Uganda's APAC District
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Contract Farming, Smallholders and Commercialization of Agriculture in Uganda: the Case of Sorghum, Sunflower, and Rice Contract Farming Schemes
Center of Evaluation for Global Action Working Paper Series Agriculture for Development Paper No. AfD-0907 Issued in July 2009 Contract Farming, Smallholders and Commercialization of Agriculture in Uganda: The Case of Sorghum, Sunflower, and Rice Contract Farming Schemes. Gabriel Elepu Imelda Nalukenge Makerere University This paper is posted at the eScholarship Repository, University of California. http://repositories.cdlib.org/cega/afd Copyright © 2009 by the author(s). Series Description: The CEGA AfD Working Paper series contains papers presented at the May 2009 Conference on “Agriculture for Development in Sub-Saharan Africa,” sponsored jointly by the African Economic Research Consortium (AERC) and CEGA. Recommended Citation: Elepu, Gabriel and Nalukenge, Imelda. (2009) Contract Farming, Smallholders and Commercialization of Agriculture in Uganda: The Case of Sorghum, Sunflower, and Rice Contract Farming Schemes. CEGA Working Paper Series No. AfD-0907. Center of Evaluation for Global Action. University of California, Berkeley. Contract Farming, Smallholders and Commercialization of Agriculture in Uganda: The Case of Sorghum, Sunflower, and Rice Contract Farming Schemes. Gabriel Elepu1∗ and Imelda Nalukenge2 1Lecturer in the Department of Agricultural Economics and Agribusiness, Makerere University, Kampala. 2Lecturer (Deceased) in the Department of Agricultural Economics and Agribusiness, Makerere University, Kampala. ABSTRACT: Contract farming has expanded in Uganda due to the promotional efforts of various actors: private, public, and/or international aid agencies. While motives for promoting contract farming may vary by actor, it is argued in this study that contract farming is crucial in the commercialization of smallholder agriculture and hence, poverty reduction in Uganda. However, smallholder farmers in Uganda have reportedly experienced some contractual problems when dealing with large agribusiness firms, resulting in them giving up contract farming. -

WHO UGANDA BULLETIN February 2016 Ehealth MONTHLY BULLETIN
WHO UGANDA BULLETIN February 2016 eHEALTH MONTHLY BULLETIN Welcome to this 1st issue of the eHealth Bulletin, a production 2015 of the WHO Country Office. Disease October November December This monthly bulletin is intended to bridge the gap between the Cholera existing weekly and quarterly bulletins; focus on a one or two disease/event that featured prominently in a given month; pro- Typhoid fever mote data utilization and information sharing. Malaria This issue focuses on cholera, typhoid and malaria during the Source: Health Facility Outpatient Monthly Reports, Month of December 2015. Completeness of monthly reporting DHIS2, MoH for December 2015 was above 90% across all the four regions. Typhoid fever Distribution of Typhoid Fever During the month of December 2015, typhoid cases were reported by nearly all districts. Central region reported the highest number, with Kampala, Wakiso, Mubende and Luweero contributing to the bulk of these numbers. In the north, high numbers were reported by Gulu, Arua and Koti- do. Cholera Outbreaks of cholera were also reported by several districts, across the country. 1 Visit our website www.whouganda.org and follow us on World Health Organization, Uganda @WHOUganda WHO UGANDA eHEALTH BULLETIN February 2016 Typhoid District Cholera Kisoro District 12 Fever Kitgum District 4 169 Abim District 43 Koboko District 26 Adjumani District 5 Kole District Agago District 26 85 Kotido District 347 Alebtong District 1 Kumi District 6 502 Amolatar District 58 Kween District 45 Amudat District 11 Kyankwanzi District -
Implementation Status & Results
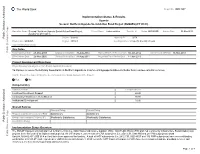
