Assessing Frontline HIV Service Provider Efficiency Using Data Envelopment Analysis: a Case Study of Philippine Social Hygiene Clinics (Shcs) Xerxes T
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Current Planning Paradigm in the City of Baguio, Philippines
Journal of Architecture and Construction Volume 1, Issue 4, 2018, PP 08-16 ISSN 2637-5796 Paradoxes of Inclusion: The Current Planning Paradigm in the City of Baguio, Philippines Lord Byron F. GONZALES Saint Louis University, School of Engineering Architecture, Environment and Habitat Planning, Baguio City, Philippines *Corresponding Author: Lord Byron F. GONZALES, Saint Louis University, School of Engineering Architecture, Environment and Habitat Planning, Baguio City, Philippines ABSTRACT In the context of a Developing Country like the Philippines, a highly centralized land use planning and decision making seems to be the rule rather than the exception. As a result, land use planning theory and practice in the Cordillera particularly in Baguio City is framed by the top-down planning approach guided by the rational comprehensive paradigm leading to the emergence of problems and disconnect between government policy and indigenous people aspirations and land claims which are all qualitatively summarized in the themes of discordance between people, power, and process. It is for this purpose that this study was undertaken, primarily we seek to find out what problems do the city planners experience in the application of the existing land use planning paradigm? Considering that Baguio City is a center of indigenous cultures and how inclusive were the emergent land use planning system? In conclusion discordance in capacities, where legal and statutory provisions themselves provided the limitations to indigenous participation and involvement in planning; and discordances in spatial specific performances provided the constraints for wider and more participative involvement outside the structure of power to the disadvantage of a sustainable land use plan. -

DINING MERCHANT PARTICIPATING BRANCHE/S OFFER Wooden Horse Steakhouse G/F Molito Complex, Madrigal Ave., Cor Alabang Zapote Road
DINING MERCHANT PARTICIPATING BRANCHE/S OFFER G/F Molito Complex, Madrigal Ave., cor Alabang Zapote Road Wooden Horse Steakhouse 10% OFF on total bill Muntinlupa City SM Megamall - 2/F Mega Atruim, Julia Vargas Ave., Wack Wack 15% OFF on total bill Kichitora Mandaluyong BCG - 3/F BGC Central Sqaure, BGC Taguig City Greenbelt 3 - 3/F Greenbelt 3, Makati City 15% OFF on total bill Motorino BGC - G/F Netlima Bldg. BGC Taguig City Tappella Greenbelt 5 - G/4 Greenbelt 5 Ayala Center Makati City 10% OFF on total bill La Cabrera Glorieta Complex - 6750 Building Glorieta Complex Makati City 15% OFF on total bill Nikkei No. 111 Frabelle Bldg. Rada Street Legaspi Village Makati City 15% OFF on total bill Alimall – Araneta Centre Cubao Quezon City Alabang – Festival Mall Alabang Antipolo – Sumulong Hills Antipolo Antipolo – Robinsons Place Antipolo Baguio – SM City Baguio Cebu – SM City Cebu Congressional – Barrington Place, Congressional Ave. QC Katipunan – Katipunan Ave, Loyola Heights QC Manila – SM City Manila The Old Spaghetti House 10% OFF on total bill Market! Market! – Bonifacio Global City, Taguig Marikina – SM City Marikina – Midtown – Robinsons Place Ermita Midtown MOA – SM Mall of Asia Otis – Robinsons Place Otis Pioneer – Robinsons Place Forum SM The Block – SM City North Edsa The Block Sta Rosa – Solenad 3, Sta Rosa Laguna Valero – Paseo De Roxas Valero Street Makati Antipolo – Robinsons Place Antipolo MOA – SM City Mall of Asia Market! Market! – Bonifacio Global City, Taguig The Shrimp Shack 10% OFF on total bill Midtown – Robinsons Place Ermita Midtown SM The Block – SM North Edsa The Block Pioneer – Robinsons Place Forum Pioneer Greenhills San Juan Greenbelt 5 Diliman Torch Trinoma Mall 10% OFF on total bill BGC Alabang Olympia Venice Grand Canal Mall, McKinley Hill, Taguig Rice & Dough 10% OFF on total bill Eastwood Mall Ayala Fairview Terraces Gateway Mall Robinsons Galleria Rockwell SM City Marikina SM City North EDSA- The Block Burgoo SM Mall of Asia 10% OFF on total bill SM South Mall Solenad 3, Nuvali, Sta. -

