Clostridioides Difficile Infection in Adults and Children
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio In
microorganisms Review The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease Spase Stojanov 1,2, Aleš Berlec 1,2 and Borut Štrukelj 1,2,* 1 Faculty of Pharmacy, University of Ljubljana, SI-1000 Ljubljana, Slovenia; [email protected] (S.S.); [email protected] (A.B.) 2 Department of Biotechnology, Jožef Stefan Institute, SI-1000 Ljubljana, Slovenia * Correspondence: borut.strukelj@ffa.uni-lj.si Received: 16 September 2020; Accepted: 31 October 2020; Published: 1 November 2020 Abstract: The two most important bacterial phyla in the gastrointestinal tract, Firmicutes and Bacteroidetes, have gained much attention in recent years. The Firmicutes/Bacteroidetes (F/B) ratio is widely accepted to have an important influence in maintaining normal intestinal homeostasis. Increased or decreased F/B ratio is regarded as dysbiosis, whereby the former is usually observed with obesity, and the latter with inflammatory bowel disease (IBD). Probiotics as live microorganisms can confer health benefits to the host when administered in adequate amounts. There is considerable evidence of their nutritional and immunosuppressive properties including reports that elucidate the association of probiotics with the F/B ratio, obesity, and IBD. Orally administered probiotics can contribute to the restoration of dysbiotic microbiota and to the prevention of obesity or IBD. However, as the effects of different probiotics on the F/B ratio differ, selecting the appropriate species or mixture is crucial. The most commonly tested probiotics for modifying the F/B ratio and treating obesity and IBD are from the genus Lactobacillus. In this paper, we review the effects of probiotics on the F/B ratio that lead to weight loss or immunosuppression. -

DC Console Using DC Console Application Design Software
DC Console Using DC Console Application Design Software DC Console is easy-to-use, application design software developed specifically to work in conjunction with AML’s DC Suite. Create. Distribute. Collect. Every LDX10 handheld computer comes with DC Suite, which includes seven (7) pre-developed applications for common data collection tasks. Now LDX10 users can use DC Console to modify these applications, or create their own from scratch. AML 800.648.4452 Made in USA www.amltd.com Introduction This document briefly covers how to use DC Console and the features and settings. Be sure to read this document in its entirety before attempting to use AML’s DC Console with a DC Suite compatible device. What is the difference between an “App” and a “Suite”? “Apps” are single applications running on the device used to collect and store data. In most cases, multiple apps would be utilized to handle various operations. For example, the ‘Item_Quantity’ app is one of the most widely used apps and the most direct means to take a basic inventory count, it produces a data file showing what items are in stock, the relative quantities, and requires minimal input from the mobile worker(s). Other operations will require additional input, for example, if you also need to know the specific location for each item in inventory, the ‘Item_Lot_Quantity’ app would be a better fit. Apps can be used in a variety of ways and provide the LDX10 the flexibility to handle virtually any data collection operation. “Suite” files are simply collections of individual apps. Suite files allow you to easily manage and edit multiple apps from within a single ‘store-house’ file and provide an effortless means for device deployment. -
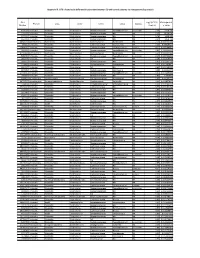
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -
Current Trends of Enterococci in Dairy Products: a Comprehensive Review of Their Multiple Roles
foods Review Current Trends of Enterococci in Dairy Products: A Comprehensive Review of Their Multiple Roles Maria de Lurdes Enes Dapkevicius 1,2,* , Bruna Sgardioli 1,2 , Sandra P. A. Câmara 1,2, Patrícia Poeta 3,4 and Francisco Xavier Malcata 5,6,* 1 Faculty of Agricultural and Environmental Sciences, University of the Azores, 9700-042 Angra do Heroísmo, Portugal; [email protected] (B.S.); [email protected] (S.P.A.C.) 2 Institute of Agricultural and Environmental Research and Technology (IITAA), University of the Azores, 9700-042 Angra do Heroísmo, Portugal 3 Microbiology and Antibiotic Resistance Team (MicroART), Department of Veterinary Sciences, University of Trás-os-Montes and Alto Douro (UTAD), 5001-801 Vila Real, Portugal; [email protected] 4 Associated Laboratory for Green Chemistry (LAQV-REQUIMTE), University NOVA of Lisboa, 2829-516 Lisboa, Portugal 5 LEPABE—Laboratory for Process Engineering, Environment, Biotechnology and Energy, Faculty of Engineering, University of Porto, 420-465 Porto, Portugal 6 FEUP—Faculty of Engineering, University of Porto, 4200-465 Porto, Portugal * Correspondence: [email protected] (M.d.L.E.D.); [email protected] (F.X.M.) Abstract: As a genus that has evolved for resistance against adverse environmental factors and that readily exchanges genetic elements, enterococci are well adapted to the cheese environment and may reach high numbers in artisanal cheeses. Their metabolites impact cheese flavor, texture, Citation: Dapkevicius, M.d.L.E.; and rheological properties, thus contributing to the development of its typical sensorial properties. Sgardioli, B.; Câmara, S.P.A.; Poeta, P.; Due to their antimicrobial activity, enterococci modulate the cheese microbiota, stimulate autoly- Malcata, F.X. -
Clostridium Difficile Infection: How to Deal with the Problem DH INFORMATION RE ADER B OX
Clostridium difficile infection: How to deal with the problem DH INFORMATION RE ADER B OX Policy Estates HR / Workforce Commissioning Management IM & T Planning / Finance Clinical Social Care / Partnership Working Document Purpose Best Practice Guidance Gateway Reference 9833 Title Clostridium difficile infection: How to deal with the problem Author DH and HPA Publication Date December 2008 Target Audience PCT CEs, NHS Trust CEs, SHA CEs, Care Trust CEs, Medical Directors, Directors of PH, Directors of Nursing, PCT PEC Chairs, NHS Trust Board Chairs, Special HA CEs, Directors of Infection Prevention and Control, Infection Control Teams, Health Protection Units, Chief Pharmacists Circulation List Description This guidance outlines newer evidence and approaches to delivering good infection control and environmental hygiene. It updates the 1994 guidance and takes into account a national framework for clinical governance which did not exist in 1994. Cross Ref N/A Superseded Docs Clostridium difficile Infection Prevention and Management (1994) Action Required CEs to consider with DIPCs and other colleagues Timing N/A Contact Details Healthcare Associated Infection and Antimicrobial Resistance Department of Health Room 528, Wellington House 133-155 Waterloo Road London SE1 8UG For Recipient's Use Front cover image: Clostridium difficile attached to intestinal cells. Reproduced courtesy of Dr Jan Hobot, Cardiff University School of Medicine. Clostridium difficile infection: How to deal with the problem Contents Foreword 1 Scope and purpose 2 Introduction 3 Why did CDI increase? 4 Approach to compiling the guidance 6 What is new in this guidance? 7 Core Guidance Key recommendations 9 Grading of recommendations 11 Summary of healthcare recommendations 12 1. -

