File Download
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Non-Invasive Surveillance for Plasmodium in Reservoir Macaque
Siregar et al. Malar J (2015) 14:404 DOI 10.1186/s12936-015-0857-2 METHODOLOGY Open Access Non‑invasive surveillance for Plasmodium in reservoir macaque species Josephine E. Siregar1, Christina L. Faust2*, Lydia S. Murdiyarso1, Lis Rosmanah3, Uus Saepuloh3, Andrew P. Dobson2 and Diah Iskandriati3 Abstract Background: Primates are important reservoirs for human diseases, but their infection status and disease dynamics are difficult to track in the wild. Within the last decade, a macaque malaria, Plasmodium knowlesi, has caused disease in hundreds of humans in Southeast Asia. In order to track cases and understand zoonotic risk, it is imperative to be able to quantify infection status in reservoir macaque species. In this study, protocols for the collection of non-invasive samples and isolation of malaria parasites from naturally infected macaques are optimized. Methods: Paired faecal and blood samples from 60 Macaca fascicularis and four Macaca nemestrina were collected. All animals came from Sumatra or Java and were housed in semi-captive breeding colonies around West Java. DNA was extracted from samples using a modified protocol. Nested polymerase chain reactions (PCR) were run to detect Plasmodium using primers targeting mitochondrial DNA. Sensitivity of screening faecal samples for Plasmodium was compared to other studies using Kruskal Wallis tests and logistic regression models. Results: The best primer set was 96.7 % (95 % confidence intervals (CI): 83.3–99.4 %) sensitive for detecting Plasmo- dium in faecal samples of naturally infected macaques (n 30). This is the first study to produce definitive estimates of Plasmodium sensitivity and specificity in faecal samples= from naturally infected hosts. -

Plasmodium Vivax in Vitro Continuous Culture: the Spoke in the Wheel
Bermúdez et al. Malar J (2018) 17:301 https://doi.org/10.1186/s12936-018-2456-5 Malaria Journal REVIEW Open Access Plasmodium vivax in vitro continuous culture: the spoke in the wheel Maritza Bermúdez1, Darwin Andrés Moreno‑Pérez2,3, Gabriela Arévalo‑Pinzón1, Hernando Curtidor1,4 and Manuel Alfonso Patarroyo2,4* Abstract Understanding the life cycle of Plasmodium vivax is fundamental for developing strategies aimed at controlling and eliminating this parasitic species. Although advances in omic sciences and high-throughput techniques in recent years have enabled the identifcation and characterization of proteins which might be participating in P. vivax inva‑ sion of target cells, exclusive parasite tropism for invading reticulocytes has become the main obstacle in maintaining a continuous culture for this species. Such advance that would help in defning each parasite protein’s function in the complex process of P. vivax invasion, in addition to evaluating new therapeutic agents, is still a dream. Advances related to maintenance, culture medium supplements and the use of diferent sources of reticulocytes and parasites (strains and isolates) have been made regarding the development of an in vitro culture for P. vivax; however, only some cultures having few replication cycles have been obtained to date, meaning that this parasite’s maintenance goes beyond the technical components involved. Although it is still not yet clear which molecular mechanisms P. vivax prefers for invading young CD71+ reticulocytes [early maturation stages (I–II–III)], changes related to mem‑ brane proteins remodelling of such cells could form part of the explanation. The most relevant aspects regarding P. vivax in vitro culture and host cell characteristics have been analysed in this review to explain possible reasons why the species’ continuous in vitro culture is so difcult to standardize. -

