Autism Information
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
L Brown Presentation
Health Equity Learning Series Beyond Service Provision and Disparate Outcomes: Disability Justice Informing Communities of Practice HEALTH EQUITY LEARNING SERIES 2016-17 GRANTEES • Aurora Mental Health Center • Northwest Colorado Health • Bright Futures • Poudre Valley Health System • Central Colorado Area Health Education Foundation (Vida Sana) Center • Pueblo Triple Aim Corporation • Colorado Cross-Disability Coalition • Rural Communities Resource Center • Colorado Latino Leadership, Advocacy • Southeast Mental Health Services and Research Organization • The Civic Canopy • Cultivando • The Gay, Lesbian, Bisexual, and • Eagle County Health and Human Transgender Community Center of Services Colorado • El Centro AMISTAD • Tri-County Health Network • El Paso County Public Health • Warm Cookies of the Revolution • Hispanic Affairs Project • Western Colorado Area Health Education Center HEALTH EQUITY LEARNING SERIES Lydia X. Z. Brown (they/them) • Activist, writer and speaker • Past President, TASH New England • Chairperson, Massachusetts Developmental Disabilities Council • Board member, Autism Women’s Network ACCESS NOTE Please use this space as you need or prefer. Sit in chairs or on the floor, pace, lie on the floor, rock, flap, spin, move around, step in and out of the room. CONTENT/TW I will talk about trauma, abuse, violence, and murder of disabled people, as well as forced treatment and institutions, and other acts of violence, including sexual violence. Please feel free to step out of the room at any time if you need to. BEYOND SERVICE -

The Cerebral Subject and the Challenge of Neurodiversity
BioSocieties (2009), 4, 425–445 ª London School of Economics and Political Science doi:10.1017/S1745855209990287 The Cerebral Subject and the Challenge of Neurodiversity Francisco Ortega Institute for Social Medicine, State University of Rio de Janeiro, Rua Saˇ o Francisco Xavier 524, Rio de Janeiro CEP 20550-900, Brazil E-mail: [email protected] Abstract The neurodiversity movement has so far been dominated by autistic people who believe their condition is not a disease to be treated and, if possible, cured, but rather a human specificity (like sex or race) that must be equally respected. Autistic self-advocates largely oppose groups of parents of autistic children and professionals searching for a cure for autism. This article discusses the posi- tions of the pro-cure and anti-cure groups. It also addresses the emergence of autistic cultures and various issues concerning autistic identities. It shows how identity issues are frequently linked to a ‘neurological self-awareness’ and a rejection of psychological interpretations. It argues that the preference for cerebral explanations cannot be reduced to an aversion to psychoanalysis or psychological culture. Instead, such preference must be understood within the context of the dif- fusion of neuroscientific claims beyond the laboratory and their penetration in different domains of life in contemporary biomedicalized societies. Within this framework, neuroscientific theories, prac- tices, technologies and therapies are influencing the ways we think about ourselves and relate to others, favoring forms of neurological or cerebral subjectivation. The article shows how neuroscien- tific claims are taken up in the formation of identities, as well as social and community networks. -

Heller 7-Day Neurodiversity Inclusion Challenge-Introduction
The 7-Day Neurodiversity Inclusion Challenge at Heller Introduction Many people are unfamiliar with the term “neurodiversity,” a concept originating in the autistic community and made widely known, in particular, by Jim Sinclair, a pioneer of autistic self-advocacy. Briefly, “neurodiversity” refers to the range of neurological divergence from “neurotypical” patterns of cognition. The term and concept originated from the neurodiversity movement, a social movement that argues that society should accommodate and include people with neurological disabilities rather than seek to cure them or enforce typical behavior. Human minds vary, and these variations do not all require a cure. The term also can imply that no typical or normal brain exists at all; all brains are variations on a theme. Associated primarily