Commercial Remittance Advice Code Descriptions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
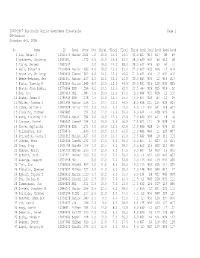
2006-2007 Wisconsin Junior Open/Open Crosstable Page 1 UW-Oshkosh November 4-5, 2006
2006-2007 Wisconsin Junior Open/Open Crosstable Page 1 UW-Oshkosh November 4-5, 2006 No. Name ID Team Rate Pts TBrk1 TBrk2 TBrk3 TBrk4 Rnd1 Rnd2 Rnd3 Rnd4 Rnd5 1 Luo, Brian J 12910173 Madisn 2024 5.0 16.0 15.0 54.0 32.0 W27 W13 W17 W9 W3 2 Mckinney, Christop 12934651 1772 4.5 16.0 14.5 52.0 28.0 W30 W33 W6 W10 D8 3 Yusim, Sergey 12852542 4.0 19.0 14.0 58.0 28.0 W12 W29 W5 W4 L1 4 Bell, Samuel W 21014944 Madisn 1663 4.0 15.0 13.0 51.0 22.0 W22 W35 W16 L3 W14 5 Brown Jr, Christop 12849430 GlenNi 1501 4.0 14.5 12.0 46.0 21.0 W31 W34 L3 W21 W16 6 Webne-Behrman, Ger 12901591 Madisn 1437 4.0 14.5 12.0 43.5 20.0 W43 W36 L2 W19 W13 7 Hintz, Timothy M 12752556 Marion 1545 4.0 13.5 12.0 44.5 20.0 W37 W19 L10 W33 W25 8 Bowen, John Armbru 12779264 USM 1596 4.0 13.5 11.5 42.0 22.5 -H- W26 W15 W14 D2 9 Her, Sou 12805616 MSL 1687 3.5 16.5 12.5 51.0 19.5 W44 W21 W18 L1 D10 10 Bowen, James H 12786949 USM 1278 3.5 14.0 12.5 45.0 15.5 W53 W49 W7 L2 D9 11 Miller, Joshua D 12871494 Marion 1516 3.5 13.5 10.0 44.5 18.0 W38 D15 L14 W24 W29 12 Dumke, Nathan C 12849428 Marion 1227 3.5 13.5 9.0 43.0 16.0 L3 W41 W34 D18 W27 13 Clausing, Michael 12864685 1254 3.0 17.0 10.0 50.0 16.0 W24 L1 W38 W20 L6 14 Wang, Xiaoming Tim 12976014 MadJf 1254 3.0 16.5 12.0 47.5 17.0 W40 W20 W11 L8 L4 15 Lancour, Daniel 12859342 JanesP 1158 3.0 16.0 9.5 46.5 17.5 W23 D11 L8 W28 D18 16 Ghose, Saptarshi 12870578 USM 1271 3.0 14.5 11.0 42.5 13.0 W45 W28 L4 W39 L5 17 Gallenberg, Bob 12779870 1436 3.0 13.5 10.0 41.5 11.0 W41 W46 L1 L25 W37 18 Petrashek, Casey D 12911815 Madisn 1427 3.0 13.0 -
Right of Passage
Right of Passage: Reducing Barriers to the Use of Public Transportation in the MTA Region Joshua L. Schank Transportation Planner April 2001 Permanent Citizens Advisory Committee to the MTA 347 Madison Avenue, New York, NY 10017 (212) 878-7087 · www.pcac.org ã PCAC 2001 Acknowledgements The author wishes to thank the following people: Beverly Dolinsky and Mike Doyle of the PCAC staff, who provided extensive direction, input, and much needed help in researching this paper. They also helped to read and re-read several drafts, helped me to flush out arguments, and contributed in countless other ways to the final product. Stephen Dobrow of the New York City Transit Riders Council for his ideas and editorial assistance. Kate Schmidt, formerly of the PCAC staff, for some preliminary research for this paper. Barbara Spencer of New York City Transit, Christopher Boylan of the MTA, Brian Coons of Metro-North, and Yannis Takos of the Long Island Rail Road for their aid in providing data and information. The Permanent Citizens Advisory Committee and its component Councils–the Metro-North Railroad Commuter Council, the Long Island Rail Road Commuters Council, and the New York City Transit Riders Council–are the legislatively mandated representatives of the ridership of MTA bus, subway, and commuter-rail services. Our 38 volunteer members are regular users of the MTA system and are appointed by the Governor upon the recommendation of County officials and, within New York City, of the Mayor, Public Advocate, and Borough Presidents. For more information on the PCAC and Councils, please visit our website: www.pcac.org. -

Heater Element Specifications Bulletin Number 592
Technical Data Heater Element Specifications Bulletin Number 592 Topic Page Description 2 Heater Element Selection Procedure 2 Index to Heater Element Selection Tables 5 Heater Element Selection Tables 6 Additional Resources These documents contain additional information concerning related products from Rockwell Automation. Resource Description Industrial Automation Wiring and Grounding Guidelines, publication 1770-4.1 Provides general guidelines for installing a Rockwell Automation industrial system. Product Certifications website, http://www.ab.com Provides declarations of conformity, certificates, and other certification details. You can