Nonpublication of Trial Results for New Neurological Drugs: a Systematic Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

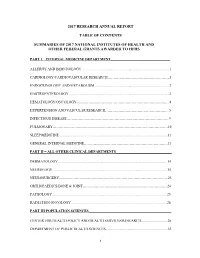
R Graphics Output
Dexamethasone sodium phosphate ( 0.339 ) Melengestrol acetate ( 0.282 ) 17beta−Trenbolone ( 0.252 ) 17alpha−Estradiol ( 0.24 ) 17alpha−Hydroxyprogesterone ( 0.238 ) Triamcinolone ( 0.233 ) Zearalenone ( 0.216 ) CP−634384 ( 0.21 ) 17alpha−Ethinylestradiol ( 0.203 ) Raloxifene hydrochloride ( 0.203 ) Volinanserin ( 0.2 ) Tiratricol ( 0.197 ) trans−Retinoic acid ( 0.192 ) Chlorpromazine hydrochloride ( 0.191 ) PharmaGSID_47315 ( 0.185 ) Apigenin ( 0.183 ) Diethylstilbestrol ( 0.178 ) 4−Dodecylphenol ( 0.161 ) 2,2',6,6'−Tetrachlorobisphenol A ( 0.156 ) o,p'−DDD ( 0.155 ) Progesterone ( 0.152 ) 4−Hydroxytamoxifen ( 0.151 ) SSR150106 ( 0.149 ) Equilin ( 0.3 ) 3,5,3'−Triiodothyronine ( 0.256 ) 17−Methyltestosterone ( 0.242 ) 17beta−Estradiol ( 0.24 ) 5alpha−Dihydrotestosterone ( 0.235 ) Mifepristone ( 0.218 ) Norethindrone ( 0.214 ) Spironolactone ( 0.204 ) Farglitazar ( 0.203 ) Testosterone propionate ( 0.202 ) meso−Hexestrol ( 0.199 ) Mestranol ( 0.196 ) Estriol ( 0.191 ) 2,2',4,4'−Tetrahydroxybenzophenone ( 0.185 ) 3,3,5,5−Tetraiodothyroacetic acid ( 0.183 ) Norgestrel ( 0.181 ) Cyproterone acetate ( 0.164 ) GSK232420A ( 0.161 ) N−Dodecanoyl−N−methylglycine ( 0.155 ) Pentachloroanisole ( 0.154 ) HPTE ( 0.151 ) Biochanin A ( 0.15 ) Dehydroepiandrosterone ( 0.149 ) PharmaCode_333941 ( 0.148 ) Prednisone ( 0.146 ) Nordihydroguaiaretic acid ( 0.145 ) p,p'−DDD ( 0.144 ) Diphenhydramine hydrochloride ( 0.142 ) Forskolin ( 0.141 ) Perfluorooctanoic acid ( 0.14 ) Oleyl sarcosine ( 0.139 ) Cyclohexylphenylketone ( 0.138 ) Pirinixic acid ( 0.137 ) -

204569Orig1s000
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 204569Orig1s000 MEDICAL REVIEW(S) Cross Discipline Team Leader Review 3. CMC/Device Dr. Khairuzzaman found the drug product portion of the NDA to be acceptable, and without need for phase 4 commitments. Dr. Sapru’s review stated that with the exception of a pending issue concerning the control of potential genotoxic impurity (b) (4) the NDA was approvable in terms of drug substance. Dr. Suarez found that the NDA was acceptable from a biopharmaceutics perspective. The Office of Compliance issuance of an acceptable recommendation for drug substance manufacturing and testing facilities was pending at the time of this review. 4. Nonclinical Pharmacology/Toxicology Dr. Richard Siarey completed the primary nonclinical review, and Dr. Lois Freed completed a supervisory memo. Dr. Siarey’s overall conclusion was that from a nonclinical perspective, approval of the suvorexant NDA was recommended. However, he found evidence that catapelxy was observed in dogs exposed to MK-4305 (suvorexant) near Tmax, although he concluded that additional information could have been gained by studying the drug in an experimental model that has been used for diagnosing cataplexy in dogs. Dr. Siarey suggested that since cataplexy occurred in dogs near Tmax, a time at which if used for insomnia patients would ordinarily be in bed, safety concern for humans was reduced. Dr. Siarey also found that the neurobehavioral assessment in the pre- and post-natal developmental study was not complete, as the passive avoidance tests was performed too early in development, while learning/acquisition tests and retention/memory tests were not conducted. -

