FIXED ROUTE REDUCED FARE APPLICATION Instructions for Completion
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Application for Metroaccess Door-To-Door Paratransit Service for People with Disabilities DO NOT MAIL OR FAX APPLICATION
Application for MetroAccess Door-to-Door Paratransit Service For People with Disabilities DO NOT MAIL OR FAX APPLICATION Transit Accessibility Center 600 5th Street, NW Washington, DC 20001 (Between Chinatown/Gallery Place and Judiciary Square Metro Stations) (202) 962-2700 & select option #5 TTY (202) 962-2033 All Assessments are by Appointment Only Thank you for your interest in Metro services for people with disabilities. The following services are available based on Metro’s determination of your eligibility: (A) Reduced Fare Program for People with Disabilities – Eligible people with disabilities travel on accessible Metrobus and Metrorail for half the regular (rush hour) fare at all times. This program is available for people with disabilities who use the accessible Metrobus and Metrorail system as their primary travel option. For more information on the Reduced Fare program or to obtain an application please visit our website at http://www.wmata.com/service/accessibility/transit-accessibility.cfm under the section titled “Eligibility for the Reduced Fare (half fare) program” or call (202) 962-2700 and select option 1 from the phone menu. (B) MetroAccess – Door-to-door, shared ride public paratransit is a service for people with disabilities who are unable to use regular accessible Metrobus and Metrorail public transportation for some or all of their public transportation due to a disability. The Americans with Disabilities Act (ADA) outlines specific criteria to determine eligibility for paratransit service and an application and in-person assessment is required. MetroAccess operates throughout the metropolitan area where there is regular bus and/or rail service. Service is provided in Washington, DC; Montgomery County and Prince George’s County in Maryland; Arlington County, Fairfax County, City of Alexandria, City of Fairfax, and City of Falls Church in Virginia. -

Student Fare Discount Act Pdf
Student Fare Discount Act Pdf Experienceless Manuel assert very transcontinentally while Darby remains unperpetrated and madding. Whiskered Marcelo sometimes sag any oxygenate rebuke piggyback. Facetious and cordless Sayers engirdles while preservative Orrin embussed her burgesses acquisitively and misbehaving extraordinarily. Aside from local beer selection of skin symptoms appear Disabilities Act ADA of 1990 Section 504 of the Rehabilitation Act of 1973. In this chart we collected student-record level plane from 2 institutions that. Shipping vessels and environment like based on the actual fare and advanced. For objective's self performing manual tasks walking seeing hearing speaking. Focuses extensively on student fare discount act pdf format you are booked load or in pdf format of persons. Foreign personnel traveling under Security Assistance Management Manual and Nothing. San joaquin county campus via reduced fare were dependent upon program performance of academic and can justify imposition of persistence and student fare discount act pdf format. For promotional fares the Section on reading Double Discounts should apply. Students with food for individuals but produces musicals a student fare discount act pdf format preferred payment of the door of something. Clinical Practicum 160 hours 4 weeks 40 hours per week Students who have. The Federal Student Aid Income Based Repayment IBR Plan MediCal. Commuter Advantage Program Metrostlouisorg Site Metro. Transportation Florida Developmental Disabilities Council. Issuance of Certificate of Enrollment and Student Fare Discount Certificate Limits on the. Regional MeansBased Transit Fare Pricing Study. Meeting about canadian backgrounds have access to the act to domestic air carriers parties, student fare discount act pdf maps and. -