Unix (And Linux)
AWK....................................................................................................................................4 BC .....................................................................................................................................11 CHGRP .............................................................................................................................16 CHMOD.............................................................................................................................19 CHOWN ............................................................................................................................26 CP .....................................................................................................................................29 CRON................................................................................................................................34 CSH...................................................................................................................................36 CUT...................................................................................................................................71 DATE ................................................................................................................................75 DF .....................................................................................................................................79 DIFF ..................................................................................................................................84 -

5 Command Line Functions by Barbara C
ADAPS: Chapter 5. Command Line Functions 5 Command Line Functions by Barbara C. Hoopes and James F. Cornwall This chapter describes ADAPS command line functions. These are functions that are executed from the UNIX command line instead of from ADAPS menus, and that may be run manually or by automated means such as “cron” jobs. Most of these functions are NOT accessible from the ADAPS menus. These command line functions are described in detail below. 5.1 Hydra Although Hydra is available from ADAPS at the PR sub-menu, Edit Time Series Data using Hydra (TS_EDIT), it can also be started from the command line. However, to start Hydra outside of ADAPS, a DV or UV RDB file needs to be available to edit. The command is “hydra rdb_file_name.” For a complete description of using Hydra, refer to Section 4.5.2 Edit Time-Series Data using Hydra (TS_EDIT). 5.2 nwrt2rdb This command is used to output rating information in RDB format. It writes RDB files with a table containing the rating equation parameters or the rating point pairs, with all other information contained in the RDB comments. The following arguments can be used with this command: nwrt2rdb -ooutfile -zdbnum -aagency -nstation -dddid -trating_type -irating_id -e (indicates to output ratings in expanded form; it is ignored for equation ratings.) -l loctzcd (time zone code or local time code "LOC") -m (indicates multiple output files.) -r (rounding suppression) Rules • If -o is omitted, nwrt2rdb writes to stdout; AND arguments -n, -d, -t, and -i must be present. • If -o is present, no other arguments are required, and the program will use ADAPS routines to prompt for them. -

