Performance Standards for Antimicrobial Susceptibility Testing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Overcoming Fluoroquinolone Resistance: Mechanistic Basis of Non- Quinolone Antibacterials Targeting Type Ii Topoisomerases
OVERCOMING FLUOROQUINOLONE RESISTANCE: MECHANISTIC BASIS OF NON- QUINOLONE ANTIBACTERIALS TARGETING TYPE II TOPOISOMERASES By Elizabeth Grace Gibson Dissertation Submitted to the Faculty of the Graduate School of Vanderbilt University in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY in Pharmacology May 10, 2019 Nashville, Tennessee Approved: Neil Osheroff, Ph.D. Joey Barnett, Ph.D. Wendell S. Akers, Pharm.D., Ph.D. Sean Davies, Ph.D. Benjamin Spiller, Ph.D. Timothy R. Sterling, M.D. DEDICATION To all my family and church family who have supported and encouraged me over all my years in school. To Him who I put all my trust. Commit your way to the Lord, trust also in Him and He shall bring it to pass. Psalm 37:5 ii ACKNOWLEDGEMENTS I want to first thank my Ph.D. advisor, Dr. Neil Osheroff, for allowing me to work in his laboratory. Thank you for all your support and encouragement and just being an overall great mentor. You really know how to bring us up when we need it or give us an ego check when we get a little high and mighty when things are going well. I appreciate your supportiveness to careers outside academia. I also appreciate that you always have our best interest at heart. To Dr. Joe Deweese, my first research mentor and the one who instilled the love of topoisomerase research. Without your guidance I would not be where I am today. Thank you for introducing me to Neil and his laboratory and helping with the transition from research in your lab to his. -

)&F1y3x PHARMACEUTICAL APPENDIX to THE
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ACTODIGIN 36983-69-4 ABANOQUIL 90402-40-7 ADAFENOXATE 82168-26-1 ABCIXIMAB 143653-53-6 ADAMEXINE 54785-02-3 ABECARNIL 111841-85-1 ADAPALENE 106685-40-9 ABITESARTAN 137882-98-5 ADAPROLOL 101479-70-3 ABLUKAST 96566-25-5 ADATANSERIN 127266-56-2 ABUNIDAZOLE 91017-58-2 ADEFOVIR 106941-25-7 ACADESINE 2627-69-2 ADELMIDROL 1675-66-7 ACAMPROSATE 77337-76-9 ADEMETIONINE 17176-17-9 ACAPRAZINE 55485-20-6 ADENOSINE PHOSPHATE 61-19-8 ACARBOSE 56180-94-0 ADIBENDAN 100510-33-6 ACEBROCHOL 514-50-1 ADICILLIN 525-94-0 ACEBURIC ACID 26976-72-7 ADIMOLOL 78459-19-5 ACEBUTOLOL 37517-30-9 ADINAZOLAM 37115-32-5 ACECAINIDE 32795-44-1 ADIPHENINE 64-95-9 ACECARBROMAL 77-66-7 ADIPIODONE 606-17-7 ACECLIDINE 827-61-2 ADITEREN 56066-19-4 ACECLOFENAC 89796-99-6 ADITOPRIM 56066-63-8 ACEDAPSONE 77-46-3 ADOSOPINE 88124-26-9 ACEDIASULFONE SODIUM 127-60-6 ADOZELESIN 110314-48-2 ACEDOBEN 556-08-1 ADRAFINIL 63547-13-7 ACEFLURANOL 80595-73-9 ADRENALONE -