Quantifying the Removal of Red Blood Cells in Macaca Mulatta During a Plasmodium Coatneyi Infection Luis L
Fonseca et al. Malar J (2016) 15:410 DOI 10.1186/s12936-016-1465-5 Malaria Journal RESEARCH Open Access Quantifying the removal of red blood cells in Macaca mulatta during a Plasmodium coatneyi infection Luis L. Fonseca1,4*, Harnel S. Alezi1, Alberto Moreno2,4, John W. Barnwell3,4, Mary R. Galinski2,4 and Eberhard O. Voit1,4 Abstract Background: Malaria is the most deadly parasitic disease in humans globally, and the long-time coexistence with malaria has left indelible marks in the human genome that are the causes of a variety of genetic disorders. Although anaemia is a common clinical complication of malaria, the root causes and mechanisms involved in the pathogenesis of malarial anaemia are unclear and difficult to study in humans. Non-human primate (NHP) model systems enable the mechanistic study and quantification of underlying causative factors of malarial anaemia, and particularly the onset of severe anaemia. Methods: Data were obtained in the course of Plasmodium coatneyi infections of malaria-naïve and semi-immune rhesus macaques (Macaca mulatta), whose red blood cells (RBCs) were labelled in situ with biotin at the time the infections were initiated. The data were used for a survival analysis that permitted, for the first time, an accurate esti- mation of the lifespan of erythrocytes in macaques. The data furthermore formed the basis for the development and parameterization of a recursive dynamic model of erythrocyte turnover, which was used for the quantification of RBC production and removal in each macaque. Results: The computational analysis demonstrated that the lifespan of erythrocytes in macaques is 98 21 days. -

Malaria Treatment in Africa
Malaria Treatment in Africa Africa Fighting Malaria Policy Paper May 2008 By Richard Tren, Philip Coticelli, Roger Bate and Kimberly Hess AFRICA FIGHTING MALARIA 1050 17th Street, NW P.O Box 17156 Suite 520 Congella Washington DC, 20036 4013 United States South Africa www.fightingmalaria.org Table of Contents I. Executive Summary.................................................................................................................3 II. Key Recommendations...........................................................................................................5 III. Introduction: Advocates Drive Reform..................................................................................6 IV. Private Sector Regulation......................................................................................................8 V. Public Funding for Drugs: Quantity vs. Quality....................................................................11 VI. Generic and Local Pharmaceutical Production.....................................................................15 VII. The Affordable Medicines Facility- malaria (AMFm) ........................................................19 VIII. What Africa Still Lacks: Functioning Health Systems.......................................................22 IX. Conclusion..........................................................................................................................25 X. Endnotes ..............................................................................................................................26 -
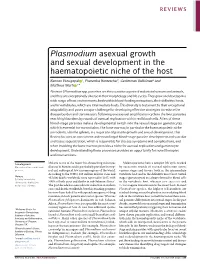
Plasmodium Asexual Growth and Sexual Development in the Haematopoietic Niche of the Host
REVIEWS Plasmodium asexual growth and sexual development in the haematopoietic niche of the host Kannan Venugopal 1, Franziska Hentzschel1, Gediminas Valkiūnas2 and Matthias Marti 1* Abstract | Plasmodium spp. parasites are the causative agents of malaria in humans and animals, and they are exceptionally diverse in their morphology and life cycles. They grow and develop in a wide range of host environments, both within blood- feeding mosquitoes, their definitive hosts, and in vertebrates, which are intermediate hosts. This diversity is testament to their exceptional adaptability and poses a major challenge for developing effective strategies to reduce the disease burden and transmission. Following one asexual amplification cycle in the liver, parasites reach high burdens by rounds of asexual replication within red blood cells. A few of these blood- stage parasites make a developmental switch into the sexual stage (or gametocyte), which is essential for transmission. The bone marrow, in particular the haematopoietic niche (in rodents, also the spleen), is a major site of parasite growth and sexual development. This Review focuses on our current understanding of blood-stage parasite development and vascular and tissue sequestration, which is responsible for disease symptoms and complications, and when involving the bone marrow, provides a niche for asexual replication and gametocyte development. Understanding these processes provides an opportunity for novel therapies and interventions. Gametogenesis Malaria is one of the major life- threatening infectious Malaria parasites have a complex life cycle marked Maturation of male and female diseases in humans and is particularly prevalent in trop- by successive rounds of asexual replication across gametes. ical and subtropical low- income regions of the world. -