view or download publications at http://www.rockwellautomation.com/literature/. To order paper copies of technical documentation, contact your local Allen-Bradley distributor or Rockwell Automation sales representative. For Application on Bulletin 100/500/609/1200 Line Starters Heater Element Specifications Eutectic Alloy Overload Relay Heater Elements Type J — CLASS 10 Type P — CLASS 20 (Bul. 600 ONLY) Type W — CLASS 20 Type WL — CLASS 30 Note: Heater Element Type W/WL does not currently meet the material Type W Heater Elements restrictions related to EU ROHS Description The following is for motors rated for Continuous Duty: For motors with marked service factor of not less than 1.15, or Overload Relay Class Designation motors with a marked temperature rise not over +40 °C United States Industry Standards (NEMA ICS 2 Part 4) designate an (+104 °F), apply application rules 1 through 3. Apply application overload relay by a class number indicating the maximum time in rules 2 and 3 when the temperature difference does not exceed seconds at which it will trip when carrying a current equal to 600 +10 °C (+18 °F). -

K-12 Individual No. Name Team Gr Rate Pts Tbrk1 Tbrk2 Tbrk3 Tbrk4
K-12 Individual No. Name Team Gr Rate Pts TBrk1 TBrk2 TBrk3 TBrk4 Rnd1 Rnd2 Rnd3 Rnd4 Rnd5 Rnd6 1 Chakraborty, Dipro 11 2299 5.5 21 24 43 20.5 W27 W12 W5 W32 W8 D3 State Champion, AZ Denker Representative 2 Yim, Tony Sung BASISS 8 2135 5 20.5 23.5 38.5 17.5 W24 W10 D3 D16 W11 W9 3 Aletheia-Zomlefer, Soren CHANPR 11 1961 5 20 23 35.5 18.5 W25 W26 D2 W40 W15 D1 4 Desmarais, Nicholas Eduard NOTRED 10 1917 5 18 20 33 18 W39 W23 W18 L15 W10 W8 5 Wong, Kinsleigh Phillip CFHS 10 1992 4.5 20 20 24.5 15 -X- W17 L1 W26 D7 W15 6 Todd, Bryce BASISC 10 1923 4.5 17 19 26.5 14.5 W38 D18 L9 W23 W21 W16 7 Chaliki, Kalyan DSMTHS 9 1726 4.5 17 18.5 26 15 W46 L16 W28 W22 D5 W17 8 Li, Bohan UHS 9 2048 4 22 25 29 18 W30 W11 W45 W9 L1 L4 9 Mittal, Rohan CFHS 9 1916 4 19.5 20.5 23 17 W47 W22 W6 L8 W20 L2 10 Pennock, Joshua CFHS 10 1682 4 19 22 24 14 W31 L2 W25 W21 L4 W29 11 Aradhyula, Sumhith CFHS 9 1631 4 18 20 22 14 W41 L8 W38 W13 L2 W19 12 Johnston, Nicolas Godfrey CFHS 9 1803 4 18 19.5 21 13 W43 L1 W29 L17 W24 W20 13 Martis, Tyler BRHS 12 1787 4 17 18 21 13 W42 L15 W24 L11 W18 W22 14 Plumb, Justin Rodney GCLACA 10 1700 4 16 17 20 13 W51 L32 W19 L20 W28 W27 15 Martinez, Isaac GLPREP 10 2159 3.5 21.5 24.5 27.5 16 W28 W13 D16 W4 L3 L5 16 Chen, Derek H CFHS 10 1965 3.5 21 23.5 26 15.5 W35 W7 D15 D2 D17 L6 17 Woodson, Tyler GILBHS 1640 3.5 19 19 17.5 14 W50 L5 W30 W12 D16 L7 18 Cancio, Aiya CFHS 9 1469 3.5 18.5 20 17.5 12.5 W36 D6 L4 W46 L13 W25 AZ Girls' Invitational Representative 19 Folden, Kurt CHANPR 10 1207 3 14 18 12 10 L32 W50 L14 W31 W23 L11 20 Thornton, -

APCD Landscape -National Association of Health Data Organizations (NAHDO) 28Th Annual Conference
All-Payer Claims Database Policy & Procedures Enhancements Subcommittee Meeting May 8, 2014 1 Agenda • Call to Order and Introductions • Public Comment • Approval of Minutes for the February 21, 2014 Meeting • Overview of Claims Adjustment Reason Codes and Remittance Advice Codes • Review of Denied Claims Data Use Cases • Discussion of Dental Data Collection and Stakeholder Engagement • Next Steps • Future Meetings 2 Overview of Claims Adjustment Reason Codes and Remittance Advice Codes 3 Denial and Adjustment Code Sets Claim Adjustment Remittance Advice Claim Adjustment Group Reason Codes Remark Codes Codes (CAGC) (CARC) (RARC) NCPDP Reject Code Offers a reason for the Delivers supplemental positive/negative Provides information Assigns financial responsibility information (in addition financial adjustment regarding a retail for the Claims Adjustment to a CARC) about why a Purpose: specific to particular pharmacy claim Reason Code (CARC). claim or service line is claim or rejection not paid in full service referenced Code Set Codes National Council for Centers for Medicare & ASC X12 Standards Committee Maintenance Committee Prescription Drug Steward: Medicaid Services (CMS) (BCBSA) Programs (NCPDP) Count: 5 ~268 ~930 NA Example: CO - Contractual Obligation CR - Corrections and Reversal N19 - Procedure code 26 - Expenses incurred OA - Other Adjustment incidental to primary NA prior to coverage. PI - Payer Initiated Reductions procedure. PR - Patient Responsibility http://www.wpc- http://www.wpc- Reference: http://www.wpc- edi.com/reference/codelists/h edi.com/reference/codelists/h edi.com/reference/codelists/healthcare/cl https://www.ncpdp.org/ aim-adjustment-reason-codes/ ealthcare/claim-adjustment- ealthcare/remittance-advice- reason-codes/ remark-codes/ 4 Denial and Adjustment Code Set Values Examples1 ASC X12 CARC CARC Description2 RARC RARC Description3 CAGC 163 Attachment/other documentation referenced on the N678 Missing post-operative images/visual field results. -

Leisure Pass Group
Explorer Guidebook Empire State Building Attraction status as of Sep 18, 2020: Open Advanced reservations are required. You will not be able to enter the Observatory without a timed reservation. Please visit the Empire State Building's website to book a date and time. You will need to have your pass number to hand when making your reservation. Getting in: please arrive with both your Reservation Confirmation and your pass. To gain access to the building, you will be asked to present your Empire State Building reservation confirmation. Your reservation confirmation is not your admission ticket. To gain entry to the Observatory after entering the building, you will need to present your pass for scanning. Please note: In light of COVID-19, we recommend you read the Empire State Building's safety guidelines ahead of your visit. Good to knows: Free high-speed Wi-Fi Eight in-building dining options Signage available in nine languages - English, Spanish, French, German, Italian, Portuguese, Japanese, Korean, and Mandarin Hours of Operation From August: Daily - 11AM-11PM Closings & Holidays Open 365 days a year. Getting There Address 20 West 34th Street (between 5th & 6th Avenue) New York, NY 10118 US Closest Subway Stop 6 train to 33rd Street; R, N, Q, B, D, M, F trains to 34th Street/Herald Square; 1, 2, or 3 trains to 34th Street/Penn Station. The Empire State Building is walking distance from Penn Station, Herald Square, Grand Central Station, and Times Square, less than one block from 34th St subway stop. Top of the Rock Observatory Attraction status as of Sep 18, 2020: Open Getting In: Use the Rockefeller Plaza entrance on 50th Street (between 5th and 6th Avenues). -

Nuclear Weapons Databook
Nuclear Weapons Databook Volume I11 U.S. Nuclear Warhead Facility Profiles Nuclear Weapons Databook Volume I11 U.S. Nuclear Warhead Facility Profiles Thomas B. Cochran, William M. Arkin, Robert S. Morris, and Milton M. Hoenig A book by the Natural Resources Defense Council, Inc. BALUNGER PUBLISHING COMPANY Cambridge, Massachusetts A Subsidiary of Harper & Row, Publishers, Inc. Copyright a 1987 by the Natural Resources Defense Council, Inc. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or trans- mitted in any form or by any means, electronic, mechanical, photocopy, recording or otherwise, without the prior written consent of the publisher. International Standard Book Number: 0-88730-126-6 (CL) 0-88730-146-0 (PB) Library of Congress Catalog Card Number: 82-24376 Printed in the United States of America Library of Congress CataloGng-iii-PublicationData U.S. nuclear warhead facility profiles. (Nuclear weapons databook ;v. 3) "A book by the Natural Resources Defense Council, Inc." Includes bibliographical references and index. 1. Nuclear weapons-United States. 2. Munitions-United States. I. Cochran, Thomas B. 11. Natural Resources Defense Council. 111. Title: US nuclear warhead facility profiles. IV. Title: United States nuclear warhead facility profiles. V. Series: Cochran, Thomas B. Nuclear weapons databook ;v. 3. U264.C6 1984 vol. 3 355.8'25119'0973 87-14552 [U264] ISBN 0-88410-172-X (v. 1) ISBN 0-88410-173-8 (pbk. : v. 1) ISBN 0-88730-124-X (v. 2) ISBN 0-88730-125-8 (pbk. : v. 2) ISBN 0-88730-126-6 (v. 3) ISBN 0-88730-146-0 (pbk. -

Public Transit in NY, the Metropolitan Transportation Authority: Its Future and History Carrigy