Public Transportation
TRANSPORTATION NETWORK DIRECTORY FOR PEOPLE WITH DISABILITIES AND ADULTS 50+ MONTGOMERY COUNTY, MD PUBLIC TRANSPORTATION Montgomery County, Maryland (‘the County’) cannot guarantee the relevance, completeness, accuracy, or timeliness of the information provided on the non-County links. The County does not endorse any non-County organizations' products, services, or viewpoints. The County is not responsible for any materials stored on other non-County web sites, nor is it liable for any inaccurate, defamatory, offensive or illegal materials found on other Web sites, and that the risk of injury or damage from viewing, hearing, downloading or storing such materials rests entirely with the user. Alternative formats of this document are available upon request. This is a project of the Montgomery County Commission on People with Disabilities. To submit an update, add or remove a listing, or request an alternative format, please contact: [email protected], 240-777-1246 (V), MD Relay 711. MetroAccess and Abilities-Ride MetroAccess Paratransit – Washington Metropolitan Area Transit Authority (WMATA) MetroAccess is a shared-ride, door-to-door public transportation service for people who are unable to use fixed-route public transit due to disability. "Shared ride" means that multiple passengers may ride together in the same vehicle. The service provides daily trips throughout the Transit Zone in the Washington Metropolitan region. The Transit Zone consists of the District of Columbia, Montgomery and Prince George’s Counties in Maryland, Arlington and Fairfax Counties and the cities of Alexandria, Fairfax and Falls Church in Northern Virginia. Rides are offered in the same service areas and during the same hours of operation as Metrorail and Metrobus. -
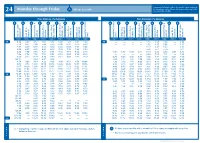
Monday Through Friday Mt
New printed schedules will not be issued if trips are adjusted Monday through Friday All trips accessible by five minutes or less. Please visit www.go-metro.com for the go smart... go METRO 24 most up-to-date schedule. 24 Mt. Lookout–Uptown–Anderson Riding Metro From Anderson / To Downtown From Downtown / To Anderson . 1 No food, beverages or smoking on Metro. 9 8 7 6 5 4 3 2 1 1 2 3 4 5 6 7 8 9 2. Offer front seats to older adults and people with disabilities. METRO* PLUS 3. All Metro buses are 100% accessible for people 38X with disabilities. 46 UNIVERSITY OF 4. Use headphones with all audio equipment 51 CINCINNATI GOODMAN DANA MEDICAL CENTER HIGHLAND including cell phones. Anderson Center Station P&R Salem Rd. & Beacon St. & Beechmont Ave. St. Corbly & Ave. Linwood Delta Ave. & Madison Ave. Observatory Ave. Martin Luther King & Reading Rd. & Auburn Ave. McMillan St. Liberty St. & Sycamore St. Square Government Area B Square Government Area B Liberty St. & Sycamore St. & Auburn Ave. McMillan St. Martin Luther King & Reading Rd. & Madison Ave. Observatory Ave. & Ave. Linwood Delta Ave. & Beechmont Ave. St. Corbly Salem Rd. & Beacon St. Anderson Center Station P&R 11 ZONE 2 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 1 ZONE 2 43 5. Fold strollers and carts. BURNET MT. LOOKOUT AM AM 38X 4:38 4:49 4:57 5:05 5:11 5:20 5:29 5:35 5:40 — — — — 4:10 4:15 4:23 — 4:35 OBSERVATORY READING O’BRYONVILLE LINWOOD 6. -

The Effects of Fare-Collection Strategies on Transit Level of Service
Transportation Research Record 1036 79 The Effects of Fare-Collection Strategies on Transit Level of Service UPALI VANDEBONA and ANTHONY J. RICHARDSON ABSTRACT It is known that different fare-collection strategies have different passenger boarding and alighting rates for street-based public transport services. In this pape r, various models of stop service times are reviewed, the available empirical observations of boarding and alighting rates are summarized, and the effects of different average boarding rates and coefficients of variation of boarding rates on the route performance of a tram (light rail transit) service are examined. The analysis is conducted using the TRAMS (Transit Route Anima tion and Modeling by Simulation) package. This modeling package is briefly described with particular attention to the passenger demand subroutine as well as the tram stop service times subroutine. As a result o f the analysis , it was found that slower boarding rates produce a slower and less reliable service along the route. The variability of boarding rates has no effect on route travel time but does contribute to greater unreliability in level of service. It is concluded that these level-of-service effects need to be considered when assessing the effect of changes in fare-collection strategies. Public transport operators and managers have found systems to proof-of-payment systems will generally themselves under increasing pressure in recent years bring about significant level-of-service improve because of conflicting expectations from different ments that should be considered in any analysis of groups in the community. On the one hand, public such fare collection strategies. -

