10. Okeke Et Al
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

Research Report
1.1 CHAPTER 1 INTRODUCTION Soil erosion is the systematic removal of soil, including plant nutrients, from the land surface by various agents of denudation (Ofomata, 1985). Water being the dominant agent of denudation initiates erosion by rain splash impact, drag and tractive force acting on individual particles of the surface soil. These are consequently transported seizing slope advantage for deposition elsewhere. Soil erosion is generally created by initial incision into the subsurface by concentrated runoff water along lines or zones of weakness such as tension and desiccation fractures. As these deepen, the sides give in or slide with the erosion of the side walls forming gullies. During the Stone Age, soil erosion was counted as a blessing because it unearths valuable treasures which lie hidden below the earth strata like gold, diamond and archaeological remains. Today, soil erosion has become an endemic global problem, In the South eastern Nigeria, mostly in Anambra State, it is an age long one that has attained a catastrophic dimension. This environmental hazard, because of the striking imprints on the landscape, has sparked off serious attention of researchers and government organisations for sometime now. Grove(1951); Carter(1958); Floyd(1965); Ofomata (1964,1965,1967,1973,and 1981); all made significant and refreshing contributions on the processes and measures to combat soil erosion. Gully Erosion is however the prominent feature in the landscape of Anambra State. The topography of the area as well as the nature of the soil contributes to speedy formation and spreading of gullies in the area (Ofomata, 2000);. 1.2 Erosion Types There are various types of erosion which occur these include Soil Erosion Rill Erosion Gully Erosion Sheet Erosion 1.2.1 Soil Erosion: This has been occurring for some 450 million years, since the first land plants formed the first soil. -

Assessing Hypoendemic Onchocerciasis in Loa Loa Endemic Areas of Southeast Nigeria
Am. J. Trop. Med. Hyg., 103(6), 2020, pp. 2328–2335 doi:10.4269/ajtmh.20-0368 Copyright © 2020 by The American Society of Tropical Medicine and Hygiene Assessing Hypoendemic Onchocerciasis in Loa loa Endemic Areas of Southeast Nigeria Lindsay J. Rakers,1* Emmanuel Emukah,2 Barminas Kahansim,3 Bertram E. B. Nwoke,4 Emmanuel S. Miri,3 Emily Griswold,1 Emmanuel Davies,5 Cephas Ityonzughul,3 Chukwuma Anyaike,5 Perpetual Agbi,5 and Frank O. Richards1 1The Carter Center, Atlanta, Georgia; 2The Carter Center, Owerri, Nigeria; 3The Carter Center, Jos, Nigeria; 4Parasitology Department, Imo State University, Owerri, Nigeria; 5Federal Ministry of Health, Abuja, Nigeria Abstract. Nigeria changed its goal for onchocerciasis from control to transmission elimination. Under the control program, ivermectin mass drug administration (MDA) focused only on hyper/meso-endemic local government areas (LGAs) identified by Rapid Epidemiological Mapping of Onchocerciasis as having ³ 20% nodule rates. Because trans- mission is likely in some LGAs where nodule rates are < 20%, the new elimination paradigm requires MDA expansion. Determining which hypoendemic areas require MDA, termed onchocerciasis elimination mapping, is a major challenge. In 2016, we studied 19 ivermectin-naive hypoendemic LGAs in southern Nigeria that bordered LGAs under MDA. Fifty adults and 50 children (aged 5–10 years) were tested in 110 villages for onchocerciasis IgG4 antibody using an Ov16 rapid diagnostic test (RDT). A 10% subset of subjects provided a blood spot for confirmatory Ov16 ELISA. The mean prevalence of RDT positives was 0.5% in the 5,276 children tested (village range, 0.0–4.0%) versus 3.3% in 5,302 adults (village range, 0.0–58.0%). -

Household Water Demand in the Peri-Urban Communities of Awka, Capital of Anambra State, Nigeria
Vol. 6(6), pp. 237-243, August, 2013 DOI: 10.5897/JGRP2013.0385 Journal of Geography and Regional Planning ISSN 2070-1845 © 2013 Academic Journals http://www.academicjournals.org/JGRP Full Length Research Paper Household water demand in the peri-urban communities of Awka, Capital of Anambra State, Nigeria E. E. Ezenwaji1*, P.O. Phil-Eze2, V. I. Otti3 and B. M. Eduputa4 1Department of Geography and Meteorology, Nnamdi Azikiwe University, Awka, Nigeria. 2Department of Geography, University of Nigeria, Nsukka, Nigeria. 3Civil Engineering Department, Federal Polytechnic, Oko, Nigeria. 4Department of Environmental Management, Nnamdi Azikiwe University, Awka, Nigeria. Accepted 22 July, 2013 The aim of this paper is to determine relevant factors contributing to the water demand in the peri-urban communities of Awka capital city. Towards achieving this aim, questionnaire were developed and served on the households in various communities to collect relevant data on the 13 physical and socio- economic factors we earlier identified as influencing water demand in the area. Water quality was ascertained through microbiological analysis of water samples. The major analytical techniques used were multiple correlations, the result of which was subjected to Principal Component Analysis (PCA) and Principal Component Regression. Result shows that the 13 variables combined to contribute 90.0% of water demand in the area. Furthermore, the low standard error of estimates of 0.029 litres shows that water demand in the communities could be predicted using the 13 variables. Policy and planning measures to improve the water supply situation of the area were suggested. Key words: Capital, communities, factors, peri-urban, water demand. -

