00 PWG-Titledisc.Fm
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Utility of the Digital Rectal Examination in the Emergency Department: a Review
The Journal of Emergency Medicine, Vol. 43, No. 6, pp. 1196–1204, 2012 Published by Elsevier Inc. Printed in the USA 0736-4679/$ - see front matter http://dx.doi.org/10.1016/j.jemermed.2012.06.015 Clinical Reviews UTILITY OF THE DIGITAL RECTAL EXAMINATION IN THE EMERGENCY DEPARTMENT: A REVIEW Chad Kessler, MD, MHPE*† and Stephen J. Bauer, MD† *Department of Emergency Medicine, Jesse Brown VA Medical Center and †University of Illinois-Chicago College of Medicine, Chicago, Illinois Reprint Address: Chad Kessler, MD, MHPE, Department of Emergency Medicine, Jesse Brown Veterans Hospital, 820 S Damen Ave., M/C 111, Chicago, IL 60612 , Abstract—Background: The digital rectal examination abdominal pain and acute appendicitis. Stool obtained by (DRE) has been reflexively performed to evaluate common DRE doesn’t seem to increase the false-positive rate of chief complaints in the Emergency Department without FOBTs, and the DRE correlated moderately well with anal knowing its true utility in diagnosis. Objective: Medical lit- manometric measurements in determining anal sphincter erature databases were searched for the most relevant arti- tone. Published by Elsevier Inc. cles pertaining to: the utility of the DRE in evaluating abdominal pain and acute appendicitis, the false-positive , Keywords—digital rectal; utility; review; Emergency rate of fecal occult blood tests (FOBT) from stool obtained Department; evidence-based medicine by DRE or spontaneous passage, and the correlation be- tween DRE and anal manometry in determining anal tone. Discussion: Sixteen articles met our inclusion criteria; there INTRODUCTION were two for abdominal pain, five for appendicitis, six for anal tone, and three for fecal occult blood. -

The Differences Between ICD-9 and ICD-10
Preparing for the ICD-10 Code Set: Fact Sheet 2 October 1, 2015 Compliance Date Get the Facts to be Compliant Alert: The new ICD-10 compliance date is October 1, 2015. The Differences Between ICD-9 and ICD-10 This is the second fact sheet in a series and is focused on the differences between the ICD-9 and ICD-10 code sets. Collectively, the fact sheets will provide information, guidance, and checklists to assist you with understanding what you need to do to implement the ICD-10 code set. The ICD-10 code sets are not a simple update of the ICD-9 code set. The ICD-10 code sets have fundamental changes in structure and concepts that make them very different from ICD-9. Because of these differences, it is important to develop a preliminary understanding of the changes from ICD-9 to ICD-10. This basic understanding of the differences will then identify more detailed training that will be needed to appropriately use the ICD-10 code sets. In addition, seeing the differences between the code sets will raise awareness of the complexities of converting to the ICD-10 codes. Overall Comparisons of ICD-9 to ICD-10 Issues today with the ICD-9 diagnosis and procedure code sets are addressed in ICD-10. One concern today with ICD-9 is the lack of specificity of the information conveyed in the codes. For example, if a patient is seen for treatment of a burn on the right arm, the ICD-9 diagnosis code does not distinguish that the burn is on the right arm. -

HIGH-SENSITIVITY GUAIAC-BASED FECAL OCCULT BLOOD TEST (HSGFOBT) Anyone Can Get Colon Cancer
GET SCREENED: DETECT ANDDETECT PREVENT AND PREVENT COLON CANCER COLON CANCER TEST TYPE: HIGH-SENSITIVITY GUAIAC-BASED FECAL OCCULT BLOOD TEST (HSGFOBT) Anyone can get colon cancer. It can affect people of all racial and ethnic groups. Routine screening can help your health care provider find cancers earlier, when they are easier to treat. Screening may also prevent cancer, by finding and removing polyps or abnormal growths from the colon. COLON CANCER SCREENING There are different test options for screening. Talk with your provider to choose FACT SHEET the test that’s right for you. WHO? Adults who are at average risk for colon WHERE? You do this test at home. cancer may have an HSgFOBT. Talk with your health WHY? HSgFOBT detects signs of colon and rectal care provider about your risk and what age to begin cancer. It can also detect some polyps, which are screening. If you are at an increased risk of colon growths that could become cancer later. cancer, you may need screening early or this test may not be right for you. Discuss your medical and family HOW? You may have a restricted diet starting a medical history with your provider before choosing a few days before the test. You will get a kit from your test. Tell them if you have any of these risk factors: provider with instructions about how to take a sample A history of colon cancer or precancerous polyps of stool from three bowel movements in a row that A parent, sibling or child with colon cancer or you collect into a clean container. -

