A Case of Thoracic Vertebral Chondroblastoma, Treated with 3-D Image Guided Resection and Reconstruction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Advances in Immune Checkpoint Inhibitors for Bone Sarcoma Therapy
UCLA UCLA Previously Published Works Title Advances in immune checkpoint inhibitors for bone sarcoma therapy. Permalink https://escholarship.org/uc/item/3k40w8f4 Authors Thanindratarn, Pichaya Dean, Dylan C Nelson, Scott D et al. Publication Date 2019-04-01 DOI 10.1016/j.jbo.2019.100221 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Journal of Bone Oncology 15 (2019) 100221 Contents lists available at ScienceDirect Journal of Bone Oncology journal homepage: www.elsevier.com/locate/jbo Review Article Advances in immune checkpoint inhibitors for bone sarcoma therapy T Pichaya Thanindratarna,b, Dylan C. Deana, Scott D. Nelsonc, Francis J. Horniceka, ⁎ Zhenfeng Duana, a Department of Orthopedic Surgery, Sarcoma Biology Laboratory, David Geffen School of Medicine, University of California, 615 Charles E. Young. Dr. South, Los Angeles, CA 90095, USA b Department of Orthopedic Surgery, Chulabhorn hospital, HRH Princess Chulabhorn College of Medical Science, Bangkok, Thailand c Department of Pathology, University of California, Los Angeles, CA, USA ARTICLE INFO ABSTRACT Keywords: Bone sarcomas are a collection of sporadic malignancies of mesenchymal origin. The most common subtypes Immune checkpoint include osteosarcoma, Ewing sarcoma, chondrosarcoma, and chordoma. Despite the use of aggressive treatment Immunotherapy protocols consisting of extensive surgical resection, chemotherapy, and radiotherapy, outcomes have not sig- Bone sarcoma nificantly improved over the past few decades for osteosarcoma or Ewing sarcoma patients. In addition, chon- Anti-PD-1/PD-L1 drosarcoma and chordoma are resistant to both chemotherapy and radiation therapy. There is, therefore, an Anti-CTLA-4 urgent need to elucidate which novel new therapies may affect bone sarcomas. -

Neurological Manifestation of Sacral Tumors
Neurosurg Focus 15 (2):Article 1, 2003, Click here to return to Table of Contents Neurological manifestation of sacral tumors MICHAEL PAYER, M.D. Department of Neurosurgery, University Hopital of Geneva, Switzerland An extensive analysis of the existing literature concerning sacral tumors was conducted to characterize their clin- ical manifestations. Although certain specific manifestations can be attributed to some of the tumor types, a more general pattern of clinical presentation of an expansive sacral lesion can be elaborated. Local pain with or without pseudoradicular or radicular radiation is the most frequent initial symptom and is usually followed by the manifesta- tion of a lumbosacral sensorimotor deficit; bladder/bowel and/or sexual dysfunction appear throughout the natural course of disease. KEY WORDS • sacrum • tumor • lesion • neurological presentation All sacral and presacral tumors are rare.32,93 In one se- REVIEW OF SACRAL ANATOMY ries patients with these tumors were estimated to account for approximately one in 40,000 hospital admissions.93 Osseous Structures of the Sacrum Tumors arising from the bone of the sacrum are by far the The sacrum is a complex bone, comprising five sacral most frequent sacral tumors; chordomas are the most com- vertebrae that have fused. In its center lies the longitudi- mon and GCTs the second most common.20,46,50,61,74,81,98 nal sacral canal, which opens caudally posteriorly into the Although sacrococcygeal teratoma is the most common sacral hiatus, an incomplete posterior closure of the S-5 sacral tumor in neonates, it is very rare in adults.30,45,66 lamina. The thick anterior or pelvic face of the sacrum is The author conducted an extensive analysis of the exist- concave and contains four right- and left-sided anterior ing literature concerning tumors of the sacrum to charac- sacral foramina. -

Malignant Bone Tumors (Other Than Ewing’S): Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up by Spanish Group for Research on Sarcomas (GEIS)