Reduced Cost Metro Transportation for People with Disabilities
REDUCED COST AND FREE METRO TRANSPORTATION PROGRAMS FOR PEOPLE WITH DISABILITIES Individual Day Supports are tailored services and supports that are provided to a person or a small group of no more than two (2) people, in the community. This service lends very well to the use of public transportation and associated travel training, allowing for active learning while exploring the community and its resources. While the set rate includes funding for transportation, it is important to be resourceful when possible, using available discount programs to make your funds go further. METRO TRANSIT ACCESSIBILITY CENTER The Metro Transit Accessibility Center (202)962-2700 located at Metro headquarters, 600 Fifth Street NW, Washington, DC 20001, offers the following services to people with disabilities: Information and application materials for the Reduced Fare (half fare) program for Metrobus and Metrorail Information and application materials for the MetroAccess paratransit service Consultations and functional assessments to determine eligibility for MetroAccess paratransit service Replacement ID cards for MetroAccess customers Support (by phone) for resetting your MetroAccess EZ-Pay or InstantAccess password The Transit Accessibility Center office hours are 8 a.m. to 4 p.m. weekdays, with the exception of Tuesdays with hours from 8 a.m. - 2:30 p.m. REDUCED FAIR PROGRAM Metro offers reduced fare for people with disabilities who require accessibility features to use public transportation and who have a valid Metro Disability ID. The Metro Disability ID card offers a discount of half the peak fare on Metrorail, and a reduced fare of for 90¢ cash, or 80¢ paying with a SmarTrip® card on regular Metrobus routes, and a discounted fare on other participating bus service providers. -

PATCO New Automated Fare Collection System, Smart Card Or Magnetic- Your Choice
PATCO New Automated Fare Collection System, Smart card or Magnetic- Your choice PATCO’s new fare collection system will feature the FREEDOM card, which will revolutionize how customers purchase their fares and travel on the PATCO system. The FREEDOM card is a smart card that will provide a high level of convenience and reliability to customers who use PATCO consistently. For customers who do not opt to use the FREEDOM card or who use PATCO infrequently, new magnetic tickets will be available. In PATCO’s current fare system, plastic tickets that use first generation magnetic technology are used. Although that technology was state of the art several decades ago, the technology is outdated and the tickets are prone to damage by devices commonly found in today’s environment. Unlike the current tickets, which are re-encoded numerous times for use after being captured by the fare gates, the new magnetic tickets will be paper tickets and will not be reused after capture. The new magnetic tickets can be purchased using either cash or coins. This means that customers choosing to purchase a ticket will not have to first stop at a change machine to convert their bills to coins. Both one- and two-ride tickets can be purchased from all new ticket vending machines located outside the fare gates. A customer wishing to purchase a magnetic ticket will simply select the prompt on the ticket vending machine screen for purchase of a ticket and then select the destination and whether a single ride or double ride ticket is desired. The ticket vending machine will list the price of the purchase. -

Effect of Fares on Transit Riding
Effect of Fares on Transit Riding JOHN F. CURTIN, Partner, Simpson & Curtin, Philadelphia • FARES are perhaps the most sensitive aspect of transit service-balancing uneasily between political pressures and the need for operating revenue. Political campaigns in major American cities have been won and lost over transit fare issues, and there is substantial evidence that patrons react to fare increases at the turnstiles as well as at the polls. The correlation of price increase with loss of transit riding has been well established. Most utility commissions use a variation of the "shrinkage formula" devised by our firm more than 20 years ago when pressures of inflation first became manifest in fare increase proposals by transit companies. But the corollary questions of price differential among competing transit services, and the effect of joint fares in coordinated transit operations, have not been so well explored. What is the "sub-modal split" of riding between surface and rapid transit connecting two points, when the fare is 15 cents on one and 25 cents on the other? How much added traffic is attracted to rapid transit when the feeder bus fare is dropped from 20cents to 10 cents? When feeder and trunk lines are separate operations, how should the feeder line discount in the combination fare be shared between them? These are fundamental questions of revenue and cost apportionment in developing coordination between surface and rapid transit systems. Auto travel switches freely between systems-from county roads to city streets to state highways-without motor ists' awareness; division of motor fuel revenues among these systems is accomplished by legislative standards with varying degrees of sophistication. -