Unenhanced Areas Revealed by Contrast-Enhanced Abdominal Ultrasonography with Sonazoidtm Potentially Correspond to Colorectal Cancer
4012 EXPERIMENTAL AND THERAPEUTIC MEDICINE 12: 4012-4016, 2016 Unenhanced areas revealed by contrast-enhanced abdominal ultrasonography with SonazoidTM potentially correspond to colorectal cancer MINORU TOMIZAWA1, MIZUKI TOGASHI2, FUMINOBU SHINOZAKI3, RUMIKO HASEGAWA4, YOSHINORI SHIRAI4, MIDORI NORITAKE2, YUKIE MATSUOKA2, HIROAKI KAINUMA2, YASUJI IWASAKI2, KAZUNORI FUGO5, YASUFUMI MOTOYOSHI6, TAKAO SUGIYAMA7, SHIGENORI YAMAMOTO8, TAKASHI KISHIMOTO5 and NAOKI ISHIGE9 Departments of 1Gastroenterology; 2Clinical Laboratory; 3Radiology and 4Surgery, National Hospital Organization, Shimoshizu Hospital, Yotsukaido City, Chiba 284-0003; 5Department of Molecular Pathology, Chiba University Graduate School of Medicine, Chiba City, Chiba 260-8670; Departments of 6Neurology; 7Rheumatology; 8Pediatrics and 9Neurosurgery, National Hospital Organization, Shimoshizu Hospital, Yotsukaido, Yotsukaido City, Chiba 284-0003, Japan Received September 18, 2015; Accepted September 22, 2016 DOI: 10.3892/etm.2016.3868 Abstract. The present study investigated the potential utility of Introduction contrast-enhanced abdominal ultrasonography (CEUS), using SonazoidTM, in colorectal cancer (CRC). Three patients were Colorectal cancer (CRC) is commonly observed in clinical subjected to CEUS with SonazoidTM. Surgical specimens were settings (1). To improve the prognosis in patients with CRC, immunostained for CD31. Numbers of blood vessels positive prompt and accurate diagnosis is essential. Screening for CRC for CD31 were analyzed in each of five fields at x400 magnifi- is performed using fecal occult blood testing, and is diagnosed cation and averaged to determine blood vessel density. Blood with colonoscopy (2). vessel density was compared between non-tumorous and Abdominal ultrasound (US) is useful for the safe and tumorous areas. Prior to the administration of SonazoidTM, easy diagnosis of patients (3-6). During US screening of the CRC was illustrated as irregular-shaped wall thickening. -
Appendectomy: Simple Appendicitis
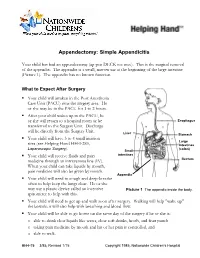
Appendectomy: Simple Appendicitis Your child has had an appendectomy (ap pen DECK toe mee). This is the surgical removal of the appendix. The appendix is a small, narrow sac at the beginning of the large intestine (Picture 1). The appendix has no known function. What to Expect After Surgery . Your child will awaken in the Post Anesthesia Care Unit (PACU) near the surgery area. He or she may be in the PACU for 1 to 2 hours. After your child wakes up in the PACU, he or she will return to a hospital room or be Esophagus transferred to the Surgery Unit. Discharge will be directly from the Surgery Unit. Liver Stomach . Your child will have 3 to 4 small incision Large sites (see Helping Hand HH-I-283, Intestines Laparoscopic Surgery (colon) ). Small . Your child will receive fluids and pain intestines medicine through an intravenous line (IV). Rectum When your child can take liquids by mouth, pain medicine will also be given by mouth. Appendix . Your child will need to cough and deep-breathe often to help keep the lungs clear. He or she may use a plastic device called an incentive Picture 1 The appendix inside the body. spirometer to help with this. Your child will need to get up and walk soon after surgery. Walking will help "wake up" the bowels; it will also help with breathing and blood flow. Your child will be able to go home on the same day of the surgery if he or she is: o able to drink clear liquids like water, clear soft drinks, broth, and fruit punch o taking pain medicine by mouth and his or her pain is controlled, and o able to walk. -