Gonorrhea, Chlamydia, and Syphilis
2019 GONORRHEA, CHLAMYDIA, AND SYPHILIS AND CHLAMYDIA, GONORRHEA, Dedication TAG would like to thank the National Coalition of STD Directors for funding and input on the report. THE PIPELINE REPORT Pipeline for Gonorrhea, Chlamydia, and Syphilis By Jeremiah Johnson Introduction The current toolbox for addressing gonorrhea, chlamydia, and syphilis is inadequate. At a time where all three epidemics are dramatically expanding in locations all around the globe, including record-breaking rates of new infections in the United States, stakeholders must make do with old tools, inadequate systems for addressing sexual health, and a sparse research pipeline of new treatment, prevention, and diagnostic options. Lack of investment in sexual health research has left the field with inadequate prevention options, and limited access to infrastructure for testing and treatment have allowed sexually transmitted infections (STIs) to flourish. The consequences of this underinvestment are large: according to the World Health Organization (WHO), in 2012 there were an estimated 357 million new infections (roughly 1 million per day) of the four curable STIs: gonorrhea, chlamydia, syphilis, and trichomoniasis.1 In the United States, the three reportable STIs that are the focus of this report—gonorrhea, chlamydia, and syphilis—are growing at record paces. In 2017, a total of 30,644 cases of primary and secondary (P&S) syphilis—the most infectious stages of the disease—were reported in the United States. Since reaching a historic low in 2000 and 2001, the rate of P&S syphilis has increased almost every year, increasing 10.5% during 2016–2017. Also in 2017, 555,608 cases of gonorrhea were reported to the U.S. -

Novel Β-Lactamase Inhibitors: a Therapeutic Hope Against the Scourge of Multidrug Resistance
REVIEW ARTICLE published: 24 December 2013 doi: 10.3389/fmicb.2013.00392 Novel β-lactamase inhibitors: a therapeutic hope against the scourge of multidrug resistance Richard R. Watkins1,2 *, Krisztina M. Papp-Wallace 3,4 , Sarah M. Drawz 5 and Robert A. Bonomo3,4,6,7 * 1 Department of Internal Medicine, Northeast Ohio Medical University, Rootstown, OH, USA 2 Division of Infectious Diseases, Akron General Medical Center, Akron, OH, USA 3 Research Service, Louis Stokes Cleveland Department of Veterans Affairs Medical Center, Cleveland, OH, USA 4 Department of Medicine, Case Western Reserve University, Cleveland, OH, USA 5 Department of Lab Medicine and Pathology, University of Minnesota, Minneapolis, MN, USA 6 Pharmacology, Case Western Reserve University, Cleveland, OH, USA 7 Molecular Biology and Microbiology, Case Western Reserve University, Cleveland, OH, USA Edited by: The increasing incidence and prevalence of multi-drug resistance (MDR) among contem- Marcelo Tolmasky, California State porary Gram-negative bacteria represents a significant threat to human health. Since University Fullerton, USA their discovery, β-lactam antibiotics have been a major component of the armamentarium Reviewed by: against these serious pathogens. Unfortunately, a wide range of β-lactamase enzymes have Marcelo Tolmasky, California State University Fullerton, USA emerged that are capable of inactivating these powerful drugs. In the past 30 years, a major Gabriel Gutkind, Universidad de advancement in the battle against microbes has been the development of β-lactamase Buenos Aires, Argentina inhibitors, which restore the efficacy of β-lactam antibiotics (e.g., ampicillin/sulbactam, *Correspondence: amoxicillin/clavulanate, ticarcillin/clavulanate, and piperacillin/tazobactam). Unfortunately, Richard R. Watkins, Division of many newly discovered β-lactamases are not inactivated by currently available inhibitors. -

Consideration of Antibacterial Medicines As Part Of
Consideration of antibacterial medicines as part of the revisions to 2019 WHO Model List of Essential Medicines for adults (EML) and Model List of Essential Medicines for children (EMLc) Section 6.2 Antibacterials including Access, Watch and Reserve Lists of antibiotics This summary has been prepared by the Health Technologies and Pharmaceuticals (HTP) programme at the WHO Regional Office for Europe. It is intended to communicate changes to the 2019 WHO Model List of Essential Medicines for adults (EML) and Model List of Essential Medicines for children (EMLc) to national counterparts involved in the evidence-based selection of medicines for inclusion in national essential medicines lists (NEMLs), lists of medicines for inclusion in reimbursement programs, and medicine formularies for use in primary, secondary and tertiary care. This document does not replace the full report of the WHO Expert Committee on Selection and Use of Essential Medicines (see The selection and use of essential medicines: report of the WHO Expert Committee on Selection and Use of Essential Medicines, 2019 (including the 21st WHO Model List of Essential Medicines and the 7th WHO Model List of Essential Medicines for Children). Geneva: World Health Organization; 2019 (WHO Technical Report Series, No. 1021). Licence: CC BY-NC-SA 3.0 IGO: https://apps.who.int/iris/bitstream/handle/10665/330668/9789241210300-eng.pdf?ua=1) and Corrigenda (March 2020) – TRS1021 (https://www.who.int/medicines/publications/essentialmedicines/TRS1021_corrigenda_March2020. pdf?ua=1). Executive summary of the report: https://apps.who.int/iris/bitstream/handle/10665/325773/WHO- MVP-EMP-IAU-2019.05-eng.pdf?ua=1. -