The World Bank Report No: ISR13907 Implementation Status & Results Uganda Second Northern Uganda Social Action Fund Project (NUSAF2) (P111633) Operation Name: Second Northern Uganda Social Action Fund Project Project Stage: Implementation Seq.No: 8 Status: ARCHIVED Archive Date: 03-May-2014 (NUSAF2) (P111633) Public Disclosure Authorized Country: Uganda Approval FY: 2009 Product Line:IBRD/IDA Region: AFRICA Lending Instrument: Specific Investment Loan Implementing Agency(ies): Key Dates Public Disclosure Copy Board Approval Date 28-May-2009 Original Closing Date 31-Aug-2014 Planned Mid Term Review Date 30-Jan-2012 Last Archived ISR Date 19-Nov-2013 Effectiveness Date 25-Nov-2009 Revised Closing Date 31-Aug-2014 Actual Mid Term Review Date 14-Jun-2013 Project Development Objectives Project Development Objective (from Project Appraisal Document) To improve access of beneficiary households in Northern Uganda to income earning opportunities and better basic socio-economic services. Has the Project Development Objective been changed since Board Approval of the Project? Yes No Public Disclosure Authorized Component(s) Component Name Component Cost Livelihood Investment Support 60.00 Community Infrastructure Rehabilitation 30.00 Institutional Development 10.00 Overall Ratings Previous Rating Current Rating Progress towards achievement of PDO Satisfactory Satisfactory Overall Implementation Progress (IP) Moderately Satisfactory Moderately Satisfactory Public Disclosure Authorized Overall Risk Rating Implementation Status Overview The NUSAF II project originally planned to finance 9750 (i.e. 8000 Household Income Support (HIS), 1000 Public Works (PW) and 750 Community Infrastructure Rehabilitation) sub projects in the five year of its implementation period. As of February 3, 2013 a total of 8,764 subprojects (i.e. -
Monthly Programme Update
EMERGENCY AND HUMANITARIAN ACTION, UGANDA APRIL 200 9 Monthly Programme Update Highlights ♦ Under surge capacity organised by IST/AFRO, supported cholera control in Zimbabwe and VHF training in Zambia. ♦ Continued supporting the second round of Polio supplemental immunization activities continued in northern Uganda, Karamoja and Kamapla with an achievement of over 100 % coverage ♦ Continued supporting Hepatitis E epidemic in Kitgum district ♦ Support to Dokolo district in sleeping sickness control 1. General Situation: Political, Social and Security ♦ Security situation in northern Ugandan districts continued being stable ♦ In Karamoja the security situation remained stable on the roads although raids and other criminal activities continue to be reported in many places of the region. ♦ Disarmament initiated by the government in Karamoja is ongoing 2. Programme Implementation a. Activities Emergency Health, Nutrition and HIV/AIDS Response Project (Sida) In Kitgum District the programme; ♦ Continued to provide technical support towards Hepatitis E interventions to support/ guide sub- county activities including supervision A who staff assists health workers arrange vaccines used for the 2nd round of mass Polio campaigns. of VHTs to enhance community mobilization and public health education. ♦ Finicailly supported VHTs and CBDs with incentives to enable them perform health education/promotion and inspection, establishing completed latrines and tracing for Hepatitis E patients. ♦ Techinically and logistically supported the Polio supplemental immunization. In Gulu and Amuru ♦ Technically and logistically supported Gulu and Amuru districts with the 2nd round of mass Polio campaigns In Pader District, WHO/HAC ♦ Continued to technically support the district health team to coordinate, supervise and monitor Hepatitis E epidemic control interventions by organizing weekly coordination meetings. -

Emergency and Humanitarian Action (EHA), Uganda Weekly Activity Report
Emergency and Humanitarian Action (EHA), Uganda Weekly Activity Report I. General Situation a. Political, Social and Security; • DRC; Joint incursion on LRA base in Garamba by the armed forces from DRC, Sudan Week 11, and Uganda has ended. 1st bunch of Uganda soldiers have returned to Uganda. Report indicates that the incursion has succeeded in reducing the strength of LRA by 80%. • 9th to 15th March Acholi and Lango sub-region; the region is calm; population movement from IDP to 2009 village of origin is ongoing. • Karamoja sub-regio; Cattle raids by armed Karamojong worriers reported. The region is in security phase III. b. Main Events of Interest/Concern for Health • Mop up mass Polio immunization campaign was successfully conducted in Amuru district in epi-week 11 • Preparation for the first round of mass Polio immunization campaign is ongoing in 29 high risk districts in Uganda. II. Analysis and Health Consequences (Health Problems and Needs of Affected Population) Malaria: Lango; Lira district continues to report higher number of cases of