A Case Study of Awka and Onitsha in Anambra State, Nigeria
Journal of Law, Policy and Globalization www.iiste.org ISSN 2224-3240 (Paper) ISSN 2224-3259 (Online) Vol.19, 2013 Urban Flooding and Vulnerability of Nigerian Cities: A Case Study of Awka and Onitsha in Anambra State, Nigeria Kingsley Efobi * Christopher Anierobi Department of Urban and Regional Planning, University of Nigeria, Enugu campus PMB 01129,Nigeria * E-mail of the corresponding author: [email protected] ABSTRACT The climate change phenomenon with its associated increase in global temperature, precipitation and rise in sea levels has also ushered in an increased frequency of flooding in recent times. In the year 2012, many Nigerian cities suffered from the ravaging effects of flooding. This led to lose of lives, internal displacements, destruction of properties, disruption of socio-economic, cultural and religious activities; and splintering of family ties. The cities of Awka and Onitsha in Anambra state, Nigeria featured among the vulnerable cities which are susceptible to flooding. This study set out to find out the causes of flooding in these cities with a view to recommending measures that will help ameliorate the situation. Direct observations and structured interview methods were used to acquire the needed primary data from residents of identified flood prone areas and in addition to secondary data obtained from official records of the State Ministry of Environment. The result revealed that although flooding gives the residents of Awka and Onitsha nightmares, especially during the rainy seasons; it had received only 15% of government intervention activities on environmental problems. There is gross inadequacy in the provision of drainage channels, coupled with poor designs, poor construction and blocked drainage channels. -

STRUCTURE PLAN for Awka and SATELLITE TOWNS
AWKA STRUCTURE PLAN FOR AWKA AND SATELLITE TOWNS Anambra State STRUCTURE PLAN FOR AWKA AND SATELLITE TOWNS Anambra State 1 Structure Plan for Awka and Satellite Towns Copyright © United Nations Human Settlements Programme (UN-HABITAT), 2009 All rights reserved United Nations Human Settlements Programme publications can be obtained from UN-HABITAT Regional and Information Offices or directly from: P.O.Box 30030, GPO 00100 Nairobi, Kenya. Fax: + (254 20) 762 4266/7 E-mail: [email protected] Website: http://www.unhabitat.org HS/1152/09E ISBN: 978-92-1-132118-0 DISCLAIMER The designation employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning delimitation of its frontiers or boundaries, or regarding its economic system or degree of development. The analysis, conclusions and recommendations of the report do not necessarily reflect the views of the United Nations Human Settlements Programme (UN-HABITAT), the Governing Council of UN-HABITAT or its Member States. Excerpts from this publication may be reproduced without authorisation, on condition that the source is indicated. Photo Credits : © UN-HABITAT acknowLEDGEMents Director: Dr Alioune Badiane Principal Editor: Prof. Johnson Bade Falade Co-ordinator: Dr. Don Okpala Principal Authors: Prof. Louis C. Umeh Prof. Samson O. Fadare Dr. Carol Arinze –Umobi Chris Ikenna Udeaja Tpl. (Dr) Francis Onweluzo Design and Layout: Andrew Ondoo 2 FOREWORD t is now widely It is to reverse and stem this development trend acknowledged and to realize the developmental potentials of well- and accepted that planned and managed cities, towns and villages, that citiesI and urban areas my Government approached the United Nations are engines of economic Human Settlements Programme (UN-HABITAT) in development and growth. -