Hofstra University, Department of Global Studies & Geography, Honors Essay Public Transit in New York The Past and Future of the Metropolitan Transportation Authority Michael Carrigy Fall 2010 Supervised by Dr. Jean-Paul Rodrigue Table of Contents Introduction: Public Transportation in the United States 3 New York’s MTA and Its Subsidiaries 7 MTA’s Departmental Structure 11 The MTA’s Report Card 19 Planning for the Future 26 Appendix 30 Bibliography 51 2 Introduction: Public Transportation in the United States The Rise of the Suburb and the Decline of the Inner City From the 1950s to the 1970s, race riots, deindustrialization, the rise of consumerism, and the rise of the automobile contributed to the decline of America’s cities and the rise of the suburbs. For instance, downtown Hempstead lost its major department store and saw a decline in population and a rise in crime. Nearby in Levittown, houses were mass produced for market consumption at a time when demand for detached suburban style houses skyrocketed. The pressure for housing not only came from a housing shortage for returning veterans but from FHA policies which subsidized mortgages for new houses. The policy made it significantly cheaper in some cases to buy a new home than to either rent an apartment or refurbish an existing home. To serve these low density areas, malls, just like the Roosevelt Field Mall in Garden City, were erected in suburban places across the country. Roosevelt Field gladly made up for Hempstead’s diminishing retailing in its downtown. Due to an increase in the number of malls, many cities saw areas just outside of their downtown decline into severe and in some cases complete abandonment. -

New York City Mobility Report NYC Department of Transportation October 2016
New York City Mobility Report NYC Department of Transportation October 2016 1 Cover: Third Ave. at 57th St., Manhattan 2 This page: 86th St. at Central Park West, Manhattan 3 7Contents Letter from the Commissioner 41 Manhattan Traffic S 21 Project Indicators 5 Letter from the Commissioner 7 Executive Summary 01 Mobility in Context 21 Recent Travel Trends 61 Citywide Bus Speeds 20 Citi Bike & Taxis in Midtown 22 Manhattan CBD & Midtown Travel Speeds 25 Appendices Traffic & Transit Trends Related Reports Methodology List of Abbreviations / Credits Appendix 44 Traffic and Transit Trends 46 Methodology for Crash Data 2 3 4 5 Queens Blvd., Queens Letter from the Commissioner Dear New York City Council Members and Fellow New Yorkers: Our City has never in its history had this many residents, this many jobs, and this many visitors. In the last five years alone, we added as many jobs as we had added in the previous thirty years. This means that New York City has never had to move as many people and goods as it has to today. Our vibrancy is something to be celebrated—and examined. How did we get to this position? And how will we maintain and sustain it? This NYC Mobility Report seeks to provide New Yorkers the context of where we have been, where we are now, and the challenges we face as we chart our City’s course in the 21st Century. We are currently providing a historic level of mobility due to wise decisions to invest in high performance modes—beginning with the reinvestment in our mass transit system that began in the 1980s, and continuing today through NYCDOT’s management of our streets to support travel by bus, on foot or by bicycle. -
Review of the a and C Lines
Review of the A and C Lines ,. December 11, 2015 Page intentionally left blank AC Line Review Executive Summary Executive Summary The attached report provides a comprehensive review of operations on the A and C lines. Combined, the two lines serve 800,000 riders a day across three boroughs and connect to many of the most important intermodal hubs in New York City. The A differs from most other New York City Transit subway lines in that its route splits three ways at its southern end in eastern Queens. It is also exceptionally long, at 32 miles between 207 St and Far Rockaway-Mott Av. Like many other subway lines, it merges several times with other lines. The combination of these traits