clinical malaria in 2009 as compared to 2008. Apac district reports lower numbers of clinical malaria in 2009 as compared to 2008. See figure I below for details. Acholi, Kitgum and Pader districts continue to register low number of cases of clinical malaria in 2009 as compared to 2008. See figure II below. Highlights Polio immunization campaign was successfully conducted in Amuru district. Coverage of 150% was registered. Plans to conduct first round of Polio vaccination in 29 districts in Uganda from 23rd to 26th April is progressing well. Karamoja sub-regions; The number of cases of clinical malaria reported and the trend in 2009 is similar to that of 2008 for the same epi-week. -

Chapter 4 Hydrogeology CHAPTER 4 HYDROGEOLOGY
The Development study on water resources development and management for Lake Kyoga Basin Final Report -Supporting- Chapter 4 Hydrogeology CHAPTER 4 HYDROGEOLOGY 4.1 Collection of Existing Data Existing data about hydrogeology managed by Directorate of Water Resources Management (DWRM) are Groundwater Database, Mapping Project data, and Groundwater Monitoring data. Others are the MIS database which is water supply facilities database managed by Directorate of Water Development, including the items of location, water source, functionality, and so on. 4.1.1 National Groundwater Database (NGWDB) This database was established by DWRM with contracting to a local consultant in 2000. DWRM had been compiled database based on the “Borehole Completion Report” which is submitted by drilling company after completion of drilling. In 1990s, it was managed by database software on MS-DOS, and before 1990s, it was borehole ledger described on paper book. Now it was compiled by Microsoft Access database management software on the Windows base again. Figure 4-1 shows the initial display of the database. The database has been input the data based on the completion report submitted by drilling company every year. It is including the well specification, geological information, pumping test data, water quality test result, and so on. This database is very sophisticated. DWRM gave to the study team the Source: DWRM data which are related to the Lake Figure 4-1 Initial Display of National Groundwater Database Kyoga Basin. In the obtained data, the number of data which described the registered well number is 11,880, the number of data which described the well construction information is 9,672, the number of data which described the hydrogeological information is 5,902, the number of data which described the pump information is 1,095, and the number of data which described the water quality is 2,293. -

324868-Eng.Pdf
World Health Organization African Programme for Onchocerciasis Control .l Evaluation of the Sustainability of Phase IV CDTI Project August-September 2006 Coordinator of Phase IV Uganda CDTI: Prof. Oladele Akogun District Team members Page ADJUMANI O. Akosun. O. Ochiene. E. Masawe l5 APAC L. Matagi" D. Abdul, T. Mu.qa'yo 31 GULU A. Turinde, T. Abraraw, F. Byenume 46 KIBALE J. Musisha. S. Aeunvo. G. Pallansvo 61 MOYO N. Ene-Obon g. A.Begumisha,A. Byamungu,T. Lakwo 78 Secretariat: NOCP/Iv{oH : Andrew Byamungu, Peace Komukama, Zakia Mugaba, V/HO/APOC: Joseph Kajubi, DRAF'T REPORT 2 0 SEP. 7006 TABLE OF CONTENTS ABBREVIATIONS/ACRONYMS ACKNOWLEDGEMENT EXECUTIVE SUMMARY t THE \ryAY FORWARI) l.O INTRODUCTION 2.0 METHODOLOGY 13 2.1 Sampling 13 2.2 Sources of Information l5 2.3 Analysis 15 3.0 EVALUATION FINDINGS IN EACH DISTRICT t6 3.1 ADJUMAI\I t6 3.1.1 Sustainabiliÿ at the District Level 16 3.1.2 Sustainabiliÿ at the FLHF Level 2T 3.1.3 Sustainability at the Community Level 25 3.1.4 Conclusion and Grading the Overall Sustainability 29 3.2 APAC 32 3.2.1 Sustainability at the District Level 32 3.2.2 Sustainability at the FLHF Level 36 3.2.3 Sustainability at the Community Level 40 3.2.4 Conclusion and Grading the Overall Sustainability 44 3.3 GULU 47 3.3.1 Sustainability at the District Level 47 3.3.2 Sustainability at the FLHF Level 51 3.3.3 Sustainability at the Community Level 54 3.3.4 Conclusion and Grading the Overall Sustainability 59 3.4 KIBALE 63 3.4.1 Sustainability at the District Level 63 3.4.2 Sustainability at the FLHF Level 68 3.4.3 Sustainability at the Community Level 7l 3.4.4 Conclusion and Grading the Overall Sustainability 75 3.5 MOYO 78 3.5.1 Sustainability at the District Level 78 3.5.2 Sustainabiliÿ at the FLHF Level 83 3.5.3 Sustainabiliÿ at the Community Level 89 3.5.4 Conclusion and Grading the Overall Sustainability 93 4. -