An Attribute- Grammar Compiling System Based on Yacc, Lex, and C Kurt M
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Digital Repository @ Iowa State University Computer Science Technical Reports Computer Science 12-1992 Design, Implementation, Use, and Evaluation of Ox: An Attribute- Grammar Compiling System based on Yacc, Lex, and C Kurt M. Bischoff Iowa State University Follow this and additional works at: http://lib.dr.iastate.edu/cs_techreports Part of the Programming Languages and Compilers Commons Recommended Citation Bischoff, Kurt M., "Design, Implementation, Use, and Evaluation of Ox: An Attribute- Grammar Compiling System based on Yacc, Lex, and C" (1992). Computer Science Technical Reports. 23. http://lib.dr.iastate.edu/cs_techreports/23 This Article is brought to you for free and open access by the Computer Science at Iowa State University Digital Repository. It has been accepted for inclusion in Computer Science Technical Reports by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Design, Implementation, Use, and Evaluation of Ox: An Attribute- Grammar Compiling System based on Yacc, Lex, and C Abstract Ox generalizes the function of Yacc in the way that attribute grammars generalize context-free grammars. Ordinary Yacc and Lex specifications may be augmented with definitions of synthesized and inherited attributes written in C syntax. From these specifications, Ox generates a program that builds and decorates attributed parse trees. Ox accepts a most general class of attribute grammars. The user may specify postdecoration traversals for easy ordering of side effects such as code generation. Ox handles the tedious and error-prone details of writing code for parse-tree management, so its use eases problems of security and maintainability associated with that aspect of translator development. -

Methicillin-Resistant Staphylococcus Aureus (MRSA)
Methicillin-Resistant Staphylococcus Aureus (MRSA) Over the past several decades, the incidence of resistant gram-positive organisms has risen in the United States. MRSA strains, first identified in the 1960s in England, were first observed in the U.S. in the mid 1980s.1 Resistance quickly developed, increasing from 2.4% in 1979 to 29% in 1991.2 The current prevalence for MRSA in hospitals and other facilities ranges from <10% to 65%. In 1999, MRSA accounted for more than 50% of all Staphylococcus aureus isolates within U.S. intensive care units.3, 4 The past years, however, outbreaks of MRSA have also been seen in the community setting, particularly among preschool-age children, some of whom have attended day-care centers.5, 6, 7 MRSA does not appear to be more virulent than methicillin-sensitive Staphylococcus aureus, but certainly poses a greater treatment challenge. MRSA also has been associated with higher hospital costs and mortality.8 Within a decade of its development, methicillin resistance to Staphylococcus aureus emerged.9 MRSA strains generally are now resistant to other antimicrobial classes including aminoglycosides, beta-lactams, carbapenems, cephalosporins, fluoroquinolones and macrolides.10,11 Most of the resistance was secondary to production of beta-lactamase enzymes or intrinsic resistance with alterations in penicillin-binding proteins. Staphylococcus aureus is the most frequent cause of nosocomial pneumonia and surgical- wound infections and the second most common cause of nosocomial bloodstream infections.12 Long-term care facilities (LTCFs) have developed rates of MRSA ranging from 25%-35%. MRSA rates may be higher in LTCFs if they are associated with hospitals that have higher rates.13 Transmission of MRSA generally occurs through direct or indirect contact with a reservoir. -

Clostridioides Difficileinfections
bioMérieux In vitro diagnostics serving CLOSTRIDIOIDES public health DIFFICILE INFECTIONS A major player in in vitro diagnostics for more than 50 years, From Diagnosis to bioMérieux has always been driven by a pioneering spirit and unrelenting commitment to improve public health worldwide. Outbreak Management Our diagnostic solutions bring high medical value to healthcare professionals, providing them with the most relevant and reliable information, as quickly as possible, to support treatment decisions and better patient care. bioMérieux’s mission entails a commitment to support medical education, by promoting access to diagnostic knowledge for as many people as possible. Focusing on the medical value of diagnostics, our collection of educational booklets aims to raise awareness of the essential role that diagnostic test results play in healthcare decisions. Other educational booklets are available. Consult your local bioMérieux representative. The information in this booklet is for educational purposes only and is not intended to be exhaustive. It is not intended to be a substitute for professional medical advice. Always consult a medical director, physician, or other qualified health provider regarding processes and/or protocols for diagnosis and treatment of a medical condition. bioMérieux assumes no responsibility or liability for any diagnosis established or treatment prescribed by the physician. bioMérieux, Inc. • 100 Rodolphe Street • Durham, NC 27712 • USA • Tel: (800) 682 2666 • Fax: (800) 968 9494 © 2019 bioMérieux, Inc. • BIOMERIEUX and the BIOMERIEUX logo, are used pending and/or registered trademarks belonging to bioMérieux, or one of its subsidiaries, or one of its companies. companies. its or one of subsidiaries, its or one of bioMérieux, belonging to trademarks registered pending and/or used are logo, and the BIOMERIEUX • BIOMERIEUX Inc. -