with autism (now known clinically as autism spectrum disorder [ASD]), neurodiversity usually also includes attention-deficit/hyperactivity disorder (ADHD), dyslexia, and dyspraxia as well as many other conditions. Some apply the term not only to innate conditions but also to acquired conditions, for example, neurological divergence caused by brain injury. Different disability communities have different politics. While some do seek cures or other interventions designed to promote typical function, a growing number of communities have adopted the neurodiversity framework as offering a better approach to research, support, and advocacy. While neurodiversity is consistent with services and supports designed to help people achieve important person-centered goals like communication, independent living, and avoiding self-injury, therefore, the neurodiversity movement rejects the idea that service provision or research should promote typical behavior, like eye contact or standard movement and speech patterns. -
Understanding Autism
1 Understanding Autism Autism is a way of being. It is pervasive; it colors every experience, every sensation, perception, thought, emotion, and encounter, every aspect of existence. It is not possible to separate the autism from the person. Jim Sinclair (1993) ur first chapter will focus on understanding autism spectrum disor- O der (ASD) for one simple reason: Informed support leads to better outcomes. Although topics related to autism are frequently in the news, the disorder is not widely understood. Many people still perceive indi- viduals with autism based on movie depictions like Rain Man, Forrest Gump, Mozart and the Whale, and Adam. Although there is some truth to these depictions, each is really just a portrayal of one individual. To com- plicate matters, a student with autism may show little evidence of a dis- ability. The student is not using a brace or walking with a guide dog. He appears typical, with no physical evidence of a challenge. Despite outward appearances, the diagnosis leaves the student disconnected from others while distorting his perceptions of the world in which he lives. There is less tolerance in schools and society in general for disabilities that are hidden. It’s much harder for students and adults to understand differences they can’t see. The student with ASD senses things differently than his typical peers and may respond in unusual ways. As a result, the student is frequently misunderstood. Misunderstandings can lead to mistreatment, exclusion, and perhaps even abuse. Understanding 5 6 TEACHING ADOLESCENTS WITH AUTISM the range of potential characteristics of this disorder will empower you to be an effective advocate and teacher. -

Autistic Adult and Non-Autistic Parent Advocates: Bridging the Divide
AUTHORS' VERSION Rottier, H. & Gernsbacher, M. A. (2020). Autistic adult and non-autistic parent advocates: Bridging the divide. In. A. C. Carey, J. M., Ostrove, & T. Fannon (Eds.) Disability alliances and allies (Research in social science and disability, Vol. 12, pp. 155-166). Emerald Publishing Limited. https://doi.org/10.1108/S1479-354720200000012011 Chapter 7 AUTISTIC ADULT AND NON-AUTISTIC PARENT ADVOCATES: BRIDGING THE DIVIDE Helen Rottier and Morton Ann Gernsbacher ABSTRACT Purpose: Due to the developmental nature of autism, which is often diagnosed in preschool or elementary school-aged children, non-autistic parents of autistic children typically play a prominent role in autism advocacy. How- ever, as autistic children become adults and adult diagnoses of autism continue to rise, autistic adults have played a more prominent role in advo- cacy. The purpose of this chapter is to explore the histories of adult and non-autistic parent advocacy in the United States and to examine the points of divergence and convergence. Approach: Because of their different perspectives and experiences, advocacy by autistic adults and non-autistic parents can have distinctive goals and conflicting priorities. Therefore, the approach we take in the current chapter is a collaboration between an autistic adult and a non-autistic parent, both of whom are research scholars. Findings: The authors explore the divergence of goals and discourse between autistic self-advocates and non-autistic parent advocates and offer three principles for building future -