WO 2010/025328 Al
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date 4 March 2010 (04.03.2010) WO 2010/025328 Al (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/00 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, (21) International Application Number: CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, PCT/US2009/055306 DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, 28 August 2009 (28.08.2009) KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, (25) Filing Language: English NO, NZ, OM, PE, PG, PH, PL, PT, RO, RS, RU, SC, SD, (26) Publication Language: English SE, SG, SK, SL, SM, ST, SV, SY, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (30) Priority Data: 61/092,497 28 August 2008 (28.08.2008) US (84) Designated States (unless otherwise indicated, for every kind of regional protection available): ARIPO (BW, GH, (71) Applicant (for all designated States except US): FOR¬ GM, KE, LS, MW, MZ, NA, SD, SL, SZ, TZ, UG, ZM, EST LABORATORIES HOLDINGS LIMITED [IE/ ZW), Eurasian (AM, AZ, BY, KG, KZ, MD, RU, TJ, —]; 18 Parliament Street, Milner House, Hamilton, TM), European (AT, BE, BG, CH, CY, CZ, DE, DK, EE, Bermuda HM12 (BM). -

Computational Antibiotics Book
Andrew V DeLong, Jared C Harris, Brittany S Larcart, Chandler B Massey, Chelsie D Northcutt, Somuayiro N Nwokike, Oscar A Otieno, Harsh M Patel, Mehulkumar P Patel, Pratik Pravin Patel, Eugene I Rowell, Brandon M Rush, Marc-Edwin G Saint-Louis, Amy M Vardeman, Felicia N Woods, Giso Abadi, Thomas J. Manning Computational Antibiotics Valdosta State University is located in South Georgia. Computational Antibiotics Index • Computational Details and Website Access (p. 8) • Acknowledgements (p. 9) • Dedications (p. 11) • Antibiotic Historical Introduction (p. 13) Introduction to Antibiotic groups • Penicillin’s (p. 21) • Carbapenems (p. 22) • Oxazolidines (p. 23) • Rifamycin (p. 24) • Lincosamides (p. 25) • Quinolones (p. 26) • Polypeptides antibiotics (p. 27) • Glycopeptide Antibiotics (p. 28) • Sulfonamides (p. 29) • Lipoglycopeptides (p. 30) • First Generation Cephalosporins (p. 31) • Cephalosporin Third Generation (p. 32) • Fourth-Generation Cephalosporins (p. 33) • Fifth Generation Cephalosporin’s (p. 34) • Tetracycline antibiotics (p. 35) Computational Antibiotics Antibiotics Covered (in alphabetical order) Amikacin (p. 36) Cefempidone (p. 98) Ceftizoxime (p. 159) Amoxicillin (p. 38) Cefepime (p. 100) Ceftobiprole (p. 161) Ampicillin (p. 40) Cefetamet (p. 102) Ceftoxide (p. 163) Arsphenamine (p. 42) Cefetrizole (p. 104) Ceftriaxone (p. 165) Azithromycin (p.44) Cefivitril (p. 106) Cefuracetime (p. 167) Aziocillin (p. 46) Cefixime (p. 108) Cefuroxime (p. 169) Aztreonam (p.48) Cefmatilen ( p. 110) Cefuzonam (p. 171) Bacampicillin (p. 50) Cefmetazole (p. 112) Cefalexin (p. 173) Bacitracin (p. 52) Cefodizime (p. 114) Chloramphenicol (p.175) Balofloxacin (p. 54) Cefonicid (p. 116) Cilastatin (p. 177) Carbenicillin (p. 56) Cefoperazone (p. 118) Ciprofloxacin (p. 179) Cefacetrile (p. 58) Cefoselis (p. 120) Clarithromycin (p. 181) Cefaclor (p. -