(12) United States Patent (10) Patent No.: US 8.598,119 B2 Mates Et Al
US008598119B2 (12) United States Patent (10) Patent No.: US 8.598,119 B2 Mates et al. (45) Date of Patent: Dec. 3, 2013 (54) METHODS AND COMPOSITIONS FOR AOIN 43/00 (2006.01) SLEEP DSORDERS AND OTHER AOIN 43/46 (2006.01) DSORDERS AOIN 43/62 (2006.01) AOIN 43/58 (2006.01) (75) Inventors: Sharon Mates, New York, NY (US); AOIN 43/60 (2006.01) Allen Fienberg, New York, NY (US); (52) U.S. Cl. Lawrence Wennogle, New York, NY USPC .......... 514/114: 514/171; 514/217: 514/220; (US) 514/229.5: 514/250 (58) Field of Classification Search (73) Assignee: Intra-Cellular Therapies, Inc. NY (US) None See application file for complete search history. (*) Notice: Subject to any disclaimer, the term of this patent is extended or adjusted under 35 (56) References Cited U.S.C. 154(b) by 215 days. U.S. PATENT DOCUMENTS (21) Appl. No.: 12/994,560 6,552,017 B1 4/2003 Robichaud et al. 2007/0203120 A1 8, 2007 McDevitt et al. (22) PCT Filed: May 27, 2009 FOREIGN PATENT DOCUMENTS (86). PCT No.: PCT/US2O09/OO3261 S371 (c)(1), WO WOOOf77OO2 * 6, 2000 (2), (4) Date: Nov. 24, 2010 OTHER PUBLICATIONS (87) PCT Pub. No.: WO2009/145900 Rye (Sleep Disorders and Parkinson's Disease, 2000, accessed online http://www.waparkinsons.org/edu research/articles/Sleep PCT Pub. Date: Dec. 3, 2009 Disorders.html), 2 pages.* Alvir et al. Clozapine-Induced Agranulocytosis. The New England (65) Prior Publication Data Journal of Medicine, 1993, vol. 329, No. 3, pp. 162-167.* US 2011/0071080 A1 Mar. -

Anti-Infectives Industry Over the Next 5 Years and Beyond
Bridging the innovation gap... New Drug Futures: Products that could change the pharma market to 2013 and beyond Over 70 pipeline prospects This new major and insightful 450 page in 8 major therapy areas analysis evaluates, compares and contrasts the are analysed in this report prospects for the development compounds that could revolutionise the pharmaceutical Anti-infectives industry over the next 5 years and beyond. Cardiovascular CNS The report provides: Gastrointestinal Detailed background and market context for Metabolic each therapy area covered: Musculoskeletal Addressable patient population Oncology Current treatments Sales drivers Respiratory Sales breakers Future treatments Market dynamics – winners and losers Key drug launches by 2013 Unique sales forecasts by major product to 2013 Over 70 key products assessed Unique evaluation scores for key areas such as novelty of mechanism, clinical data and competition Critical and detailed appraisal of each product‟s research and development Extensive pipeline listings, putting the profiled products into their competitive context The search – and need – for new products has never been greater and what’s in the development pipeline has never generated more interest. That is why this analysis is so important! GLOBAL PHARMA MARKET IN CONTEXT THE Are there too many prophets of doom ready to write-off the research-based pharma industry in the future? Too few novel There is plenty on which to base such anxiety. The research-based industry products and an must achieve a fair price in the face of greater cost control, while the aggressive generic burden of regulation is setting the bar high for successful product sector are taking introduction. -