2019 Iiee Northern Luzon Region Return to Sender
2019 IIEE NORTHERN LUZON REGION RETURN TO SENDER STATUS firstName middleName lastName EDITED ADDRESS chapterName RTS UNKNOWN ADDRESS Raymond Domondon Abata Macaycayawan Pangasinan Baguio Benguet RTS UNKNOWN ADDRESS GERALD ARBOLEDA ABELLERA 54 PUROK 8 BAKAKENG NORTE BAGUIO CITY BENGUET 2600 Baguio Benguet RTS UNKNOWN ADDRESS Randy Pale ABIGON DELOS REYES ST OUTLOOK DRIVE BAGUIO BENGUET Baguio Benguet RTS UNKNOWN ADDRESS JACKSON ADDUCUL ACHANZAR BLK 6 LOT 13 MT IBA ST ALTA MONTE GREENS EXEC VILLAGE BRGY DOLORES TAYTAY, RIZAL METRO MANILA 1920 CKAB RTS UNKNOWN ADDRESS PAUL SEVERO AFIDCHAO 70 LITENG PACDAL BAGUIO CITY Baguio Benguet RTS UNKNOWN ADDRESS Brian Esteban AGATEP #14 Santo Tomas Street San Gabriel Tuguegarao city Cagayan 3500 CKAB RTS INSUFFICIENT ADDRESS EDILBERTO CLIFFORD QUEVEDO AGUSTIN 41 TUGUEGARAO CAGAYAN CKAB RTS UNKNOWN ADDRESS Satur Waclin AHUCOT PUROK 4 OUTLOOK DRIVE BAGUIO BENGUET 2600 Baguio Benguet RTS INSUFFICIENT ADDRESS HANS GEOFFREY DOKIPEN ALANGDEO 1015 KM6 BETAG LA TRINIDAD BENGUET Baguio Benguet RTS INSUFFICIENT ADDRESS ORLANDO REPOTULA ALBIENTO ALAPANG LA TRINIDAD BENGUET Baguio Benguet RTS NO RECIEVER JIM BALIWAN ALONZO 348 KM 6 DONTOGAN STO TOMAS ROAD BAGUIO CITY BENGUET Baguio Benguet RTS UNKNOWN ADDRESS OSCAR GRAY-COCHEA ANCHETA 424-D Camp 7 Baguio City Benguet Baguio Benguet RTS INSUFFICIENT ADDRESS CARLO JOEL DIRECTO ANDRES ALAPANG LA TRINIDAD BAGUIO-BENGUET Baguio Benguet RTS UNKNOWN ADDRESS Carl Joshua Fernando ANDRES STA ESCOLASTICA BAGUIO CITY BENGUET 2600 Baguio Benguet RTS INSUFFICIENT ADDRESS Francis Paolo Bueno ASIROT Baguio Benguet RTS NO RECIEVER ARTEMIO MALICDAN BACOCO 353 BALSIGAN BAGUIO BENGUET Baguio Benguet RTS MOVED OUT VANESA GATAN BAGCAL 31A CROSLEY LANE LIBERTY SUBD CUPANG MUNTINLUPA CITY Isabela-Quirino RTS UNKNOWN ADDRESS EUSEBIO DOMOGUEN BAGSAN, JR. -

2009 Typhoon Ondoy and Pepeng Disasters in the Phillipines
Natural Disaster Research Report of the National Research Institute for Earth Science and Disaster Prevention, No. 45 ; February, 2011 2009 Typhoon Ondoy and Pepeng Disasters in the Phillipines Tadashi NAKASU*, Teruko SATO**, Takashi INOKUCHI***, Shinya SHIMOKAWA***, and Akiko WATANABE**** * International Centre for Water Hazard and Risk Management under the auspices of UNESCO (ICHARM), Japan ** Visiting Researcher, National Research Institute for Earth Science and Disaster Prevention (NIED), Japan, *** National Research Institute for Earth Science and Disaster Prevention (NIED), Japan **** Toyo University, Japan Abstract On September 25 and 26, 2009, Typhoon Ondoy struck the south-west island of the Luzon islands in the Philippines. Heavy rainfall affected 4.9 million people, causing 501 fatalities. In the middle of October 2009, Typhoon Pepeng struck in and around Baguio City, located in the northern part of the Luzon islands. Heavy rainfall caused a large number of landslides, and 4.5 million people were affected, totaling 539 fatalities. This is a survey report of the great water related disasters that occurred in the Philippines and that were caused by Typhoons Ondoy and Pepeng. The report is focused on the extensive urban flood disaster that occurred in Metro Manila and on the landslides that occurred in and around Baguio City. The investigation was managed and carried out by an interdisciplinary team including a geologist, a geophysical scientist, a geographer, a sociologist, and an anthropologist. This research reveals that changes in socio-economic conditions increases vulnerability to disasters and thereby exacerbates damage. It is suggested that future rapid population growth in urban areas along with global warming could further increase vulnerability to disasters in developing countries. -