List of Coded Health Facilities in Anambra State.Pdf
Anambra State Health Facility Listing LGA WARD NAME OF HEALTH FACILITY FACILITY TYPE OWERSHIP CODE (PUBLIC/ PRIVATE) LGA STATE OWERSHIP FACILITYTYPE FACILITYNUMBER Primary Health Centre Oraeri Primary Public 04 01 1 1 0001 Primary Health Centre Akpo Primary Public 04 01 1 1 0002 Ebele Achina PHC Primary Public 04 01 1 1 0003 Primary Health Centre Aguata Primary Public 04 01 1 1 0004 Primary Health Centre Ozala Isuofia Primary Public 04 01 1 1 0005 Primary Health Centre Uga Primary Public 04 01 1 1 0006 Primary Health Centre Mkpologwu Primary Public 04 01 1 1 0007 Primary Health Centre Ikenga Primary Public 04 01 1 1 0008 Health Centre Ekwusigo Isuofia Primary Public 04 01 1 1 0009 Primary Health Centre Amihie Umuchu Primary Public 04 01 1 1 0010 Obimkpa Achina Health Centre Primary Public 04 01 1 1 0011 Primary Health Centre Amesi Primary Public 04 01 1 1 0012 Primary Health Centre Ezinifite Primary Public 04 01 1 1 0013 Primary Health Centre Ifite Igboukwu Primary Public 04 01 1 1 0014 Health Post Amesi Primary Public 04 01 1 1 0015 Isiaku Health Post Primary Public 04 01 1 1 0016 Analasi Uga Health Post Primary Public 04 01 1 1 0017 Ugwuakwu Umuchu Health Post Primary Public 04 01 1 1 0018 Aguluezechukwu Health Post Primary Public 04 01 1 1 0019 Health Centre Umuona Primary Public 04 01 1 1 0020 Health Post Akpo Primary Public 04 01 1 1 0021 Health Center, Awa Primary Public 04 01 1 1 0022 General Hospital Ekwuluobia Secondary Public 04 01 1 1 0023 General Hospital Umuchu Secondary Public 04 01 2 1 0024 Comprehensive Health Centre Achina Primary Public 04 01 1 1 0025 Catholic Visitation Hospital, Umuchu Secondary Private 04 01 2 2 0026 Continental Hospital Ekwulobia Primary Private 04 01 1 2 0027 Niger Hospital Igboukwu Primary Private 04 01 1 2 0028 Dr. -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -
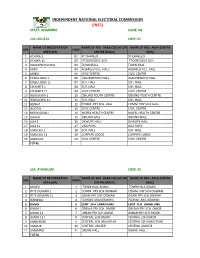
State: Anambra Code: 04
INDEPENDENT NATIONAL ELECTORAL COMMISSION (INEC) STATE: ANAMBRA CODE: 04 LGA :AGUATA CODE: 01 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA CENTRE S/N CODE AREA (RA) CENTRE (RACC) (RAC) 1 ACHINA 1 01 ST CHARLED ST CHARLED 2 ACHINA 11 02 PTOGRESSIVE SCH. PTOGRESSIVE SCH. 3 AGULEZECHUKWU 03 TOWN HALL TOWN HALL 4 AKPO 04 AGBAELU VILL. HALL AGBAELU VILL. HALL 5 AMESI 05 CIVIC CENTRE CIVIC CENTRE 6 EKWULOBIA 1 06 UMUEZENOFO HALL. UMUEZENOFO HALL. 7 EKWULOBIA 11 07 SCH. HALL SCH. HALL 8 EZENIFITE 1 08 SCH. HALL SCH. HALL 9 EZENIFITE 11 09 CIVIC CENTRE CIVIC CENTRE 10 IGBOUKWU 1 10 OBIUNO YOUTH CENTRE OBIUNO YOUTH CENTRE 11 IGBOUKWU 11 11 SCH. HALL SCH. HALL 12 IKENGA 12 COMM. PRY SCH. HALL COMM. PRY SCH. HALL 13 ISUOFIA 13 CIVIC CENTRE CIVIC CENTRE 14 NKPOLOGWU 14 MOFEL HEALTH CENTRE MOFEL HEALTH CENTRE 15 ORAERI 15 OBIUNO HALL OBIUNO HALL 16 UGA 1 16 OKWUTE HALL OKWUTE HALL 17 UGA 11 17 UGA BOYS UGA BOYS 18 UMUCHU 1 18 SCH. HALL SCH. HALL 19 UMUCHU 11 19 CORPERS LODGE CORPERS LODGE 20 UMOUNA 20 CIVIC CENTRE CIVIC CENTRE TOTAL LGA: AYAMELUM CODE: 02 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA CENTRE S/N CODE AREA (RA) CENTRE (RACC) (RAC) 1 ANAKU 1 TOWN HALL ANAKU TOWN HALL ANAKU 2 IFITE OGWARI 1 2 COMM. PRY SCH.OGWARI COMM. PRY SCH.OGWARI 3 IFITE OGWARI 11 3 OGARI PRY SCH.OGWARI OGARI PRY SCH.OGWARI 4 IGBAKWU 4 ISIOKWE ARA,IGBAKWU ISIOKWE ARA,IGBAKWU 5 OMASI 5 CENT. -