tends to reduce reliability. In contrast, the C is a shorter line scheduled to run less frequently than the A and many other lines. C service is relatively reliable, even though it has historically been assigned some of the oldest cars in the system. This review has been prepared within the context of NYC Transit’s service planning procedures, and all discussions of service levels take into account established guidelines for designing and scheduling service. NYC Transit determines how many trains run on a given line based on a number of factors, including line capacity, equipment availability, and the Rapid Transit Loading Guidelines. The Guidelines ensure that limited resources are equitably allocated throughout the system by establishing, by time of day, maximum passenger load levels and minimum service frequencies, where operationally feasible. The Guidelines are applied by evaluating average ridership levels at locations where trains are most heavily loaded (“peak load points”) to develop recommended service frequencies, where operationally feasible. -

Transit and Bus Committee Meeting September 2020 Committee Members H
Transit and Bus Committee Meeting September 2020 Committee Members H. Mihaltses, Chair D. Jones A. Albert L. Lacewell J. Barbas R. Linn N. Brown D. Mack V. Calise R. Mujica L. Cortés-Vázquez J. Samuelsen R. Glucksman L. Schwartz MTA New York City Transit reinstituted front door boarding and fare collection on local buses on August 31st,, ending a short term, stop-gap measure where customers boarded from bus rear doors, put in place to help safeguard employees and customers from health risks. Protective barriers around bus operators were installed on more than 5,800 buses, allowing front door boarding and fare collection to resume safely. The change increases bus capacity by 40 percent for enhanced social distancing. Additionally, the white safety line on the bus floor that riders should stand behind was pushed back to provide more distance between the operator and customers. New York City Transit and Bus Committee Meeting Wednesday, 9/23/2020 10:00 AM - 5:00 PM ET 2 Broadway 20th Floor Board Room New York, NY 10004 1. PUBLIC COMMENT PERIOD 2. SUMMARY OF ACTIONS Summary of Actions - Page 4 3. APPROVAL OF MINUTES – July 2020 Minutes - Page 5 4. COMMITTEE WORK PLAN Work Plan September 2020 - Page 6 5. PRESIDENT'S REPORT a. Customer Service Report i. Subway Report Subway Report (August Data) - Page 14 Subway Report (July Data) - Page 41 ii. NYCT, MTA Bus Reports Bus Report (August Data) - Page 66 Bus Report (July Data) - Page 82 iii. Paratransit Report Paratransit Report (July Data) - Page 96 Paratransit Report (June Data) - Page 110 iv. -
Manhattan Bus Map
Manhattan Bus Map Bx7 to Address Locator 1 Riverdale/263 St via Riverdale Av Manhattan Bus Routes BRIDGE To locate an avenue address, cancel BROADWAY BRIDGE Bx20 to 9 M1 Harlem - Soho the last figure, divide by 2, then add HENRY HUDSON A Riverdale/246 St V via Henry Washington Heights - East Village or subtract the key number below. Hudson Pkwy M2 The answer is the nearest numbered INWOOD HILL BAKER FIELD 100 NATURE CENTER M3 Fort George - East Village cross street, approximately. M4 The Cloisters - E 32 St To find addresses on numbered cross streets, remember that INWOOD W 215 ST M5 GW Bridge - Midtown numbers increase east or west from HILL Bx 1 215 St PARK Inwood 7 M7 Harlem - 14th Street 5 Avenue, which runs north-south. Bx ISHAM 20 West Village - East Village PARK M8 Avenue A . add 3 ISHAM ST M9 Battery Park City - Kips Bay Avenue B . add 3 A Inwood-207 St W 207 ST Avenue C . add 3 TENTH AV TENTH M10 Harlem - Columbus Circle DYCKMAN HOUSE UNIVERSITY Avenue D . add 3 E Bx Bx HEIGHTS 20 12 M11 Riverbank Park - West Village 1 Avenue . add 3 W 204 ST Bx BRIDGE 12 SBS 2 Avenue . add 3 1 M12 Columbus Circle - Abingdon Square 207 St Bx12 to Bay 3 Avenue . add 10 Plaza via M14A SBS Lower E Side - Chelsea Piers Dyckman Fordham Rd and 4 Avenue . add 8 St A BROADWAY SHERMAN AV Pelham Pkwy (to DYCKMAN ST Orchard Beach M14D SBS Lower E Side - Abingdon Square 5 Avenue: THE summers only) CLOISTERS up to 200 .