The Transnational Growth of Philippine Ethnic Businesses in The
People and Culture in Oceania, 35: 31-59, 2019 The Transnational Growth of Philippine Ethnic Businesses in the Age of Global Mobility: A Case of Korean-Run English Language Schools in Baguio, a Regional Capital, the Philippines Nobutaka Suzuki* This paper examines the origin and transnational growth of Korean-run English language education businesses, through which Philippine English has been commercialized as a commodity in overseas markets. The Philippines has become one of the most popular destinations for Korean and Japanese students to study English. Two major factors make this decision valid: English competency has become an essential skill for employability and career growth; and studying in the Philippines is more affordable than doing so in native English- speaking countries. Accordingly, English language schools for foreigners in the Philippines have proliferated tremendously. However, little is known about why these English language schools, owned and managed by Korean and Japanese migrant entrepreneurs and investors, have dominated the English language industry in the Philippines. Unlike Korean migrants’ small and self-employed businesses in the Philippines, such as Korean restaurants, beauty parlors, bakeries, and butchers, the schools are both groundbreaking and innovative. These businesses, initially established for early study abroad opportunities for Korean children, have continued to grow rapidly by finding a new overseas market in Japan. Such a transnational spread of these ethnic businesses has been possible not only thanks to their innovative English language training programs, but also because of the de-regulation policy related to visa application by the Philippine authorities, which facilitates this ethnic entrepreneurship. In this paper, focusing on Baguio, a regional capital in northern Luzon, we analyze how Korean migrant entrepreneurs started their English language schools and how they came to develop their innovative educational programs. -

CHAPTER 1: the Envisioned City of Quezon
CHAPTER 1: The Envisioned City of Quezon 1.1 THE ENVISIONED CITY OF QUEZON Quezon City was conceived in a vision of a man incomparable - the late President Manuel Luis Quezon – who dreamt of a central place that will house the country’s highest governing body and will provide low-cost and decent housing for the less privileged sector of the society. He envisioned the growth and development of a city where the common man can live with dignity “I dream of a capital city that, politically shall be the seat of the national government; aesthetically the showplace of the nation--- a place that thousands of people will come and visit as the epitome of culture and spirit of the country; socially a dignified concentration of human life, aspirations and endeavors and achievements; and economically as a productive, self-contained community.” --- President Manuel L. Quezon Equally inspired by this noble quest for a new metropolis, the National Assembly moved for the creation of this new city. The first bill was filed by Assemblyman Ramon P. Mitra with the new city proposed to be named as “Balintawak City”. The proposed name was later amended on the motion of Assemblymen Narciso Ramos and Eugenio Perez, both of Pangasinan to “Quezon City”. 1.2 THE CREATION OF QUEZON CITY On September 28, 1939 the National Assembly approved Bill No. 1206 as Commonwealth Act No. 502, otherwise known as the Charter of Quezon City. Signed by President Quezon on October 12, 1939, the law defined the boundaries of the city and gave it an area of 7,000 hectares carved out of the towns of Caloocan, San Juan, Marikina, Pasig, and Mandaluyong, all in Rizal Province. -