Dysphagia - Pathophysiology of Swallowing Dysfunction, Symptoms, Diagnosis and Treatment
ISSN: 2572-4193 Philipsen. J Otolaryngol Rhinol 2019, 5:063 DOI: 10.23937/2572-4193.1510063 Volume 5 | Issue 3 Journal of Open Access Otolaryngology and Rhinology REVIEW ARTICLE Dysphagia - Pathophysiology of Swallowing Dysfunction, Symptoms, Diagnosis and Treatment * Bahareh Bakhshaie Philipsen Check for updates Department of Otorhinolaryngology-Head and Neck Surgery, Odense University Hospital, Denmark *Corresponding author: Dr. Bahareh Bakhshaie Philipsen, Department of Otorhinolaryngology-Head and Neck Surgery, Odense University Hospital, Sdr. Boulevard 29, 5000 Odense C, Denmark, Tel: +45 31329298, Fax: +45 66192615 the vocal folds adduct to prevent aspiration. The esoph- Abstract ageal phase is completely involuntary and consists of Difficulty swallowing is called dysphagia. There is a wide peristaltic waves [2]. range of potential causes of dysphagia. Because there are many reasons why dysphagia can occur, treatment Dysphagia is classified into the following major depends on the underlying cause. Thorough examination types: is important, and implementation of a treatment strategy should be based on evaluation by a multidisciplinary team. 1. Oropharyngeal dysphagia In this article, we will describe the mechanism of swallowing, the pathophysiology of swallowing dysfunction and different 2. Esophageal dysphagia causes of dysphagia, along with signs and symptoms asso- 3. Complex neuromuscular disorders ciated with dysphagia, diagnosis, and potential treatments. 4. Functional dysphagia Keywords Pathophysiology Dysphagia, Deglutition, Deglutition disorders, FEES, Video- fluoroscopy Swallowing is a complex process and many distur- bances in oropharyngeal and esophageal physiology including neurologic deficits, obstruction, fibrosis, struc- Introduction tural damage or congenital and developmental condi- Dysphagia is derived from the Greek phagein, means tions can result in dysphagia. Breathing difficulties can “to eat” [1]. -

Laparoscopy in Emergency Hernia Repair
Review Article Page 1 of 11 Laparoscopy in emergency hernia repair George P.C. Yang Department of Surgery, Hong Kong Adventist Hospital, Hong Kong, China Correspondence to: George Pei Cheung Yang, FRACS. Department of Surgery, Hong Kong Adventist Hospital, 40 Stubbs Road, Hong Kong, China. Email: [email protected]. Abstract: Minimal access surgery (MAS) or laparoscopic surgery has revolutionized our surgical world since its introduction in the 1980s. Its benefits of faster recovery, lesser wound pain which in turn reduced respiratory complications, allows earlier mobilization, minimize deep vein thrombosis, minimize wound infection rate are well reported and accepted. It also has significant long-term benefits which are often neglected by many, such as reduced risk of incisional hernia and lesser risk of intestinal obstruction from post-operative bowel adhesion. The continuous development and improvement in laparoscopic equipment and instruments, together with the better understanding of laparoscopic anatomy and refinement of laparoscopic surgical techniques, has enable laparoscopic surgery to evolve further. The evolution allows its application to include not only elective conditions, but also emergency surgical conditions. Performing laparoscopy and laparoscopic procedure under surgical emergencies require extra cautions. These procedures should be performed by expert in these fields together with experienced supporting staffs and the availability of appropriate equipment and instruments. Laparoscopic management for emergency groin hernia conditions has been reported by centers expert in laparoscopic hernia surgery. However, laparoscopy in emergency hernia repair includes a wide variety of meanings. Often in the different reports series one will see different meanings for laparoscopic repair and open conversion when reading in details. -
Flexible Sigmoidoscopy in Asymptomatic Patients with Negative Fecal Occult Blood Tests Joy Garrison Cauffman, Phd, Jimmy H