The Dual Orexin Receptor Antagonist TCS1102 Does Not Affect Reinstatement of Nicotine- Seeking
RESEARCH ARTICLE The dual orexin receptor antagonist TCS1102 does not affect reinstatement of nicotine- seeking Shaun Yon-Seng Khoo, Gavan P. McNally, Kelly J. Clemens* School of Psychology, University of New South Wales, Sydney, Australia * [email protected] a1111111111 a1111111111 a1111111111 Abstract a1111111111 a1111111111 The orexin/hypocretin system is important for appetitive motivation towards multiple drugs of abuse, including nicotine. Both OX1 and OX2 receptors individually have been shown to influence nicotine self-administration and reinstatement. Due to the increasing clinical use of dual orexin receptor antagonists in the treatment of disorders such as insomnia, we OPEN ACCESS examined whether a dual orexin receptor antagonist may also be effective in reducing nico- Citation: Khoo SY-S, McNally GP, Clemens KJ tine seeking. We tested the effect of intracerebroventricular (i.c.v.) administration of the (2017) The dual orexin receptor antagonist potent and selective dual orexin receptor antagonist TCS1102 on orexin-A-induced food TCS1102 does not affect reinstatement of nicotine- self-administration, nicotine self-administration and reinstatement of nicotine-seeking in seeking. PLoS ONE 12(3): e0173967. https://doi. org/10.1371/journal.pone.0173967 rats. Our results show that 30 μg of TCS1102 i.c.v. abolishes orexin-A-induced increases in food self-administration but does not reduce nicotine self-administration. Neither i.c.v. 10 μg Editor: Judith Homberg, Radboud University Medical Centre, NETHERLANDS nor 30 μg of TCS1102 reduced compound reinstatement after short-term (15 days) self- administration nicotine, but 30 μg transiently reduced cue/nicotine compound reinstatement Received: November 24, 2016 after chronic self-administration (29 days). -

Annual HFHS Publications List 2017 This Bibliography Aims to Recognize
Annual HFHS Publications List 2017 This bibliography aims to recognize the scholarly activity and provide ease of access to journal articles, meeting abstracts, book chapters, books and other works published by Henry Ford Health System personnel. Searches were conducted in PubMed, Embase, Web of Science, and Google Scholar during 2017, and then imported into EndNote for formatting. The searches captured over 1,500 unique publications from Henry Ford Health System authors for 2017. Click the “Full Text” link to view the articles to which Sladen Library provides access. If the full-text of the article is not available, you may request it through ILLiad by clicking on the “Article Request Form,” or by calling us at 313-916-2550. If you would like to be added to the monthly email distribution list to automatically receive a PDF of this bibliography in your inbox, or you have any questions or comments, please contact Angela Cabrera at [email protected]. Administration Omar J, Heidemann DL, Blum-Alexandar B, Uju-Eke C, Alam Z, Willens DE, and Wisdom K. Fresh prescription: Improving nutrition education and access to fresh produce in Detroit J Gen Intern Med 2017; 32(2):S752. PMID: Not assigned. Abstract Administration Smith KL, Fedel P, and Heitman J. Incapacitated surrogates: A new and increasing dilemma in hospital care J Clin Ethics 2017; 28(4):279-289. PMID: 29257763. Article Request Form Allergy Brown KR, Krouse RZ, Calatroni A, Visness CM, Sivaprasad U, Kercsmar CM, Matsui EC, West JB, Makhija MM, Gill MA, Kim H, Kattan M, Pillai D, Gern JE, Busse WW, Togias A, Liu AH, and Khurana Hershey GK. -
2017 Research Annual Report Table of Contents Summaries of 2017
2017 RESEARCH ANNUAL REPORT TABLE OF CONTENTS SUMMARIES OF 2017 NATIONAL INSTITUTES OF HEALTH AND OTHER FEDERAL GRANTS AWARDED TO HFHS PART I – INTERNAL MEDICINE DEPARTMENT_________________________________ ALLERGY AND IMMUNOLOGY ................................................................................................. 1 CARDIOLOGY/CARDIOVASCULAR RESEARCH…………………………………………….1 ENDOCRINOLOGY AND METABOLISM .................................................................................. 2 GASTROENTEROLOGY ............................................................................................................. .3 HEMATOLOGY/ONCOLOGY…………………………………………………………………...4 HYPERTENSION AND VASCULAR RESEARCH……………………………………………...5 INFECTIOUS DISEASE…………………………………………………………………………..9 PULMONARY……………………………………………………………………………………10 SLEEP MEDICINE ....................................................................................................................... 11 GENERAL INTERNAL MEDICINE…………………………………………………………….13 PART II – ALL OTHER CLINICAL DEPARTMENTS_______________________________ DERMATOLOGY ........................................................................................................................ 14 NEUROLOGY .............................................................................................................................. 15 NEUROSURGERY……………………………………………………………………………….23 ORTHOPAEDICS/BONE & JOINT……………………………………………………………..24 PATHOLOGY .............................................................................................................................. -

