPL) clients. CLINDAMYCIN / BENZOYL PEROXIDE 1.2%-5% (DUAC) (TOPICAL) SABRIL 500 MG POWDER PACK (ORAL) • Preferred or Non-preferred status only applies to DIFFERIN 0.1% CREAM (TOPICAL) (not OTC GEL) (DX CODE REQ.) ANTI-ALLERGENS, ORAL SABRIL TABLET (ORAL) those medications that fall within the drug classes DIFFERIN -

Instructions For
Instructions for Use Please see page 2 Instructions for Use Please see page 3 SIMPONI® (SIM-po-nee) (golimumab) SIMPONI® (SIM-po-nee) (golimumab) SmartJect® autoinjector Prefilled Syringe SINGLE-DOSE Important Important If your doctor decides that you or a caregiver may be able to give your SIMPONI® injections at home, you should SIMPONI® comes as a single-dose prefilled syringe containing one 50 mg or one 100 mg dose. Each SIMPONI® prefilled receive training on the right way to prepare and inject SIMPONI® using SmartJect®. syringe can only be used one time. Throw away (dispose of) the used prefilled syringe (See Step 3) after one dose, even Do not try to inject SIMPONI® yourself until you have been shown the right way to give the injections by your doctor if there is medicine left in it. Do not reuse your SIMPONI® prefilled syringe. or nurse. If your healthcare provider decides that you or a caregiver may be able to give your injections of SIMPONI® at home, Please read this Instructions for Use before using SIMPONI® SmartJect® and each time you get a refill. There may be you should receive training on the right way to prepare and inject SIMPONI® using the prefilled syringe before new information. This leaflet does not take the place of talking with your doctor about your medical condition or attempting to inject. Do not try to inject yourself until you have been shown the right way to give the injections by your your treatment. healthcare provider. Read this Instructions for Use before using your SIMPONI® prefilled syringe and each time you get a refill. -

New Autoinjector Technology for the Delivery of Subcutaneous Methotrexate in the Treatment of Rheumatoid Arthritis
Expert Review of Medical Devices ISSN: 1743-4440 (Print) 1745-2422 (Online) Journal homepage: http://www.tandfonline.com/loi/ierd20 New autoinjector technology for the delivery of subcutaneous methotrexate in the treatment of rheumatoid arthritis Michael Schiff, Jonathan Jaffe, Bruce Freundlich & Patrick Madsen To cite this article: Michael Schiff, Jonathan Jaffe, Bruce Freundlich & Patrick Madsen (2014) New autoinjector technology for the delivery of subcutaneous methotrexate in the treatment of rheumatoid arthritis, Expert Review of Medical Devices, 11:5, 447-455, DOI: 10.1586/17434440.2014.929492 To link to this article: http://dx.doi.org/10.1586/17434440.2014.929492 Published online: 17 Jun 2014. Submit your article to this journal Article views: 112 View related articles View Crossmark data Citing articles: 1 View citing articles Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ierd20 Download by: [Rosa Weiss] Date: 14 February 2017, At: 10:26 Device Profile New autoinjector technology for the delivery of subcutaneous methotrexate in the treatment of rheumatoid arthritis Expert Rev. Med. Devices 11(5), 447–455 (2014) Michael Schiff*1, Methotrexate (MTX) is the cornerstone of treatment for rheumatoid arthritis (RA), and is Jonathan Jaffe2, widely used both as first-line therapy and as an important component of long-term therapy. Bruce Freundlich3,4 Although subcutaneous MTX is typically delivered orally, parenteral administration offers benefits with respect to tolerability and systemic exposure, and may be an underutilized and Patrick Madsen5 treatment option. The RA patient population presents specific challenges for safe and 1 Department of Rheumatology, accurate administration of parenteral therapies, because of common symptoms of joint pain University of Colorado, Denver, CO, USA and limited manual dexterity.