National Internally Displaced Persons Return, Resettlement and Re-Integration Strategic Plan for Lango and Teso Sub Regions
NATIONAL INTERNALLY DISPLACED PERSONS RETURN, RESETTLEMENT AND RE-INTEGRATION STRATEGIC PLAN FOR LANGO AND TESO SUB REGIONS November 2005 Table of Contents Page Introduction Budget Summary ANNEX Component 1 Lira and Amolatar Districts IDP return plan Component 2 Apac District IDP Return Plan Component 3 Katakwi and Amuria Districts IDP Return plan Component 4 Soroti District IDP Return Plan Component 5 Kaberamaido District IDP Return Plan INTRODUCTION 1. Background Recent political and military developments in Northern Uganda have generated optimism for the IDP return process to begin. These include the Southern Sudan peace process, the renewed diplomatic relation between Sudan and Uganda, under which the latter is allowed to pursue the LRA rebels into the former’s territory (Operation Iron Fist II) and the efforts for peaceful agreement between LRA and government brokered by Mrs Betty Bigombe. From July 2004, there has been a marked improvement in the general security situation in the Northern Uganda Districts evidenced by the high rates of LRA desertions which is partly as a result of increased pressure from the UPDF supported by the auxiliary forces and the people, and also as a result of the government amnesty to insurgents who renounce war. In August 2004, Cabinet approved a National Policy for Internally Displaced Persons, which establishes principles for provision of assistance to IDPs while in the camps and procedures for their return and resettlement. In the policy, Government committed itself to ending the insurgency and facilitating the voluntary return, resettlement and re-integration of the IDPs. By October 2004, the LRA capacities to attack civilians became less frequent in Acholiland, and virtually ended in Teso and Lango sub regions except for some few isolated incursions that have been effectively contained. -

Uganda Weekly Activity Report
Emergency and Humanitarian Action (EHA), Uganda Weekly Activity Report I. General Situation a. Political, Social and Security; The UPDF military operation against LRA in Garamba forest is still ongoing. Week 4, However, the security situation in Acholi, Lango and Karamoja sub-region is calm. th th b. Main Events of Interest/Concern for Health 19 to 25 January Regional workshop on “STOP AVIAN INFLUENZA” conducted for districts 2009 in Lango and Acholi sub-region by the Ministry of Agriculture, Animal Industries and Fisheries (MAAIF). WHO, Dokolo DHT and officials from MoH Sleeping Sickness control Programme conducted a joint support supervision of intensified HAT control activities in Dokolo district WHO Lira sub-office conducted inventory of human resources for health and staff accommodation in Lango sub-region. Preliminary findings show that according to HSSP II norms, over 70% of health posts in 4 of the 5 districts are filled. Apac district coverage is the lowest at 67.5%. On average, only about 30% of the staff has staff accommodation. II. Analysis and Health Consequences (Health Problems and Needs of Affected Population) Malaria: Acholi, Lango and Karamoja sub-regions; The trend of malaria cases in all sub- regions in the last four weeks is similar to that of 2008 for the same epi-week. Figure I Highlights Capacity building for districts in Acholi and Lango sub-regions on Avian Influenza The epidemic outbreak of meningitis in Hoima, Masindi, Arua, Moyo Meningitis; The epidemic outbreak of Meningitis in the districts of Hoima, Masindi, and Adjumani has been Arua, Moyo and Adjumani has been contained. -
HIV and AIDS MAPPING