Dissertation Submitted in Partial Fulfillment of the Regulations
IDENTIFICATION OF GENES CODING FOR CARBAPENEMASES IN CLINICAL ISOLATES OF CARBAPENEM RESISTANT KLEBSIELLA SPECIES IN A TERTIARY CARE HOSPITAL Dissertation submitted in Partial fulfillment of the Regulations required for the award of M.D. DEGREE In MICROBIOLOGY– BRANCH IV The Tamil Nadu DR. M.G.R. MEDICAL UNIVERSITY Chennai MAY 2020. UNIVERSITY REGISTRATION NO: 201714252 CERTIFICATE This is to certify that the enclosed work “Identification of Genes Coding for Carbapenemases in Clinical Isolates of Carbapenem Resistant Klebsiella Species in a Tertiary Care Hospital” submitted by Dr.S.Sharon Dorothy to The Tamilnadu Dr. MGR Medical University is based on bonafide cases studied and analysed by the candidate in the Department of Microbiology, Coimbatore Medical College Hospital during the period from July 2018 to June 2019 under the guidance and supervision of Dr. N.Mythily, MD., Professor & HOD, Department of Microbiology and the conclusion reached in this study are her own. Guide Dr. N.MYTHILY, MD., Professor & HOD, Department of Microbiology, Coimbatore Medical College, Coimbatore. Dr. B. ASOKAN. M.S., M.Ch., Dr., N.MYTHILY, MD., Dean, Professor & HOD, Coimbatore Medical College and Hospital, Department of Microbiology, Coimbatore – 14. Coimbatore Medical College, Coimbatore – 14. DECLARATION I, Dr.S.Sharon Dorothy solemnly declare that the dissertation entitled “Identification of Genes Coding for Carbapenemases in Clinical Isolates of Carbapenem Resistant Klebsiella Species in a Tertiary Care Hospital” was done by me at Coimbatore Medical College Hospital, during the period from July 2018 to June 2019 under the guidance and supervision of Dr. N. Mythily, M.D., Professor & HOD, Department of Microbiology, Coimbatore Medical College, Coimbatore. -

Anew Drug Design Strategy in the Liht of Molecular Hybridization Concept
www.ijcrt.org © 2020 IJCRT | Volume 8, Issue 12 December 2020 | ISSN: 2320-2882 “Drug Design strategy and chemical process maximization in the light of Molecular Hybridization Concept.” Subhasis Basu, Ph D Registration No: VB 1198 of 2018-2019. Department Of Chemistry, Visva-Bharati University A Draft Thesis is submitted for the partial fulfilment of PhD in Chemistry Thesis/Degree proceeding. DECLARATION I Certify that a. The Work contained in this thesis is original and has been done by me under the guidance of my supervisor. b. The work has not been submitted to any other Institute for any degree or diploma. c. I have followed the guidelines provided by the Institute in preparing the thesis. d. I have conformed to the norms and guidelines given in the Ethical Code of Conduct of the Institute. e. Whenever I have used materials (data, theoretical analysis, figures and text) from other sources, I have given due credit to them by citing them in the text of the thesis and giving their details in the references. Further, I have taken permission from the copyright owners of the sources, whenever necessary. IJCRT2012039 International Journal of Creative Research Thoughts (IJCRT) www.ijcrt.org 284 www.ijcrt.org © 2020 IJCRT | Volume 8, Issue 12 December 2020 | ISSN: 2320-2882 f. Whenever I have quoted written materials from other sources I have put them under quotation marks and given due credit to the sources by citing them and giving required details in the references. (Subhasis Basu) ACKNOWLEDGEMENT This preface is to extend an appreciation to all those individuals who with their generous co- operation guided us in every aspect to make this design and drawing successful. -