Flexible Sigmoidoscopy in Asymptomatic Patients with Negative Fecal Occult Blood Tests Joy Garrison Cauffman, PhD, Jimmy H. Hara, MD, Irving M. Rasgon, MD, and Virginia A. Clark, PhD Los Angeles, California Background. Although the American Cancer Society and tients with lesions were referred for colonoscopy; addi others haw established guidelines for colorectal cancer tional lesions were found in 14%. A total of 62 lesions screening, questions of who and how to screen still exist. were discovered, including tubular adenomas, villous Methods. A 60-crn flexible sigmoidoscopy was per adenomas, tubular villous adenomas (23 of the adeno formed on 1000 asymptomatic patients, 45 years of mas with atypia), and one adenocarcinoma. The high age or older, with negative fecal occult blood tests, est percentage of lesions discovered were in the sig who presented for routine physical examinations. Pa moid colon and the second highest percentage were in tients with clinically significant lesions were referred for the ascending colon. colonoscopy. The proportion of lesions that would not Conclusions. The 60-cm flexible sigmoidoscope was have been found if the 24-cm rigid or the 30-cm flexi able to detect more lesions than either the 24-cm or ble sigmoidoscope had been used was identified. 30-cm sigmoidoscope when used in asymptomatic pa Results. Using the 60-cm flexible sigmoidoscope, le tients, 45 years of age and over, with negative fecal oc sions were found in 3.6% of the patients. Eighty per cult blood tests. When significant lesions are discovered cent of the significant lesions were beyond the reach of by sigmoidoscopy, colonoscopy should be performed. -

Evidence Vs Experience in the Surgical Management of Necrotizing Enterocolitis and Focal Intestinal Perforation
Journal of Perinatology (2008) 28, S14–S17 r 2008 Nature Publishing Group All rights reserved. 0743-8346/08 $30 www.nature.com/jp ORIGINAL ARTICLE Evidence vs experience in the surgical management of necrotizing enterocolitis and focal intestinal perforation CJ Hunter1,2, N Chokshi1,2 and HR Ford1,2 1Department of Surgery, University of Southern California Keck School of Medicine, Los Angeles, CA, USA and 2Department of Surgery, Childrens Hospital Los Angeles, Los Angeles, CA, USA bacterial colonization and prematurity.4 There is a subset of low Introduction: Necrotizing enterocolitis (NEC) and focal intestinal birth weight infants, however, that sustain focal intestinal perforation (FIP) are neonatal intestinal emergencies that affect premature perforation (FIP) without classic clinical, radiographic, or infants. Although most cases of early NEC can be successfully managed with histological evidence of NEC.5 FIP appears to be a distinct clinical medical therapy, prompt surgical intervention is often required for advanced entity that occurs in 3% of very low birth weight (VLBW) infants or perforated NEC and FIP. and accounts for 44% of gastrointestinal perforations in this 6 Method: The surgical management and treatment of FIP and NEC are population. Optimal surgical management of severe NEC and discussed on the basis of literature review and our personal experience. FIP has been the subject of ongoing controversy for many years. Result: Surgical options are diverse, and include peritoneal drainage, laparotomy with diverting ostomy alone, laparotomy with intestinal Presentation of NEC and FIP resection and primary anastomosis or stoma creation, with or without Infants with NEC typically present with feeding intolerance and second-look procedures. -
Laparoscopic Totally Extraperitoneal Inguinal Hernia Repair: Lessons Learned from 3,100 Hernia Repairs Over 15 Years
Surg Endosc (2009) 23:482–486 DOI 10.1007/s00464-008-0118-3 Laparoscopic totally extraperitoneal inguinal hernia repair: lessons learned from 3,100 hernia repairs over 15 years Jean-Louis Dulucq Æ Pascal Wintringer Æ Ahmad Mahajna Received: 30 November 2007 / Accepted: 14 July 2008 / Published online: 23 September 2008 Ó Springer Science+Business Media, LLC 2008 Abstract Mean operative time was 17 min in unilateral hernia and Background Two revolutions in inguinal hernia repair 24 min in bilateral hernia. There were 36 hernias (1.2%) surgery have occurred during the last two decades. The first that required conversion: 12 hernias were converted to was the introduction of tension-free hernia repair by open anterior Liechtenstein and 24 to laparoscopic TAPP Liechtenstein in 1989 and the second was the application of technique. The incidence of intraoperative complications laparoscopic surgery to the treatment of inguinal hernia in was low. Most of the patients were discharged at the sec- the early 1990s. The purposes of this study were to assess ond day of the surgery. The overall postoperative morbidity the safety and effectiveness of laparoscopic totally extra- rate was 2.2%. The incidence of recurrence rate was peritoneal (TEP) repair and to discuss the technical changes 0.35%. The recurrence rate for the first 200 repairs was that we faced on the basis of our accumulative experience. 