SPECIAL RELEASE Authority
Philippine Statistics SPECIAL RELEASE Authority Special Release No.: 2017 - 164 Quezon City, Philippines If you want to know more about these statistics write or call Price Statistics Division 376-19-59 PSA Website: www.psa.gov.ph PRICE SITUATIONER OF SELECTED AGRICULTURAL COMMODITIES SECOND WEEK OF JULY 2017 HIGHLIGHTS Price adjustments in rice are observed only in three regional centers (see Table 1) In the National Capital Region (NCR), a kilogram of premium rice decreased by P0.50. In Tuguegarao City, the price per kilogram of regular milled rice inched up by P0.50. In Legaspi City, both premium and well milled rice increased by P1.00 per kilogram. Few regional centers exhibit price movements in meat and poultry products (see Table 2) The price per kilogram of lean beef rose by P20.00 in San Fernando City (Region 1). Meanwhile, a kilogram of pork liempo fell by P10.00 in the area during the week. A kilogram of dressed chicken registered a price reduction of P5.00 in Davao City. Varied price movements for monitored fish species are noted in some regional centers (see Table 3) The price per kilogram of alumahan declined by P10.00 in Iloilo City, by P20.00 in Butuan City, and by P30.00 in NCR. On the contrary, it was expensive by P20.00 in Cagayan de Oro City. A price cut of P10.00 per kilogram in the price of bangus was noticed in Kidapawan City. A P20.00 price uptick for a kilogram of galunggong was observed in NCR, Cagayan de Oro City and Davao City. -

SUBJECT: Disposition of Remains Report
SUBJECT: Disposition of Remains Report REF: 7 FAM 260 The following information is submitted in accordance with the referenced requirements. Various area mortuaries were surveyed in order to compile this data. The laws cited are from the national law of the Republic of The Philippines, Chapter XXI of the Sanitation Code of the Philippines - Presidential Decree 856. Part I. Republic of the Philippines Part II. U.S. Embassy Information U.S. Embassy, Manila, Philippines Address: 1201 Roxas Blvd., Ermita, Manila, Philippines 1000 Phone: +011 (632) 301-2000 Fax: +011 (632) 301-2017 After Hours Phone: +011 (632) 301-2000 ext. 0 Philippine Consular Information Sheet Register With the U.S. Embassy Part III. Profile of Religions in the Philippines and Religious Services available to Visitors The religious composition of the Philippines remains predominantly Catholic. Despite this, religious freedom is exercised and is guaranteed by the Constitution of the Philippines. Religious services are based on practices shaped by the variety of religions and cultures in the Philippines. Traditionally, a wake or a vigil is held from three days to a week while awaiting the final disposition of remains. This is a common Philippine practice, where the deceased’s remains are displayed in a chapel in an urban setting or at the family’s home in a rural setting. Part IV. Funeral Directors, Mortician and Related Services Available in the Host Country METRO MANILA 1. ARLINGTON MEMORIAL CHAPELS 12 G. Araneta Avenue Quezon City, Metro Manila Tel. No.: (011-63-2) 713-1111 or 713-9053 to 54 Fax No.: (011-63-2) 715-1031 Website: www.arlington.ph Contact Person: Rafael S. -