Novel Cyclodextrin Derivatives Presented at the 3Rd European Conference on Cyclodextrins
VOLUME 27. No. 11. NOVEMBER 2013 ISSN 0951-256X October 2-4, 2013, Antalya, Turkey Novel cyclodextrin derivatives presented at the 3rd European Conference on Cyclodextrins This year’s European Conference on Cyclodextrins organized by Prof. Erem Bilensoy, Hacettepe University, Ankara brought 50 oral presentations and 65 posters. Most of the presented works covered the main theme of the congress: ”multifunctional excipient potential of cyclodextrins in pharmaceutical, cosmetic and biomedical industries”. The large number of the presented works dealing with novel cyclodextrin derivatives clearly shows that recently there has been a renewed interest in functionalization of cyclodextrins in order to extend the utilization of these derivatives as tools in catalysis, drug delivery, formulation and stabilization of active molecules and cosmetic ingredients. This short paper gives a brief review of the presented novel cyclodextrin derivatives, summarizes their synthetic methodologies and the field of their applications. Extended abstracts will be published in the Journal of Inclusion Phenomena and Macrocyclic Chemistry after peer review. The references given here are the papers of the cited authors on similar topics presented at the conference. NOVEL CYCLODEXTRIN POLYMERS AND NANOSPONGES Phosphorus-containing cyclodextrin polymers presented by Prof. Catherine Amiel A very attractive new cyclodextrin (CD) based polymeric system presented by Prof. Amiel combines the advantages of cyclodextrin polymers (formation of inclusion complexes with apolar guests) and phosphorus-containing polymers (biocompatibility, calcium affinity). These VOLUME 27. No 11. polymeric systems are promising candidates to be used in biomedical applications that jointly require calcium delivery and transport of lipophilic bioactive molecules. A non-toxic cyclic sodium trimetaphosphate (STMP) was used as a cross-linking agent under basic conditions. -

Study Protocol
Confidential Page 1 Protocol No. Everolimus Investigator-initiated Protocol Template RAD001 (Everolimus) Clinical evaluation of everolimus (a rapamycin analog) in restoring salivary gland function to patients treated with radiotherapy for head and neck cancer CRAD001XUS274T Authors: Panayiotis Savvides, MD PhD MPH (Principal Investigator) Kirsten Limesand, PhD (co-Investigator) Denise Roe, DrPH (co-Investigator) Sun Yi, MD (co-Investigator) Julie Bauman, MD (co-Investigator) Daruka Mahadevan, MD PhD (co-Investigator) Version number: 1.2 Release date 06/22/2018 Referenced Investigator Brochure 15, release date 27-April-2016 Edition IRB NUMBER: PHXB-17-0072-70-15 IRB APPROVAL DATE: 07/03/2018 Confidential Page 2 Protocol No. Table of contents Table of contents..................................................................................................................2 List of figures.......................................................................................................................3 List of tables.........................................................................................................................3 List of abbreviations ............................................................................................................4 Glossary of terms.................................................................................................................6 Schema.................................................................................................................................8 1 -

Datasheet Inhibitors / Agonists / Screening Libraries a DRUG SCREENING EXPERT
Datasheet Inhibitors / Agonists / Screening Libraries A DRUG SCREENING EXPERT Product Name : Volinanserin Catalog Number : T5389 CAS Number : 139290-65-6 Molecular Formula : C22H28FNO3 Molecular Weight : 373.46 Description: Volinanserin (MDL 100907) is a potent and selective antagonist of the serotonin receptor 5-HT2 (Ki: 0.36 nM) and shows 300-fold selectivity for 5-HT2 receptor over 5-HT1c, alpha-1 adrenergic and sigma receptors. Storage: 2 years -80°C in solvent; 3 years -20°C powder; DMSO 100 mg/mL (267.8 mM) Solubility Ethanol 18 mg/mL (48.2 mM) ( < 1 mg/ml refers to the product slightly soluble or insoluble ) Receptor (IC50) 5-HT2 receptor 0.36 nM (Ki) In vitro Activity MDL 100,907 demonstrated low nanomolar or subnanomolar binding in vitro at the 5-HT2A receptor and showed a > 100-fold separation from all other receptors measured. MDL 100,907 had subnanomolar potency as a 5-HT2A antagonist in vitro in reversing 5-HT-stimulated inositol phosphate accumulation in NIH 3T3 cells transfected with the rat 5-HT2A receptor [2]. In vivo Activity In mice, MDL 100,907 blocked amphetamine-stimulated locomotion at doses that did not significantly affect apomorphine- stimulated climbing behavior. When administered chronically, MDL 100,907 selectively reduced the number of spontaneously active A10 neurons [1]. In vivo, MDL 100,907 potently inhibited 5-methoxy-N, N-dimethyltryptamine-induced head twitches in mice or 5-hydroxytryptophan-induced head twitches in rats. In vivo, functional tests in mice revealed a > 500-fold separation between doses that produced 5-HT2A antagonism and doses that produced alpha 1-adrenergic or striatal D2 antagonism [2]. -