2.5%, but it decreased to 0.47% for the subsequent 1,254 Methods Patients who underwent an elective inguinal hernia repairs hernia repair at the Department of Abdominal Surgery at Conclusion According to our experience, in the hands of the Institute of Laparoscopic Surgery (ILS), Bordeaux, experienced laparoscopic surgeons, laparoscopic hernia between June 1990 and May 2005 were enrolled retro- repair seems to be the favored approach for most types of spectively in this study. -

Ventral Hernia Repair
AMERICAN COLLEGE OF SURGEONS • DIVISION OF EDUCATION Ventral Hernia Repair Benefits and Risks of Your Operation Patient Education B e n e fi t s — An operation is the only This educational information is way to repair a hernia. You can return to help you be better informed to your normal activities and, in most about your operation and cases, will not have further discomfort. empower you with the skills and Risks of not having an operation— knowledge needed to actively The size of your hernia and the pain it participate in your care. causes can increase. If your intestine becomes trapped in the hernia pouch, you will have sudden pain and vomiting Keeping You Common Sites for Ventral Hernia and require an immediate operation. Informed If you decide to have the operation, Information that will help you possible risks include return of the further understand your operation The Condition hernia; infection; injury to the bladder, and your role in healing. A ventral hernia is a bulge through blood vessels, or intestines; and an opening in the muscles on the continued pain at the hernia site. Education is provided on: abdomen. The hernia can occur at a Hernia Repair Overview .................1 past incision site (incisional), above the navel (epigastric), or other weak Condition, Symptoms, Tests .........2 Expectations muscle sites (primary abdominal). Treatment Options….. ....................3 Before your operation—Evaluation may include blood work, urinalysis, Risks and Common Symptoms Possible Complications ..................4 ultrasound, or a CT scan. Your surgeon ● Visible bulge on the abdomen, and anesthesia provider will review Preparation especially with coughing or straining your health history, home medications, and Expectations .............................5 ● Pain or pressure at the hernia site and pain control options. -
Exploratory Laparotomy.Docx
EXPLORATORY LAPAROTOMY CONSENT FORM Your physician has determined that you may have a disease or abnormality inside your abdomen which may be life threatening, preventing pregnancy or causing medical problems if not treated. An exploratory laparotomy is an operation in which the doctor makes a surgical “cut” in the belly. Sometimes this operation is done to make sure that no disease or abnormality exists. If the physician finds that a disease is found or if the physician doesn’t feel that corrective surgery should be done immediately, then he will close up the surgical cut. If major corrective surgery is done the risk will be greater than if no corrective surgery is done. It is possible that you will be worse after the operation. Your physician can make no guarantee as to the result that might be obtained from this operation. Complications from exploratory surgery of the abdomen without any corrective surgery are infrequent, but they do occur. As with any surgical procedure, complications from bleeding and infection can occur. These complications can result in prolonged illness, the need for blood transfusions, poor healing wounds, scarring and the need for further operations. Other uncommon complications of this operation include: Damage to the intestines, blocked bowels, hernia or “rupture” developing at the site of the surgical cut, heart attacks or stroke, blood clots in the lungs and pneumonia. Some complications of exploratory surgery of the abdomen may require further surgery, some can cause permanent deformity and rarely, some can even be fatal. Furthermore, there may be alternative therapeutic or diagnostic methods available to you in addition to exploratory surgery.