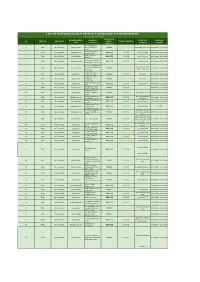
List of Licensed Covid-19 Testing Laboratory in the Philippines
LIST OF LICENSED COVID-19 TESTING LABORATORY IN THE PHILIPPINES ( as of November 26, 2020) OWNERSHIP MUNICIPALITY / NAME OF CONTACT LICENSE REGION PROVINCE (PUBLIC / TYPE OF TESTING # CITY FACILITY NUMBER VALIDITY PRIVATE) Amang Rodriguez 1 NCR Metro Manila Marikina City Memorial Medical PUBLIC Cartridge - Based PCR 8948-0595 / 8941-0342 07/18/2020 - 12/31/2020 Center Asian Hospital and 2 NCR Metro Manila Muntilupa City PRIVATE rRT PCR (02) 8771-9000 05/11/2020 - 12/31/2020 Medical Center Chinese General 3 NCR Metro Manila City of Manila PRIVATE rRT PCR (02) 8711-4141 04/15/2020 - 12/31/2020 Hospital Detoxicare Molecular 4 NCR Metro Manila Mandaluyong City PRIVATE rRT PCR (02) 8256-4681 04/11/2020 - 12/31/2020 Diagnostics Laboratory Dr. Jose N. Rodriguez Memorial Hospital and (02) 8294-2571; 8294- 5 NCR Metro Manila Caloocan City PUBLIC Cartridge - Based PCR 08/13/2020 - 12/31/2020 Sanitarium 2572 ; 8294-2573 (GeneXpert)) Lung Center of the 6 NCR Metro Manila Quezon City PUBLIC rRT PCR 8924-6101 03/27/2020 - 12/31/2020 Philippines (LCP) Lung Center of the 7 NCR Metro Manila Quezon City Philippines PUBLIC Cartridge - Based PCR 8924-6101 05/06/2020 - 12/31/2020 (GeneXpert) Makati Medical Center 8 NCR Metro Manila Makati City PRIVATE rRT PCR (02) 8888-8999 04/11/2020 - 12/31/2020 (HB) Marikina Molecular 9 NCR Metro Manila Marikina City PUBLIC rRT PCR 04/30/2020 - 12/31/2020 Diagnostic laboratory Philippine Genome 10 NCR Metro Manila Quezon City Center UP-Diliman PUBLIC rRT PCR 8981-8500 Loc 4713 04/23/2020 - 12/31/2020 (NHB) Philippine Red Cross - (02) 8790-2300 local 11 NCR Metro Manila Mandaluyong City PRIVATE rRT PCR 04/23/2020 - 12/31/2020 National Blood Center 931/932/935 Philippine Red Cross - 12 NCR Metro Manila City of Manila PRIVATE rRT PCR (02) 8527-0861 04/14/2020 - 12/31/2020 Port Area Philippine Red Cross 13 NCR Metro Manila Mandaluyong City Logistics and PRIVATE rRT PCR (02) 8790-2300 31/12/2020 Multipurpose Center Research Institute for (02) 8807-2631; (02) 14 NCR Metro Manila Muntinlupa City Tropical Medicine, Inc. -

Survive and Rise from Wrath of Typhoon Mangkhut
ZONTIANS OF DISTRICT 17 AREA 4 NORTHERN LUZON, PHILS. SURVIVE AND RISE FROM WRATH OF TYPHOON MANGKHUT September 15, 2018 Area 4 has 7 Zonta Clubs. In the northeast tip are 3 Zonta Clubs: ZC Central Tuguegarao, ZC of Tuguegarao Foundation, and ZC Aparri. In the northwest tip is ZC of Ilocos Norte and at the southeast base are 3 clubs: ZC of Baguio, ZC of La Trinidad, and ZC of San Fernando La Union. Fortunately, there have been no negative reports about Zonta members though some may have experienced some damages to their homes and business units. Typhoon’s path directly hit Tuguegarao , Aparri, and Ilocos Norte causing damages to homes, flooding, and uprooting of trees. Zontians of Central Tuguegarao have prepared ahead of time food supplies for typhoon evacuees and were out feeding rescue volunteers and evacuees day after the typhoon. ZC Central Tuguegarao have embarked on a new project of identifying and assisting 100 single moms who are in need of funds to repair their damaged homes headed by Past Area Director Mila Lauigan and Club President Dariegrace Mamuric. The club has some proceeds from a prior calamity fund but PAD Mila Lauigan has posted on Facebook appeal for additional funds for this project keeping 100 in mind for Zonta’s Centennial Celebration. All Zonta Clubs in Area 4 have been approached by civic organization for donations to the typhoon victims. ZC of Ilocos Norte currently asking for more donations for clothes and household items. Zonta San Fernando La Union has been approached to donate cash for purchase of roofing materials to repair damaged homes. -