Neurodiversity 10Th Annual Nurturing Developing Minds Conference
Neurodiversity 10th Annual Nurturing Developing Minds Conference Manuel F. Casanova, M.D. SmartState Endowed Chair in Childhood Neurotherapeutics University of South Carolina Greenville Health System Conflict of Interests Neuronetics (TMS platform), Neuronetrix Incorporated, Clearly Present Foundation Pfizer, Eisai, Nycomed Amersham, Aventis Pasteur Limited, Medvantis Medical Service Council of Health Care Advisors for the Gerson Lehrman Goup Royalties: Springer, Nova, Taylor and Francis, John Wiley I am a physician who deals with individuals with neurodevelopmental disabilities and have a grandson with autism. Neurodiversity “A new wave of activists wants to celebrate atypical brain function as a positive identity, not a disability.” New York News and Politics “…neurological (brain wiring) differences, traditionally seen as disadvantages, are really advantages.” Fox and Hounds “What is autism: a devastating developmental disorder, a lifelong disability, or a naturally occurring form of cognitive difference akin to certain forms of genius?” SUPOZA.COM NEURODIVERSITY AND AUTISTIC PRIDE Individual with autism vs. Autistic Individual Control subject vs. Typically developing(TD) subject What message are you sending??? “Why is it that what makes me me, needs to be classified as a disability?” A child under 18 will be considered disabled if he or she has a medically determinable physical or mental impairment or combination of impairments that cause marked and severe functional limitations, that can be expected to cause death or that has lasted or can be expected to last for a continuous period of not less than 12 months. Normal variation in the human genome A social category rather than a medical disorder Includes autism, bipolar disorders, and other neurotypes It does not need to be cured ABA is specially pernicioius. -
Double Empathy, Explained
Spectrum | Autism Research News https://www.spectrumnews.org NEWS Double empathy, explained BY RACHEL ZAMZOW 22 JULY 2021 Listen to this story: Difficulty navigating social interactions pervades even the earliest accounts of autism. This defining trait of the condition has informed prevailing theories of its roots as well as the design of many autism treatments. But an emerging line of work supports a more nuanced look at the social abilities of autistic people. Proponents of an idea called the ‘double empathy problem’ believe that communication breakdowns between autistic and non-autistic people are a two-way issue, caused by both parties’ difficulties in understanding. This ‘double problem’ challenges long-held theories of autism that point to social shortcomings of people with autism as the reason interactions flop. It also echoes principles of neurodiversity in its assumption that autistic people simply have a different way of communicating rather than a deficient one. “As a theory, it matches autistic phenomenology coming from insider accounts,” says autistic researcher Damian Milton, lecturer in developmental and intellectual disabilities at the University of Kent in the United Kingdom. Although scientific support for the theory is building, it is not yet rock solid. And not all researchers are tuned in to this new direction, says Matthew Lerner, associate professor of psychology, psychiatry and pediatrics at Stony Brook University in New York. “The double empathy problem is a younger theory empirically,” he says. What is the double empathy problem? The basis of the theory is that a mismatch between two people can lead to faulty communication. This disconnect can occur at many levels, from conversation styles to how people see the world. -
Rethinking Autism, Communication, and Community