A Phase 3, Multicenter, Randomized, Double-Blind
Official Title: A Phase 3, Multicenter, Randomized, Double-blind, Placebo-controlled Study to Evaluate the Efficacy and Safety of Adjunctive Pimavanserin in Subjects With Major Depressive Disorder and Inadequate Response to Antidepressant Treatment NCT Number: NCT03999918 Document Date: 21 Jun 2020 CLINICAL STUDY PROTOCOL UNMASKED PROTOCOL A Phase 3, Multicenter, Randomized, Double-blind, Placebo-controlled Study to Evaluate the Efficacy and Safety of Adjunctive Pimavanserin in Subjects With Major Depressive Disorder and Inadequate Response to Antidepressant Treatment Protocol Number: ACP-103-054 Amendment 4 EudraCT Number: 2018-003251-37 Original Protocol Date: 30 August 2018 Protocol Amendment 1 Date: 05 December 2018 Protocol Amendment 2 Date: 18 March 2019 Protocol Amendment 3 Date: 29 October 2019 Protocol Amendment 4 Date: 21 June 2020 Confidentiality Statement This protocol is the confidential information of ACADIA Pharmaceuticals Inc. and is intended solely for the guidance of the clinical investigation. This protocol may not be disclosed to parties not associated with the clinical investigation or used for any purpose without the prior written consent of ACADIA Pharmaceuticals Inc. Confidential and Proprietary Information of ACADIA Pharmaceuticals Inc. Page 1 of 81 Study: ACP-103-054 Final Version: 1.0 Clinical Study Protocol Amendment 4 UNMASKED VERSION Date: 21 June 2020 SPONSOR SIGNATURE PAGE Title: A Phase 3, Multicenter, Randomized, Double-blind, Placebo-controlled Study to Evaluate the Efficacy and Safety of Adjunctive Pimavanserin in Subjects With Major Depressive Disorder and Inadequate Response to Antidepressant Treatment ACADIA President: President ACADIA Pharmaceuticals Inc. See appended electronic signature page Signature Date ACADIA Study Lead: Executive Director, Clinical Research ACADIA Pharmaceuticals Inc. -

Emerging Anti-Insomnia Drugs: Tackling Sleeplessness and the Quality of Wake Time
REVIEWS Emerging anti-insomnia drugs: tackling sleeplessness and the quality of wake time Keith A. Wafford* and Bjarke Ebert‡ Abstract | Sleep is essential for our physical and mental well being. However, when novel hypnotic drugs are developed, the focus tends to be on the marginal and statistically significant increase in minutes slept during the night instead of the effects on the quality of wakefulness. Recent research on the mechanisms underlying sleep and the control of the sleep–wake cycle has the potential to aid the development of novel hypnotic drugs; however, this potential has not yet been realized. Here, we review the current understanding of how hypnotic drugs act, and discuss how new, more effective drugs and treatment strategies for insomnia might be achieved by taking into consideration the daytime consequences of disrupted sleep. Primary insomnia Humans spend approximately one-third of their lifetime Insomnia is defined as difficulty in initiating and/or Patients who suffer from sleeping, but we still know relatively little about why this maintaining sleep. The incidence of insomnia in the gen- sleeplessness for at least process is so critical for every living animal. Current eral population is between 10–30%, and approximately 1 month that cannot be thinking suggests that waking activity is relatively 50% of the cases complain of serious daytime conse- attributed to a medical, dynamic in terms of using the body’s resources: breaking quences, such as inability to concentrate, reduced energy psychiatric or an environmental cause (such as drug abuse or down proteins, gathering information and expending and memory problems. When this persists for more medications).