Cancer Chemother Pharmacol DOI 10.1007/s00280-017-3436-0 ORIGINAL ARTICLE Malignant bone tumors (other than Ewing’s): clinical practice guidelines for diagnosis, treatment and follow-up by Spanish Group for Research on Sarcomas (GEIS) Andrés Redondo1 · Silvia Bagué2 · Daniel Bernabeu1 · Eduardo Ortiz-Cruz1 · Claudia Valverde3 · Rosa Alvarez4 · Javier Martinez-Trufero5 · Jose A. Lopez-Martin6 · Raquel Correa7 · Josefina Cruz8 · Antonio Lopez-Pousa9 · Aurelio Santos10 · Xavier García del Muro11 · Javier Martin-Broto10 Received: 7 July 2017 / Accepted: 15 September 2017 © The Author(s) 2017. This article is an open access publication Abstract Primary malignant bone tumors are uncommon of a localized bone tumor, with various techniques available and heterogeneous malignancies. This document is a guide- depending on the histologic type, grade and location of the line developed by the Spanish Group for Research on Sar- tumor. Chemotherapy plays an important role in some che- coma with the participation of different specialists involved mosensitive subtypes (such as high-grade osteosarcoma). in the diagnosis and treatment of bone sarcomas. The aim is In other subtypes, historically considered chemoresistant to provide practical recommendations with the intention of (such as chordoma or giant cell tumor of bone), new targeted helping in the clinical decision-making process. The diag- therapies have emerged recently, with a very significant effi- nosis and treatment of bone tumors requires a multidiscipli- cacy in the case of denosumab. Radiation therapy is usually nary approach, involving as a minimum pathologists, radi- necessary in the treatment of chordoma and sometimes of ologists, surgeons, and radiation and medical oncologists. other bone tumors. Early referral to a specialist center could improve patients’ survival. -
View Presentation Notes
When is a musculoskeletal condition a tumor? Recognizing common bone and soft tissue tumors Christian M. Ogilvie, MD Assistant Professor of Orthopaedic Surgery University of Pennsylvania University of Pennsylvania Department of Orthopaedic Surgery Purpose • Recognize that tumors can present in the extremities of patients treated by athletic trainers • Know that tumors may present as a lump, pain or both • Become familiar with some bone and soft tissue tumors University of Pennsylvania Department of Orthopaedic Surgery Summary • Introduction – Pain – Lump • Bone tumors – Malignant – Benign • Soft tissue tumors – Malignant – Benign University of Pennsylvania Department of Orthopaedic Surgery Summary • Presentation • Imaging • History • Similar conditions –Injury University of Pennsylvania Department of Orthopaedic Surgery Introduction •Connective tissue tumors -Bone -Cartilage -Muscle -Fat -Synovium (lining of joints, tendons & bursae) -Nerve -Vessels •Malignant (cancerous): sarcoma •Benign University of Pennsylvania Department of Orthopaedic Surgery Introduction: Pain • Malignant bone tumors: usually • Benign bone tumors: some types • Malignant soft tissue tumors: not until large • Benign soft tissue tumors: some types University of Pennsylvania Department of Orthopaedic Surgery Introduction: Pain • Bone tumors – Not necessarily activity related – May be worse at night – Absence of trauma, mild trauma or remote trauma • Watch for referred patterns – Knee pain for hip problem – Arm and leg pains in spine lesions University of Pennsylvania -

A Rare Case of Chondromyxoid Fibroma of the Scapula Jay B
A Case Report & Literature Review A Rare Case of Chondromyxoid Fibroma of the Scapula Jay B. Jani, MD, Kathleen S. Beebe, MD, Meera Hameed, MD, and Joseph Benevenia, MD hondromyxoid fibroma (CMF) is a rare benign Plain radiography (Figures 1A, 1B) and computed tumor, apparently derived from cartilage-forming tomography (CT) scan (Figure 2) revealed an expansile connective tissue. The name is highly descriptive lesion of the right scapula with central calcification sug- of this distinctive tumor and has gained accep- gesting chondroid-type matrix. There was some thinning Ctance.1 The entity was first described in 1948 by Jaffe and of the cortex but no obvious cortical breach or associated Lichtenstein,2 who presented 8 cases and emphasized the soft-tissue mass. MRI (Figure 3) revealed a 5×3×2.5- danger of mistaking this benign neoplasm for a malignant cm expansile lesion involving the inferior border of the lesion, chondrosarcoma in particular. Approximately two scapula. T2-weighted images showed