Portland State University PDXScholar Dissertations and Theses Dissertations and Theses Winter 3-31-2015 Rethinking Autism, Communication, and Community Involvement: Exploring Involvement in Online Communities, Communication Preference, Autistic Identity, and Self-Determination Colleen Anne Kidney Portland State University Follow this and additional works at: https://pdxscholar.library.pdx.edu/open_access_etds Part of the Psychology Commons Let us know how access to this document benefits ou.y Recommended Citation Kidney, Colleen Anne, "Rethinking Autism, Communication, and Community Involvement: Exploring Involvement in Online Communities, Communication Preference, Autistic Identity, and Self-Determination" (2015). Dissertations and Theses. Paper 2224. https://doi.org/10.15760/etd.2221 This Dissertation is brought to you for free and open access. It has been accepted for inclusion in Dissertations and Theses by an authorized administrator of PDXScholar. Please contact us if we can make this document more accessible: [email protected]. Rethinking Autism, Communication, and Community Involvement: Exploring Involvement in Online Communities, Communication Preference, Autistic Identity, and Self-Determination by Colleen Anne Kidney A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Applied Psychology Dissertation Committee: Eric Mankowski, Chair Katherine E. McDonald Greg Townley Christina Nicolaidis Laurie Powers Portland State University 2015 i Abstract Autistic individuals experience marginalization and stigmatization, and are often not connected to mainstream services or organizations fostering peer relationships (Boundy, 2008; Jaarsma & Welin, 2012; Robertson, 2010). Therefore, the accomplishments of the online Autistic community in building a community for self- advocacy, peer-support, friendships, and identity development (Brownlow & O’Dell, 2006; Kidney, 2012) are important to recognize, empirically examine, and promote (Blume, 1997a; Davidson, 2008). -
Finding Strengths in Autism
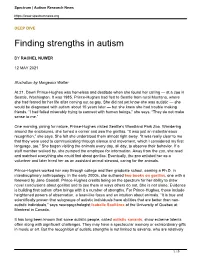
Spectrum | Autism Research News https://www.spectrumnews.org DEEP DIVE Finding strengths in autism BY RACHEL NUWER 12 MAY 2021 Illustration by Margeaux Walter At 21, Dawn Prince-Hughes was homeless and destitute when she found her calling — at a zoo in Seattle, Washington. It was 1985. Prince-Hughes had fled to Seattle from rural Montana, where she had feared for her life after coming out as gay. She did not yet know she was autistic — she would be diagnosed with autism about 15 years later — but she knew she had trouble making friends. “I had failed miserably trying to connect with human beings,” she says. “They do not make sense to me.” One morning, pining for nature, Prince-Hughes visited Seattle’s Woodland Park Zoo. Wandering around the enclosures, she turned a corner and saw the gorillas. “It was just an instantaneous recognition,” she says. She felt she understood them almost right away. “It was really clear to me that they were used to communicating through silence and movement, which I considered my first language, too.” She began visiting the animals every day, all day, to observe their behavior. If a staff member walked by, she pumped the employee for information. Away from the zoo, she read and watched everything she could find about gorillas. Eventually, the zoo enlisted her as a volunteer and later hired her as an assistant animal steward, caring for the animals. Prince-Hughes worked her way through college and then graduate school, earning a Ph.D. in interdisciplinary anthropology. In the early 2000s, she authored two books on gorillas, one with a foreword by Jane Goodall. -

2015-Kenny-Terms-To
AUT0010.1177/1362361315588200AutismKenny et al. 588200research-article2015 Original Article Autism 1 –21 Which terms should be used to describe © The Author(s) 2015 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav autism? Perspectives from the UK DOI: 10.1177/1362361315588200 autism community aut.sagepub.com Lorcan Kenny1, Caroline Hattersley2,3, Bonnie Molins2, Carole Buckley4, Carol Povey2 and Elizabeth Pellicano1,5 Abstract Recent public discussions suggest that there is much disagreement about the way autism is and should be described. This study sought to elicit the views and preferences of UK autism community members – autistic people, parents and their broader support network – about the terms they use to describe autism. In all, 3470 UK residents responded to an online survey on their preferred ways of describing autism and their rationale for such preferences. The results clearly show that people use many terms to describe autism. The most highly endorsed terms were ‘autism’ and ‘on the autism spectrum’, and to a lesser extent, ‘autism spectrum disorder’, for which there was consensus across community groups. The groups disagreed, however, on the use of several terms. The term ‘autistic’ was endorsed by a large percentage of autistic adults, family members/friends and parents but by considerably fewer professionals; ‘person with autism’ was endorsed by almost half of professionals but by fewer autistic adults and parents. Qualitative analysis of an open- ended question revealed the reasons underlying respondents’ preferences. These findings demonstrate that there is no single way of describing autism that is universally accepted and preferred by the UK’s autism community and that some disagreements appear deeply entrenched. -