ANNEX 1: NGO, CBO, FBO & UN AGENCY INTERVENTIONS HIV and AIDS MAPPING HIV AND AIDS SERVICE PROVISION TO IDP COMMUNITIES IN NORTHERN UGANDA DISTRICTS OF GULU, AMURU, KITGUM, PADER, LIRA, OYAM, AND APAC SEPTEMBER – DECEMBER, 2006 Conducted by the International Organization for Migration In Collaboration with the Government of Uganda and UN Agencies As part of the Joint UN Inter-Agency Programme on Health, Nutrition, and HIV and AIDS Funded by the Department for International Development of the British Government ANNEX 1: HIV AND AIDS SERVICE PROVISION BY SERVICE PROVIDERS, AS PER SERVICE PROVIDERS Overview Service Provision by Geographical Location, ie; IDP location by district Acronyms and Abbreviations 4 HIV and AIDS service provision by service provider by IDP camp/settlement site, Gulu district 5 HIV and AIDS service provision by service provider by IDP camp/settlement site, Amuru district 8 HIV and AIDS service provision by service provider by IDP camp/settlement site, Kitgum district 10 HIV and AIDS service provision by service provider by IDP camp/settlement site, Pader district 13 HIV and AIDS service provision by service provider by IDP camp/settlement site, Lira district 17 HIV and AIDS service provision by service provider by IDP camp/settlement site, Oyam/Apac districts 20 Table: Number of beneficiaries of WFP & partner nutritional assistance by district 22 Table: Number of WFP & partners nutritional assistance to direct beneficiaries by category by district 22 Table: WFP implementing partners by category by district 22 Table: -

DISTRICT INVESTMENT PLAN for WATER SANITATION and HYGIENE Process, Outcomes and Emerging Issues
DISTRICT INVESTMENT PLAN FOR WATER SANITATION AND HYGIENE Process, outcomes and emerging issues Ministry of Water and Environment • KEY ISSUES Background every community; every clinic; every school; everyone, and forever. Provision of water and sanitation services The focus is on ensuring 100% access and • The DIP is a remains a priority to the Government of coverage for both water and sanitation in an projection of what is Uganda and its development partners. entire district (urban, peri-urban/rural growth required to achieve centres and rural). All aspects and factors that Apart from subscribing to the Sustainable ensure full coverage, such as: quality, quantity, 100% WASH coverage Development Goals (SDGs), the Government reduced distances between households and of Uganda in 2015 adopted its second in any given district. water sources, coordination of sector actors, National Development Plan (NDPII) which planning, costs and reliability of the services puts provision of water and sanitation services are given due consideration. • The DIP largely at the forefront of national development. relies on the Earlier in 2009, the Ministry of Water and The Government commits to increase water Environment developed a Strategic Sector quality of data. It is supply coverage in rural areas from 65 Investment Plan (SSIP), with the aim of guiding percent to 79 percent while ensuring that at important to work all future investments in the sector so as to least each village has a clean and safe water improve its fiscal and physical effectiveness with stakeholders like source; Increase urban water supply from 77 for the achievement of sector targets and percent to 95 percent (100 percent in NWSC UBOS to get reliable goals by 2035. -

Contributing to a Peace Economy in Northern Uganda: a Guide for Investors
Contributing to a Peace Economy in Northern Uganda: A Guide for Investors June 2009 Understanding conflict. Building peace About International Alert International Alert is an independent peacebuilding organisation that has worked for over 20 years to lay the foundations for lasting peace and security in communities affected by violent conflict. Our multifaceted approach focuses both in and across various regions; aiming to shape policies and practices that affect peacebuilding; and helping build skills and capacity through training. Our field work is based in Africa, South Asia, the South Caucasus, Latin America, Lebanon and the Philippines. Our thematic projects work at local, regional and international levels, focusing on cross-cutting issues critical to building sustainable peace. These include business and economy, gender, governance, aid, security and justice. We are one of the world’s leading peacebuilding NGOs with more than 120 staff based in London and our 11 field offices. Photo credits: K. Burns/ USAID Africa Bureau, IRIN photo unit and International Alert. Lay-out design: The Print House Ltd. Contributing to a Peace Economy in Northern Uganda: A Guide for Investors June 2009 2 International Alert Contents Acknowledgements 3 Forewords Q. B Kitara McMot, LC5 vice-chair, Gulu district 5 Dr. Maggie Kigozi, executive director, Uganda Investment Authority 6 Preface 8 Map of Uganda 10 Acronyms 11 Section 1 Introduction 14 Northern Uganda’s conflict context and economic outlook today 16 The business case for conflict-sensitive investment