The Study Listed May Include Approved and Non-Approved Uses, Formulations Or Treatment Regimens
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product. Before prescribing any product mentioned in this Register, healthcare professionals should consult prescribing information for the product approved in their country. GSK Medicine: Gepotidacin Study Number: 207625 Title: Meta-analysis to estimate the microbiological treatment effect of nitrofurantoin for determination of the non-inferiority margin in a phase 3 clinical trial of uncomplicated urinary tract infection (uUTI). Rationale: Active-comparator, non-inferiority study designs are generally used in uUTI trials, given the ethical implications of placebo treatment. In order to design, execute, and analyze a non-inferiority trial, an estimate of the treatment effect (M1) of the planned active comparator (nitrofurantoin), must be obtained from historical randomized or open label studies. Once an estimate of M1 (nitrofurantoin treatment effect) is obtained, a non-inferiority margin (M2) or the largest clinically acceptable difference of the test drug compared to the active comparator must be determined. Determination of M1 and M2 is critical to the design, analysis and interpretation of a non-inferiority trial. The rationale for this study was to estimate the treatment effect of an active comparator (nitrofurantoin) in order to determine the non-inferiority margin for a Phase III study, which will demonstrate the efficacy of a new -

European Surveillance of Healthcare-Associated Infections in Intensive Care Units
TECHNICAL DOCUMENT European surveillance of healthcare-associated infections in intensive care units HAI-Net ICU protocol Protocol version 1.02 www.ecdc.europa.eu ECDC TECHNICAL DOCUMENT European surveillance of healthcare- associated infections in intensive care units HAI-Net ICU protocol, version 1.02 This technical document of the European Centre for Disease Prevention and Control (ECDC) was coordinated by Carl Suetens. In accordance with the Staff Regulations for Officials and Conditions of Employment of Other Servants of the European Union and the ECDC Independence Policy, ECDC staff members shall not, in the performance of their duties, deal with a matter in which, directly or indirectly, they have any personal interest such as to impair their independence. This is version 1.02 of the HAI-Net ICU protocol. Differences between versions 1.01 (December 2010) and 1.02 are purely editorial. Suggested citation: European Centre for Disease Prevention and Control. European surveillance of healthcare- associated infections in intensive care units – HAI-Net ICU protocol, version 1.02. Stockholm: ECDC; 2015. Stockholm, March 2015 ISBN 978-92-9193-627-4 doi 10.2900/371526 Catalogue number TQ-04-15-186-EN-N © European Centre for Disease Prevention and Control, 2015 Reproduction is authorised, provided the source is acknowledged. TECHNICAL DOCUMENT HAI-Net ICU protocol, version 1.02 Table of contents Abbreviations ............................................................................................................................................... -
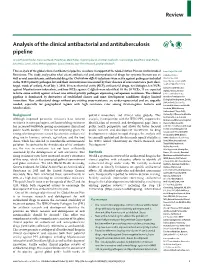
Analysis of the Clinical Antibacterial and Antituberculosis Pipeline
Review Analysis of the clinical antibacterial and antituberculosis pipeline Ursula Theuretzbacher, Simon Gottwalt, Peter Beyer, Mark Butler, Lloyd Czaplewski, Christian Lienhardt, Lorenzo Moja, Mical Paul, Sarah Paulin, John H Rex, Lynn L Silver, Melvin Spigelman, Guy E Thwaites, Jean-Pierre Paccaud, Stephan Harbarth This analysis of the global clinical antibacterial pipeline was done in support of the Global Action Plan on Antimicrobial Lancet Infect Dis 2018 Resistance. The study analysed to what extent antibacterial and antimycobacterial drugs for systemic human use as Published Online well as oral non-systemic antibacterial drugs for Clostridium difficile infections were active against pathogens included October 15, 2018 in the WHO priority pathogen list and their innovativeness measured by their absence of cross-resistance (new class, http://dx.doi.org/10.1016/ S1473-3099(18)30513-9 target, mode of action). As of July 1, 2018, 30 new chemical entity (NCE) antibacterial drugs, ten biologics, ten NCEs Center for Anti-Infective against Mycobacterium tuberculosis, and four NCEs against C difficile were identified. Of the 30 NCEs, 11 are expected Agents, Vienna, Austria to have some activity against at least one critical priority pathogen expressing carbapenem resistance. The clinical (U Theuretzbacher PhD); pipeline is dominated by derivatives of established classes and most development candidates display limited Biovision Foundation for innovation. New antibacterial drugs without pre-existing cross-resistance are under-represented and are urgently Ecological Development, Zurich, Switzerland (S Gottwalt); needed, especially for geographical regions with high resistance rates among Gram-negative bacteria and Essential Medicines and Health M tuberculosis. Products, WHO, Geneva, Switzerland (P Beyer PhD); Background potential inno vation, and clinical value globally.