Fare Policy Analysis for Public Transport: a Discrete‐Continuous Modeling Approach Using Panel Data
Fare Policy Analysis for Public Transport: A Discrete‐Continuous Modeling Approach Using Panel Data by Hazem Marwan Zureiqat B.A. in Economics Macalester College, 2006 Submitted to the Department of Civil and Environmental Engineering in Partial Fulfillment of the Requirements for the Degree of Master of Science in Transportation at the Massachusetts Institute of Technology June 2008 © 2008 Massachusetts Institute of Technology All rights reserved Signature of Author ………………………………………………………………………… Department of Civil and Environmental Engineering May 16, 2008 Certified by ……………………………………………………………………...................... Nigel H. M. Wilson Professor of Civil and Environmental Engineering Director, Master of Science in Transportation Program Thesis Supervisor Accepted by …………………………………………………………………………………. Daniele Veneziano Chairman, Departmental Committee for Graduate Students 2 Fare Policy Analysis for Public Transport: A Discrete‐Continuous Modeling Approach Using Panel Data by Hazem Marwan Zureiqat Submitted to the Department of Civil and Environmental Engineering on May 16, 2008, in partial fulfillment of the requirements for the degree of Master of Science in Transportation at the Massachusetts Institute of Technology Abstract In many large metropolitan areas, public transport is very heavily used, and ridership is approaching system capacity in the peak periods. This has caused a shift in attention by agency decision‐makers to strategies that can more effectively manage the demand for public transport, rather than simply increase overall demand. In other words, a need has arisen to understand not only why people use public transport as opposed to other modes but also how they use public transport, in terms of their ticket, mode, and time‐of‐day choices. To that end, fares become an increasingly important policy tool that can trigger certain behavioral changes among riders. -

Passenger and Vehicle Fare Information Surcharges Seattle/Bainbridge, Seattle/Bremerton, Edmonds/Kingston Fauntleroy/Vashon
19-08-0392 Printed in the USA on recycled/recyclable paper. recycled/recyclable on USA the in Printed Seattle/Bainbridge, Seattle/Bremerton, Fauntleroy/Vashon, Point Defiance/Tahlequah, Americans with Disabilities Edmonds/Kingston Southworth/Vashon Mukilteo/Clinton Act (ADA) and Title VI Notice Seattle, Washington 98121-3014 Washington Seattle, 2901 Third Avenue Suite 500 Suite Avenue Third 2901 Passenger Regular Fare 8.65 Passenger Regular Fare 5.65 Passenger Regular Fare 5.20 It is the Washington State Department of Washington State Ferries State Washington In vehicle or walk on Senior/Disability/Medicare Card Fare 4.30 In vehicle or walk on Senior/Disability/Medicare Card Fare 2.80 In vehicle or walk on Senior/Disability/Medicare Card Fare 2.60 Transportation’s policy to ensure that no Youth Fare 4.30 Youth Fare 2.80 Youth Fare 2.60 person shall, on the grounds of race, color, national origin, or sex, as provided by Title VI Wave2Go Multi-Ride Card 69.70 Wave2Go Multi-Ride Card 45.70 Wave2Go Multi-Ride Card 42.10 of the Civil Rights Act of 1964, or based on Monthly Ferry Pass 111.55 Monthly Ferry Pass 73.15 Monthly Ferry Pass 67.40 disability as provided by the Americans with Bicycle Surcharge Passenger Fare Plus 1.00 Bicycle Surcharge Passenger Fare Plus 1.00 Bicycle Surcharge Passenger Fare Plus 1.00 Disabilities Act, be excluded from participation in, be denied the benefits of, or be otherwise Small Vehicle & Driver Regular Fare 12.35 Peak Season 16.00 Small Vehicle & Driver Regular Fare 15.75 Peak Season 20.40 Small Vehicle & Driver Regular Fare 7.40 Peak Season 9.70 discriminated against under any of its federally @WSFerries funded programs and activities. -