a heterogeneous thirds of the recorded cases of this tumor have been in the mass with bright signal intensity. There was considerable long tubular bones and one third in the proximal tibia.1,3,4 A edema in the teres minor and subscapularis muscle bel- scapular origin of this tumor is exceedingly rare.1,5-10 lies. No fluid–fluid levels were seen. Additional workup We report the case of a 13-year-old girl with chondro- included a chest CT scan and a whole-body bone scan. myxoid fibroma of the scapula. This case is of interest The bone scan revealed increased focal uptake to the right because of the rarity and unusual location of the tumor. -

Giant Cell Tumor of Bone
GIANT CELL TUMOR OF BONE Definition. First described by Jaffe et al. 1, giant cell tumor of bone is a locally aggressive primary neoplasm of bone that is composed of proliferation of bland looking oval to polyhedral mononuclear cells, admixed with evenly distributed, osteoclast-type giant cells. The tumor is typically located with the epiphysis of long tubular bones or the epiphyseal equivalent in other bones 2-4. In the most current WHO classification of bone tumors, giant cell tumor of bone is classified as a locally aggressive, rarely metastasizing neoplasm 3. General features. Accounts for approximately 6% of primary bone tumors and 20% of benign bone tumors 5. Previously, it was believed that the giant cells were formed by the fusion of the mononuclear neoplastic cells and it was assumed that the giant cells might also be neoplastic. Currently, giant cell tumor of bone is considered a neoplastic process derived from mononuclear cells exhibiting osteoblastic phenotype that express RANK-ligand (RANKL), which induces the formation of the osteoclast-type giant cells, from which the tumor derives its name. Most giant cell tumors of bone arise de-novo but can also arise in bones affected by Paget disease of bone. Clinical features. Most patients are skeletally mature at the time of diagnosis (usually between the age of 20-40 years); it rarely arises in skeletally immature individuals; less than 10% arise in patients under the age of 18 years 6. Females are affected more common than males. It is more common in the Chinese population accounting for approximately 20% of primary bone tumors 7. -

Pelvic Chondroblastoma in an Adolescent. New Treatment Approach
www.medigraphic.org.mx Acta Ortopédica Mexicana 2011; 25(6): Nov.-Dec: 388-394 Clinical case Pelvic chondroblastoma in an adolescent. New treatment approach Rico-Martínez G,* Linares-González L,** Delgado-Cedillo E,** Cerrada-Moreno L,*** Clara-Altamirano M,*** Pichardo-Bahena R**** National Rehabilitation Institute. Mexico, D.F. ABSTRACT. Surgical management of tumors RESUMEN. Los tumores que están localizados located in the spine and the pelvis involves greater en la columna vertebral y en la pelvis tienen aso- diffi culty. Moreover, these tumors are usually very ciada una mayor difi cultad para el manejo quirúr- large and vascularized. Preoperative embolization gico. Además, estos tumores son habitualmente de of the internal iliac artery is a relatively safe pro- gran tamaño y ricamente vascularizados. La em- cedure that may reduce the risk of bleeding and lo- bolización prequirúrgica arterial de la arteria ilía- cal recurrence in the case of benign tumors. Chon- ca interna tiene la bondad de ser un procedimiento droblastoma is a tumor that is rarely located in the relativamente seguro que puede reducir el riesgo pelvis; its more frequent location is the triradiate de sangrado y de recidiva local en tumores benig- cartilage. We describe a case of a chondroblasto- nos. El condroblastoma es un tumor raro en la pel- ma with a relapsing aneurysmal cystic component vis y la localización más frecuente es en el cartílago in the acetabulum of an adolescent patient. Treat- trirradiado. Se presenta un caso de condroblasto- ment consisted of embolization of the internal iliac ma con componente quístico aneurismático recidi- artery, fl uid hyperthermia, hydrogen peroxide and vante en el acetábulo de un paciente adolescente. -

Chondroblastoma: a Rare Cause of Femoral Neck Fracture in a Teenager Michael D