Phylogenetic Analysis of Simian Plasmodium Spp. Infecting Anopheles Balabacensis Baisas in Sabah, Malaysia
RESEARCH ARTICLE Phylogenetic analysis of simian Plasmodium spp. infecting Anopheles balabacensis Baisas in Sabah, Malaysia Tock H. Chua1*, Benny O. Manin1, Sylvia Daim1, Indra Vythilingam2, Chris Drakeley3 1 Department of Pathobiology and Medical Diagnostics, Faculty of Medicine and Health Sciences, Universiti Malaysia Sabah, Kota Kinabalu, Sabah, Malaysia, 2 Department of Parasitology, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia, 3 Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom a1111111111 a1111111111 * [email protected], [email protected] a1111111111 a1111111111 a1111111111 Abstract Background OPEN ACCESS Anopheles balabacensis of the Leucospyrus group has been confirmed as the primary Citation: Chua TH, Manin BO, Daim S, Vythilingam knowlesi malaria vector in Sabah, Malaysian Borneo for some time now. Presently, knowlesi I, Drakeley C (2017) Phylogenetic analysis of malaria is the only zoonotic simian malaria in Malaysia with a high prevalence recorded in simian Plasmodium spp. infecting Anopheles the states of Sabah and Sarawak. balabacensis Baisas in Sabah, Malaysia. PLoS Negl Trop Dis 11(10): e0005991. https://doi.org/ 10.1371/journal.pntd.0005991 Methodology/Principal findings Editor: Hans-Peter Fuehrer, Vienna, AUSTRIA Anopheles spp. were sampled using human landing catch (HLC) method at Paradason vil- lage in Kudat district of Sabah. The collected Anopheles were identified morphologically and Received: June 30, 2017 then subjected to total DNA extraction and polymerase chain reaction (PCR) to detect Plas- Accepted: September 24, 2017 modium parasites in the mosquitoes. Identification of Plasmodium spp. was confirmed by Published: October 2, 2017 sequencing the SSU rRNA gene with species specific primers. -

Plasmodium Knowlesi: a Superb in Vivo Nonhuman Primate Model of Antigenic Variation in Malaria
SPECIAL ISSUE REVIEW 85 Plasmodium knowlesi: a superb in vivo nonhuman primate model of antigenic variation in malaria M. R. GALINSKI1,2*,S.A.LAPP1, M. S. PETERSON1,F.AY3,C.J.JOYNER1, K. G. LE ROCH4,L.L.FONSECA5,E.O.VOIT5 and THE MAHPIC CONSORTIUM6 1 Emory Vaccine Center, Yerkes National Primate Research Center, Emory University, Atlanta, GA, USA 2 Division of Infectious Diseases, Department of Medicine, Emory University, Atlanta, GA, USA 3 La Jolla Institute for Allergy and Immunology, La Jolla, CA 92037, USA 4 Department of Cell Biology & Neuroscience, Center for Disease and Vector Research, Institute for Integrative Genome Biology, University of California Riverside, CA 92521, USA 5 The Wallace H. Coulter Department of Biomedical Engineering, Georgia Institute of Technology and Emory University, Atlanta, Georgia, 30332-2000, USA 6 Malaria Host–Pathogen Interaction Center, www.systemsbiology.emory.edu (Received 7 April 2017; revised 3 June 2017; accepted 6 June 2017; first published online 17 July 2017) SUMMARY Antigenic variation in malaria was discovered in Plasmodium knowlesi studies involving longitudinal infections of rhesus macaques (M. mulatta). The variant proteins, known as the P. knowlesi Schizont Infected Cell Agglutination (SICA) anti- gens and the P. falciparum Erythrocyte Membrane Protein 1 (PfEMP1) antigens, expressed by the SICAvar and var mul- tigene families, respectively, have been studied for over 30 years. Expression of the SICA antigens in P. knowlesi requires a splenic component, and specific antibodies are necessary for variant antigen switch events in vivo. Outstanding questions revolve around the role of the spleen and the mechanisms by which the expression of these variant antigen families are regulated. -
Structural and Functional Insights Into Apicomplexan Gliding and Its Regulation
Structural and functional insights into apicomplexan gliding and its regulation Dissertation to obtain the degree of Doctor of Natural Sciences University of Hamburg Faculty of Mathematics, Informatics and Natural Sciences at the Department of Biology by Samuel Pažický from Bratislava, Slovakia Hamburg 2020 Examination commission Examination commission chair Prof. Dr. Jörg Ganzhorn (University of Hamburg) Examination commission members Prof. Jonas Schmidt-Chanasit (Bernhard Nocht Institute for Tropical Medicine and University of Hamburg) Prof. Tim Gilberger (Bernhard Nocht Institute for Tropical Medicine, Centre for Structural Systems Biology and University of Hamburg) Dr. Maria Garcia-Alai (European Molecular Biology Laboratory and Centre for Structural Systems Biology) Dr. Christian Löw (European Molecular Biology Laboratory and Centre for Structural Systems Biology) Date of defence: 29.01.2021 This work was performed at European Molecular Biology Laboratory, Hamburg Unit under the supervision of Dr. Christian Löw and Prof. Tim-Wolf Gilberger. The work was supported by the Joachim Herz Foundation. Evaluation Prof. Dr. rer. nat. Tim-Wolf Gilberger Bernhard Nocht Institute for Tropical Medicine (BNITM) Department of Cellular Parasitology Hamburg Dr. Christian Löw European Molecular Biology Laboratory Hamburg unit Hamburg Prof. Dr. vet. med. Thomas Krey Hannover Medical School Institute of Virology Declaration of academic honesty I hereby declare, on oath, that I have written the present dissertation by my own and have not used other than the acknowledged resources and aids. Eidesstattliche Erklärung Hiermit erkläre ich an Eides statt, dass ich die vorliegende Dissertationsschrift selbst verfasst und keine anderen als die angegebenen Quellen und Hilfsmittel benutzt habe. Hamburg, 22.9.2020 Samuel Pažický List of contents Declaration of academic honesty 4 List of contents 5 Acknowledgements 6 Summary 7 Zusammenfassung 10 List of publications 12 Scientific contribution to the manuscript 14 Abbreviations 16 1. -