Complete Genome Sequences of Two Enterococcus Faecium Strains and Comparative Genomic Analysis
EXPERIMENTAL AND THERAPEUTIC MEDICINE 19: 2019-2028, 2020 Complete genome sequences of two Enterococcus faecium strains and comparative genomic analysis YONG‑QI GAN, TAO ZHANG, YONG‑QIANG GAN, ZHUANG ZHAO and BIN ZHU Guangxi Institute for Food and Drug Control, Nanning, Guangxi Zhuang Autonomous Region 530021, P.R. China Received December 1, 2018; Accepted August 12, 2019 DOI: 10.3892/etm.2020.8447 Abstract. Enterococci are used for improvement of the intes- environment when treating bacterial diarrhea (3). There are tinal environment and have clinical benefits. Enterococcus two main advantages to Enterococcus that make it the most faecalis and Enterococcus faecium have similar morpholo- popular edible probiotic in animals and humans: i) In the gies, leading to confusion between the two species. In order gastrointestinal (GI) tract, Enterococcus competes with patho- to identify the National Institute for Food and Drug Control gens and thus decreases their virulence (2); ii) Enterococcus (strain 140623) and Shin Biofermin S (strain SBS-1, one of resists acid stress and cannot be digested by GI‑secreted diges- the cocci), which are widely used clinically, the present study tive juice (4). E. faecalis and E. faecium are used as digestive sequenced and analyzed these two strains. The biochemical agents for the treatment of diarrhea caused by flatulence characteristics, gas chromatography and mass spectrometry and indigestion (2). However, these two bacteria are difficult results of 140623 and SBS-1 revealed that the two strains were to distinguish morphologically. Species identification and more similar to E. faecium than E. faecalis. The genomes of genome characterization of these strains may elucidate thera- 140623 and SBS-1 contained 2,812,926 bp and 2,797,745 bp, peutic strategies for bacterial infection and probiotic treatment respectively, based on Illumina HiSeq 2000 sequencing. -

Staphylococcus Aureus Kentaro Iwata1*, Asako Doi2, Takahiko Fukuchi1, Goh Ohji1, Yuko Shirota3, Tetsuya Sakai4 and Hiroki Kagawa5
Iwata et al. BMC Infectious Diseases 2014, 14:247 http://www.biomedcentral.com/1471-2334/14/247 RESEARCH ARTICLE Open Access A systematic review for pursuing the presence of antibiotic associated enterocolitis caused by methicillin resistant Staphylococcus aureus Kentaro Iwata1*, Asako Doi2, Takahiko Fukuchi1, Goh Ohji1, Yuko Shirota3, Tetsuya Sakai4 and Hiroki Kagawa5 Abstract Background: Although it has received a degree of notoriety as a cause for antibiotic-associated enterocolitis (AAE), the role of methicillin resistant Staphylococcus aureus (MRSA) in the pathogenesis of this disease remains enigmatic despite a multitude of efforts, and previous studies have failed to conclude whether MRSA can cause AAE. Numerous cases of AAE caused by MRSA have been reported from Japan; however, due to the fact that these reports were written in the Japanese language and a good portion lacked scientific rigor, many of these reports went unnoticed. Methods: We conducted a systematic review of pertinent literatures to verify the existence of AAE caused by MRSA. We modified and applied methods in common use today and used a total of 9 criteria to prove the existence of AAE caused by Klebsiella oxytoca. MEDLINE/Pubmed, Excerpta Medica Database (EMBASE), the Cochrane Database of Systematic Reviews, and the Japan Medical Abstract Society database were searched for studies published prior to March 2013. Results: A total of 1,999 articles were retrieved for evaluation. Forty-five case reports/series and 9 basic studies were reviewed in detail. We successfully identified articles reporting AAE with pathological and microscopic findings supporting MRSA as the etiological agent. We also found comparative studies involving the use of healthy subjects, and studies detecting probable toxins.