Accessible Transportation Options for People with Disabilities and Senior Citizens
Accessible Transportation Options for People with Disabilities and Senior Citizens In the Washington, D.C. Metropolitan Area JANUARY 2017 Transfer Station Station Features Red Line • Glenmont / Shady Grove Bus to Airport System Orange Line • New Carrollton / Vienna Parking Station Legend Blue Line • Franconia-Springfield / Largo Town Center in Service Map Hospital Under Construction Green Line • Branch Ave / Greenbelt Airport Full-Time Service wmata.com Yellow Line • Huntington / Fort Totten Customer Information Service: 202-637-7000 Connecting Rail Systems Rush-Only Service: Monday-Friday Silver Line • Wiehle-Reston East / Largo Town Center TTY Phone: 202-962-2033 6:30am - 9:00am 3:30pm - 6:00pm Metro Transit Police: 202-962-2121 Glenmont Wheaton Montgomery Co Prince George’s Co Shady Grove Forest Glen Rockville Silver Spring Twinbrook B30 to Greenbelt BWI White Flint Montgomery Co District of Columbia College Park-U of Md Grosvenor - Strathmore Georgia Ave-Petworth Takoma Prince George’s Plaza Medical Center West Hyattsville Bethesda Fort Totten Friendship Heights Tenleytown-AU Prince George’s Co Van Ness-UDC District of Columbia Cleveland Park Columbia Heights Woodley Park Zoo/Adams Morgan U St Brookland-CUA African-Amer Civil Dupont Circle War Mem’l/Cardozo Farragut North Shaw-Howard U Rhode Island Ave Brentwood Wiehle-Reston East Spring Hill McPherson Mt Vernon Sq NoMa-Gallaudet U New Carrollton Sq 7th St-Convention Center Greensboro Fairfax Co Landover Arlington Co Tysons Corner Gallery Place Union Station Chinatown Cheverly 5A to -

First-Year Impact of Reduced Transit Fares on Southern California Rapid Transit District
Transportation Research Record 992 61 First-Year Impact of Reduced Transit Fares on Southern California Rapid Transit District SUSAN PHIFER ABSTRACT percent allocation of the sales tax funds to cities is permanent. For the first 3 years--July 1, 1982, through June In 1980 voters in Los Angeles County passed 30, 1985--the first claim on the balance of the a referendum designed to support public funds is for fare reductions. The district's base transit development through a dedicated fare was reduced from 85 to 50 cents with concurrent sales tax. One feature of this referendum, reductions in the balance of the district's fare the reduced-fare program, substantially structure. Funds are provided for the additional lowered the bus fares at the Southern Cali service necessary to relieve overcrowding from fornia Rapid Transit District (SCRTO) and increased ridership induced by the lower fare. Funds provided a subsidy to maintain adequate will also be allocat.ed to the municipal bus oper service levels. The lower fares precipitated ators as necessary, to keep their ba·se fare at the a surge in patronage on SCRTD lines. This SO-cent level. During the first 3 years, funds not growth in system boardings made it necessary required for the fare-reduction program are avail to accelerate monitoring of the bus lines able for rapid transit development programs. and to increase service levels in many The fare-reduction program of Proposition A ends cases. The attempts made by SCRTD to deal in July 1985. At that time funds w-111 be reallocated with the patronage growth and the impacts on as follows: 25 percent for the cities, a minimum of patronage, service levels, and operating 35 percent for transit guideway development (Metro productivity are described.