Modelling for the Effectiveness of Lower
JOURNAL OF ENGINEERING AND Journal of Engineering and Applied Sciences 10 (2014), 19-29 APPLIED SCIENCES Surface water quality degradation in Anambra State, South Eastern Nigeria B.U. Okoro* and +N.E Nwaiwu** Department of Civil Engineering, Nnamdi Azikiwe University, Awka, Anambra, * Email: [email protected] (+23408025163719) **Email: [email protected] (+23408025528200) Abstract The study was undertaken to assess the water quality in selected rivers and lake in Anambra State, South Eastern Nigeria. A total of six surface water sources selected(including Rivers Niger,Eziche,Omambala,Obibia,Okpuno stream and Agulu Lake) were from five Local Government Areas in the State, viz.: Onitsha South, Anambra East, Anaocha, Awka North and Awka South. All the samples were analyzed for parameters which include temperature, total dissolved solids (TDS), pH and six heavy metals, viz., As, Cd, Cu, Fe, Pb, and Zn using standard procedures. The results were compared with present National and International (World Health Organisation WHO) standard, the Nigerian Standard for Drinking Water Quality NSDWQ (2007). Among the analyzed samples, all samples contained Zinc and Copper within the NSDWQ (2007), although no guideline is set by WHO (2011) for Zinc level in drinking water. Cadmium , Arsenic , Iron and Lead were above the maximum admissible and desirable limits recommended by NSDWQ (2007) and WHO (2011). Microbiological parameters, viz., total coliform, fecal coliform and the total aerobic heterotrophic bacterial count, were all above the maximum admissible and desirable limits recommended by NSDWQ (2007) and WHO (2011) for all the surface water sources selected. This is an indication of pollution hazards in the study areas, which in turn have important human health implications. -

City Structure Plans for Onitsha, Nnewi & Awka
EXECUTIVE SUMMARY OF STRUCTURE PLANS FOR AWKA, ONITSHA AND NNEWI AND ENVIRONS 2009-2027 Anambra State EXECUTIVE SUMMARY OF STRUCTURE PLANS FOR AWKA, ONITSHA AND NNEWI AND ENVIRONS 2009-2027 Anambra State 1 Executive Summary of Structure Plans for Awka, Onitsha and Nnewi and Environs 2009-2027 Copyright © United Nations Human Settlements Programme (UN-HABITAT), 2009 All rights reserved United Nations Human Settlements Programme publications can be obtained from UN-HABITAT Regional and Information Offices or directly from: P.O.Box 30030, GPO 00100 Nairobi, Kenya. Fax: + (254 20) 762 4266/7 E-mail: [email protected] Website: http://www.unhabitat.org HS: HS/1153/09E ISBN: 978-92-1-132119-7 DISCLAIMER The designation employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning delimitation of its frontiers or boundaries, or regarding its economic system or degree of development. The analysis, conclusions and recommendations of the report do not necessarily reflect the views of the United Nations Human Settlements Programme (UN-HABITAT), the Governing Council of UN-HABITAT or its Member States. Excerpts from this publication may be reproduced without authorisation, on condition that the source is indicated. Photo Credits : © UN-HABITAT acknowLEDGEMents Director: Dr Alioune Badiane Principal Editor: Prof. Johnson Bade Falade Co-ordinator: Dr. Don Okpala Principal Authors: Dr Francis Onweluzo Tpl. Joachim, A. C. Okafor Engr Felix Nnamdi Nwokedi M Mrs. -

(ESMP) for the Amachalla Gully Erosion Site
Nigeria Erosion and Watershed Management Project (NEWMAP) Draft Report Public Disclosure Authorized Environmental and Social Management Plan (ESMP) for the Amachalla Gully Erosion Site Awka South, Anambra State. Public Disclosure Authorized Public Disclosure Authorized [Document title] [Document subtitle] Abstract [Draw your reader in with an engaging abstract. It is typically a short summary of the document. When you’re ready to add your content, just click here and start typing.] Public Disclosure Authorized Prepared for the State Project Management Unit (SPMU) Anambra State Nigeria Erosion and Watershed Management Project [Email address] Draft Report for the Amachalla gully erosion site Nigeria Erosion and Watershed Management Project (NEWMAP) Draft Report Environmental and Social Management (ESMP) for the Amachalla Gully Erosion Site Awka, Anambra State Prepared for the State Project Management Unit (SPMU) Anambra State Nigeria Erosion and Watershed Management Project ii Draft Report for the Amachalla gully erosion site Table of Contents LIST OF FIGURES ..................................................................................................................................... IV LIST OF PHOTOS ...................................................................................................................................... V LIST OF TABLES ....................................................................................................................................... V EXECUTIVE SUMMARY ..............................................................................................................