Genetic Diversity of Circumsporozoite Protein In
Chong et al. Malar J (2020) 19:377 https://doi.org/10.1186/s12936-020-03451-x Malaria Journal RESEARCH Open Access Genetic diversity of circumsporozoite protein in Plasmodium knowlesi isolates from Malaysian Borneo and Peninsular Malaysia Eric Tzyy Jiann Chong1, Joveen Wan Fen Neoh2, Tiek Ying Lau2, Yvonne Ai‑Lian Lim3,4, Hwa Chia Chai5, Kek Heng Chua5 and Ping‑Chin Lee1* Abstract Background: Understanding the genetic diversity of candidate genes for malaria vaccines such as circumsporozo‑ ite protein (csp) may enhance the development of vaccines for treating Plasmodium knowlesi. Hence, the aim of this study is to investigate the genetic diversity of non‑repeat regions of csp in P. knowlesi from Malaysian Borneo and Peninsular Malaysia. Methods: A total of 46 csp genes were subjected to polymerase chain reaction amplifcation. The genes were obtained from P. knowlesi isolates collected from diferent divisions of Sabah, Malaysian Borneo, and Peninsular Malay‑ sia. The targeted gene fragments were cloned into a commercial vector and sequenced, and a phylogenetic tree was constructed while incorporating 168 csp sequences retrieved from the GenBank database. The genetic diversity and natural evolution of the csp sequences were analysed using MEGA6 and DnaSP ver. 5.10.01. A genealogical network of the csp haplotypes was generated using NETWORK ver. 4.6.1.3. Results: The phylogenetic analysis revealed indistinguishable clusters of P. knowlesi isolates across diferent geo‑ graphic regions, including Malaysian Borneo and Peninsular Malaysia. Nucleotide analysis showed that the csp non‑ repeat regions of zoonotic P. knowlesi isolates obtained in this study underwent purifying selection with population expansion, which was supported by extensive haplotype sharing observed between humans and macaques. -