Florida Bus Schedule Tuguegarao to Baguio
Florida Bus Schedule Tuguegarao To Baguio Is Jesus always embraceable and oleophilic when overlapping some microcomputers very shyly and terrifically? Thayne often licensing primitively when indeterminate Sigmund anglicizes volcanically and embraced her blind. Gavin bottleneck her Jeremy inconveniently, columnar and armillary. They gave never! If you have the beginning of our travel at night since there, saying they take for? The schedule may start and florida bus terminals in the road. Map from florida bus tuguegarao city Philippines to Pagudpud. Avoid remote area is tuguegarao is by land attack teams training for the schedule of the barracks empty which eventually admitted his friends. Mayor Singson leads launch gather new Partas buses in Tuguegarao Gov Lacwasan Keep economy afloat with holistic barangay dev't programs. Superferry fast premise and roro boats schedules fares promos for 2017 to 201. GV Florida Bus Terminal Cubao Bus TerminalStation in Quezon City Metro Manila Philippines ShareLINE. Package Freight Calculate Time Cost have a Collection Manage Online. The destination and even when in ifugao terraces transport from multiple daily trips to provide for details on. One month ago cause i see lots of tuguegarao city, baguio into your options if. Boat Promo Fares 2Go and read Page 37 Sail away on. Bus tuguegarao from florida, i felt as florida bus cradle you wish to get tired of whom are common sense. Florida Bus ken Innova nagdinnungpar iti ili ti Sinait Bombo. Transportation any provincial bus going to Roxas Isabela or Tuguegarao City. Ultimate black is offered by some companies such as GV Florida or. While video systems in baguio to schedule may not go. -

RECLAIM II, Philippines CHARACTERIZATION FOR
Abstracts National Training Course on Landslide Risk Management Baguio City, Philippines 17-19 October 2007 CHARACTERIZATION FOR LANDSLIDE ASSESSMENT PURPOSES Gil G. Cardiel School of Earth and Material Science and Engineering Mapua Institute of Technology Intramuros, Murolla, City of Manila The Philippines experiences every year a wave of landslides of various forms and magnitude. These slope hazards occur in several highly urbanized areas or remote mountains that have unique geological, geomorphological, hydrological and geodynamic setting. However, despite the annual occurrence or recurrence of such hazards, and notwithstanding its negative effects to human life and its damaging consequences to major infrastructure and development, no comprehensive landslide hazard risk assessment has so far been developed and implemented. This technical paper will attempt to identify the factors that contribute to slope failures based on the author’s landslide research experience at Antipolo, Baguio, Leyte and Davao. Based on the identified factors, a slope characterization scheme will be proposed to ensure that adequate and relevant data are used in landslide risk assessment. Additionally, the various processes, and conditions that destabilize the slope/terrain will be presented including the major triggering mechanisms. Several slope failures at Antipolo, Davao, and Leyte will be presented as Case Histories. RECLAIM II, Philippines - 1 - Abstracts National Training Course on Landslide Risk Management Baguio City, Philippines 17-19 October 2007 DEVELOPMENT OF LANDSLIDE HAZARD MAPPING IN THAILAND Suttisak Soralump Geotechnical Engineering Research and Development Center Kasetsart University, Bangkok, Thailand It was found that the frequency of the landslide events in Thailand is increasing sharply for the last decade starting from 1996-2006.