A Case Report & Literature Review Chondroblastoma: A Rare Cause of Femoral Neck Fracture in a Teenager Michael D. Paloski, DO, Michael J. Griesser, MD, Mark E. Jacobson, MD, and Thomas J. Scharschmidt, MD chanter apophysis, review the literature, and present Abstract learning points for this diagnosis and treatment. Chondroblastomas usually present in the epiphyseal The patient provided written informed consent for region of bones in skeletally immature patients. These print and electronic publication of this case report. uncommon, benign tumors are usually treated with curet- tage and use of a bone-void filler. ASE EPORT Here we report a case of a hip fracture secondary to C R an underlying chondroblastoma in a 19-year-old woman. The patient was an otherwise healthy 19-year-old Open biopsy with intraoperative frozen section pointed white woman who presented to the emergency toward a diagnosis of chondroblastoma. Extended curet- department with the chief report of right hip pain, tage was performed, followed by cryotherapy with a liquid and inability to ambulate after slipping on ice and nitrogen gun and filling of the defect with calcium phos- falling on her left side from standing height. She phate bone substitute. The femoral neck fracture was stated she had a 3-year history of intermittent stabilized with a sliding hip screw construct. The patient right hip pain before this incident. At that time, her progressed well and continued to regain functional sta- primary care physician had worked up her initial tus. A final pathology report confirmed the lesion to be a symptoms with radiographs, which were reported chondroblastoma. -

Evaluation of Some Histochemical and Immunohistochemical Criteria of Round Cell Tumors of Bone Eman M
Original article 21 Evaluation of some histochemical and immunohistochemical criteria of round cell tumors of bone Eman M. S. Muhammada, Zeinab H. El-badawia, Sana S. Krooshc and Hassan H. Noamanb Departments of aPathology, bOrthopedic Surgery, Background/aims Faculty of Medicine, University of Sohag, Sohag and cDepartment of Pathology, Faculty of Medicine, The differential diagnosis of round cell tumors of bone (RCTB), Ewing sarcoma, small- University of Assiut, 82524 Assiut, Egypt cell osteosarcoma, mesenchymal chondrosarcoma, osteoblastoma, chondroblastoma, Correspondence to Eman M. S. Muhammad, primary bone lymphoma, and multiple myeloma still remains a challenge. Given the Department of Pathology, Faculty of Medicine, significant differences in treatment, an accurate diagnosis is crucial. This study aimed University of Sohag, Sohag, Egypt Tel:+ 02 093 460 2963; e-mail: [email protected] to evaluate some histochemical and immunohistochemical criteria of RCTB. Participants and methods Received 29 January 2012 Accepted 6 March 2012 Periodic acid-Schiff (PAS), CD99, CD138, osteocalcin, and leukocyte common antigen (LCA) were evaluated in 113 patients with RCTB. Journal of the Arab Society for Medical Research 2012, 7:21–32 Results PAS was positive in neoplastic cells of all Ewing sarcomas, 27% of osteosarcomas, 92% of chondrosarcomas, all osteoblastomas and chondroblastomas, and the osteoid tissue of all osteosarcomas and osteoblastomas. CD99 was positive in all Ewing sarcomas, in 11, 4, and 11% of osteoblastomas, multiple myelomas, and bone lymphomas, respectively. CD99 was higher in Ewing sarcoma than in other RCTB (Po0.0001). Osteocalcin was positive in neoplastic cells of all osteosarcomas, osteoblastomas, and 20% of chondroblastomas, 84, and 78% of osteoid of osteosarcomas and osteoblastomas, respectively. -

Chondroblastoma: an Unusual Cause of Shoulder Pain in Adolescence
Lambert, J et al 2016 Chondroblastoma: An Unusual Cause Of Shoulder Pain In Adolescence. Journal of the Belgian Society of Radiology, 100(1): 16, pp. 1–3, DOI: http://dx.doi.org/10.5334/jbr-btr.1027 CASE REPORT Chondroblastoma: An Unusual Cause Of Shoulder Pain In Adolescence Julie Lambert*, Tom Verstraeten† and Koen Mermuys‡ Chondroblastoma is a rare benign bone tumor, most often localized in the epiphysis of long bones. We report a case of atraumatic shoulder pain in a 17-year old soccer player. This chondroblastoma case dem- onstrates the difficult differentiation of chondroblastoma from giant cell tumor and clear cell chondrosar- coma and highlights possible pitfalls and clinical importance. Keywords: Chondroblastoma; Shoulder pain; Radiography; Magnetic resonance imaging; Multidetector computed tomography A 17-year-old athletic male presented to the orthopedic center for consultation regarding left shoulder pain last- ing more than two months. There was no recent trauma. Clinical examination was unremarkable, with a normal mobility of the shoulder joint. Ultrasound examination of the shoulder was normal. There was no fever or any other sign of systemic illness and laboratory findings were normal. A single corticoid injection was given, which did not result in any pain relief. Subsequently, magnetic reso- nance (MR) arthrography, performed for the detection of ligamentous or labral injury, revealed a bone lesion located at the epiphysis of the humeral head (Figure 1). The location and morphology of this lesion, as well as the age of the patient, were suggestive for chondroblas- toma. However, the hyper-intense signal intensity on the T2-weighted images was a typical for this diagnosis. -
Epiphyseal Chondromyxoid Fibroma with Prominent Adipose Tissue: an Unusual Radiologic and Histologic Presentation
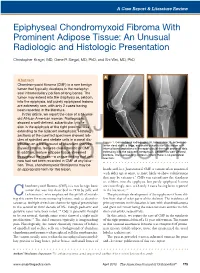
A Case Report & Literature Review Epiphyseal Chondromyxoid Fibroma With Prominent Adipose Tissue: An Unusual Radiologic and Histologic Presentation Christopher Kragel, MD, Gene P. Siegal, MD, PhD, and Shi Wei, MD, PhD A B Abstract Chondromyxoid fibroma (CMF) is a rare benign tumor that typically develops in the metaphy- seal intramedullary portion of long bones. The tumor may extend into the diaphysis or, seldom, into the epiphysis, but purely epiphyseal lesions are extremely rare, with only 2 cases having been reported in the literature. In this article, we report the case of a 51-year- old African American woman. Radiographs showed a well-defined, subarticular lytic le- sion in the epiphysis of the right proximal tibia extending to the adjacent metaphysis.AJO Histologic sections of the curetted specimen showed lob- ules of spindled and stellate cells in a zonal dis- Figure 1. Conventional radiographs (A, lateral view; B, anteropos- tribution on a background of abundant chondro- terior view) show a large, expansile subarticular lytic lesion with myxoid stroma, features characteristic of CMF. internal bony septations in the epiphysis of the right proximal tibia In addition, mature adipose tissue streamed extending into the adjacent metaphysis. Lesion has well-defined borders. The surrounding cortex is intact; there is no periosteal throughout the lesion—a unique finding that until reaction. DOnow had not been recorded NOT in CMF at any loca- COPY tion. Thus, chondromyxoid fibrolipoma may be an appropriate term for this lesion. hands and -
Understanding Bone Sarcoma
Understanding bone sarcoma sarcoma.org.uk 1 About this Contents booklet This booklet is aimed at anyone We offer information, support What is bone sarcoma? 4 who has been diagnosed with a and a signposting service Signs and symptoms 5 bone sarcoma. to other organisations that can help. How is bone sarcoma diagnosed? 6 It explains what bone sarcoma is, how it is diagnosed and the Treatment may vary depending What tests or scans might I have? 7 treatment options available on which nation of the UK you Understanding my diagnosis 8 to you. live in. Please ask your doctor or sarcoma clinical nurse specialist It also has information on Who will treat me? 10 about the treatment options where you can go for support. What treatment is available? 11 available in your area. It is your personal guide with – Chondrosarcoma space available to keep all your diagnosis information and the – Osteosarcoma details of your next hospital – Ewing’s sarcoma appointments. – Chordoma You can also include contact What happens after I have had my treatment? 20 details of your doctor, sarcoma clinical nurse specialist or other Will my cancer come back? 21 health professionals. What if my cancer spreads? 21 You may find it useful to What support is available? 22 share the information in this booklet with your partner My diagnosis details 26 or family members to help My sarcoma multi-disciplinary team (MDT) 27 them understand about bone sarcoma. If you have questions about anything you read in this booklet please contact Sarcoma UK. 2 3 means bone.