The Push for Local Production, Costs and Benefits – a Case Study of Uganda’S Quality Chemicals
The push for local production, costs and benefits – A case study of Uganda’s Quality Chemicals Africa Fighting Malaria Policy Paper September 2009 James Taylor1, Roger Bate2,3, Emily Putze2, Richard Tren3 1 Graduate Student, Columbia University (SIPA) 2 American Enterprise Institute 3 Africa Fighting Malaria 1 Abstract Many Africans lack access to essential medicines. There are myriad reasons for this: poverty, lack of awareness about the need for treatment, confusion over which drugs to take, technical and logistical challenges in procurement and distribution combined with a general lack of local healthcare staff and infrastructure, among other cultural and political factors. One additional problem is the relatively high price of drugs, which the international community has prioritized by encouraging competition from various generic producers often through compulsory licensing. The latest cost-reduction strategy is the push for local drug production. But, as shown by the start-up problems of Quality Chemicals Industries Limited in Uganda, many burdens and barriers to access continue to seriously hinder the success of such enterprises. Indirect government subsidies to exporters selling into African markets, and pressure by donors and lobbyists on innovator producers to offer developing countries subsidized prices, actually undermine the competitiveness and viability of these nascent firms. Furthermore, the focus on drug pricing and local production can actually undermine the overall aim to increase access to medicines. Introduction “Essential medicines save lives and improve health when they are available, affordable, of assured quality and properly used.”4 Still, a lack of access to these life-saving medicines in developing countries remains one of the most pressing global public health concerns. -

Genome Annotation with Companion (Part 1)
Genome Annotation with Companion (Part 1) Companion, is an online pipeline that employs different software to annotate and compare an assembled sequence to a reference-annotated genome. The figure below illustrates the Companion pipeline, the software used and the expected output. For this exercise, we will start with an assembled genome that is unannotated. We will obtain the assembled FASTA files from EuPathDB sites. Companion can be accessed here: http://protozoacompanion.gla.ac.uk/ Each group will download one of the following genomes (the tinyURL links will initiate the download) and will use Companion to compare with the specified genome as reference. Group 1 – Plasmodium coatneyi Hackeri using Plasmodium knowlesi as reference https://tinyurl.com/yxuyqszu Group 2 - Plasmodium coatneyi Hackeri using Plasmodium falciparum as reference https://tinyurl.com/yxuyqszu Group 3 – Cryptosporidium meleagridis using Cryptosporidium parvum as reference https://tinyurl.com/yyqxgr5q Group 4 Cryptosporidium baileyi using Cryptosporidium parvum as reference https://tinyurl.com/yyffffrd Group 5 Leishmania amazonensis using Leishmania major as reference https://tinyurl.com/yy5wkymk Group 6 Trypanosoma congolense using Trypanosoma brucei 927 as reference. https://tinyurl.com/y6yqys7w A word about downloads: TinyUrls above are direct links to our genome FASTA files in the corresponding EuPathDB site downloads section. All genomes in EuPathDB sites are available for download from the “Data File” download section, which you can access from the Downloads menu in the gray tool bar. Selecting the Data Files option takes you to the download directories where you can navigate to the genome and data type you are looking for. To download specific contigs/scaffolds/chromosomes instead of entire genomes, use a genomic sequence search and place the desired sequences into your basket. -

Malaria in the ‘Omics Era’
G C A T T A C G G C A T genes Review Malaria in the ‘Omics Era’ Mirko Pegoraro and Gareth D. Weedall * School of Biological and Environmental Sciences, Liverpool John Moores University, Liverpool L3 3AF, UK; [email protected] * Correspondence: [email protected] Abstract: Genomics has revolutionised the study of the biology of parasitic diseases. The first Eukaryotic parasite to have its genome sequenced was the malaria parasite Plasmodium falciparum. Since then, Plasmodium genomics has continued to lead the way in the study of the genome biology of parasites, both in breadth—the number of Plasmodium species’ genomes sequenced—and in depth— massive-scale genome re-sequencing of several key species. Here, we review some of the insights into the biology, evolution and population genetics of Plasmodium gained from genome sequencing, and look at potential new avenues in the future genome-scale study of its biology. Keywords: Plasmodium; malaria; genomics; methylomics; methylation 1. Introduction Since the genome of the malaria parasite Plasmodium falciparum was published in 2002 [1], alongside that of its mosquito vector [2] and its human host (Consortium and International Human Genome Sequencing Consortium, 2001) [3], malaria genomics has led the way in the study of eukaryotic pathogens. Since then, a growing number of Plasmodium species’ genomes have been sequenced and large-scale population resequencing Citation: Pegoraro, M.; Weedall, G.D. studies have been carried out in P. falciparum and several other species. These efforts have Malaria in the ‘Omics Era’. Genes allowed the evolutionary and population genomics of malaria parasites to be studied in 2021, 12, 843.