The Autism Binary: Finding the Cause and Cure
THE AUTISM BINARY: FINDING THE CAUSE AND CURE/ ACCEPTING AND HELPING THE AFFECTED POPULATION – MAKING THE CASE FOR NEURODIVERSITY By STEVEN WALKER A capstone submitted to the Graduate School-Camden Rutgers, The State University of New Jersey In partial fulfillment of the requirements For the degree of Master of Arts Graduate Program in Liberal Studies Written under the direction of Professor Timothy Pure And approved by _____________________ Professor Timothy Pure Camden, New Jersey May 2017 CAPSTONE ABSTRACT The Autism Binary: Finding the Cause and Cure/Accepting and Helping the Affected Population – Making the Case for Neurodiversity by STEVEN WALKER Capstone Director: Professor Timothy Pure According to the CDC (Centers for Disease Control and Prevention), the probability of a child being diagnosed with some form of Autism Spectrum Disorder is 1 in 68. Autism is nondiscriminatory, for it can arise in any family at any time. In light of these facts, the Autistic community has become a veritable part of the western world. Subsequently, a continuing debate exists on whether to find the cause and possible cure for the condition, or to pursue the Neurodiversity movement, which is to accept Autism as a brain variation – not a disability. As an Autistic individual, I concur with the latter motive, for an immeasurable amount of neurotypicals are obsessed with the former idea. In addition, neurotypicals make endless attempts to ‘normalize’ the Autistic populace without their consent whatsoever. Well, what exactly is the true definition of ‘normal?’ Normal is a relative descriptor after all. Therefore, in this paper I will argue in favor of the Neurodiversity movement, for I am a proponent of its core message. -
Transcript of the December 14, 2010 IACC Meeting
1 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES INTERAGENCY AUTISM COORDINATING COMMITTEE FULL COMMITTEE MEETING TUESDAY, DECEMBER 14, 2010 The Committee met in The Grand Ballroom, Salons A-D, of the Pooks Hill Marriott, 5151 Pooks Hill Road, Bethesda, Maryland at 10:00 a.m., Thomas Insel, Chair, presiding. PARTICIPANTS: THOMAS INSEL, M.D., Chair, National Institute of Mental Health (NIMH) DELLA HANN, Ph.D., Executive Secretary, Office of Autism Research Coordination (OARC), National Institute of Mental Health (NIMH) SUSAN DANIELS, Ph.D., Office of Autism Research Coordination (OARC), National Institute of Mental Health (NIMH) JAMES BATTEY, M.D., Ph.D., National Institute on Deafness and Other Communication Disorders (NIDCD) ELLEN BLACKWELL, M.S.W., Centers for Medicare & Medicaid Services (CMS) COLEEN BOYLE, Ph.D., Centers for Disease Control and Prevention (CDC) NEAL R. GROSS COURT REPORTERS AND TRANSCRIBERS 1323 RHODE ISLAND AVE., N.W. (202) 234-4433 WASHINGTON, D.C. 20005-3701 www.nealrgross.com 2 PARTICIPANTS (continued): JOSEPHINE BRIGGS, M.D., National Center for Complementary and Alternative Medicine (NCCAM) (representing Francis Collins, M.D., Ph.D.) HENRY CLAYPOOL, U.S. Department of Health and Human Services (DHHS), Office on Disability (attended by phone) JUDITH COOPER, Ph.D., National Institute on Deafness and other Communication Disorders (NIDCD)(representing James Battey, M.D., Ph.D.) GERALDINE DAWSON, Ph.D., Autism Speaks GERALD FISCHBACH, M.D., Simons Foundation LEE GROSSMAN, Autism Society (attended by phone) ALAN GUTTMACHER, M.D., Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) GAIL HOULE, Ph.D., U.S. Department of Education WALTER KOROSHETZ, M.D., National Institute of Neurological Disorders and Stroke (NINDS) CINDY LAWLER, Ph.D., National Institute of Environmental Health Sciences (NIEHS) (representing Linda Birnbaum, Ph.D.) SHARON LEWIS, Administration for Children and Families (ACF) CHRISTINE MCKEE, J.D.