Sentinel Surveillance Report and Epidemiology Studies Will Guide the Department for Taking Various Measures and It Will Also Give Information to All
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Accused Persons Arrested in Kottayam District from 08.09.2019To14.09.2019
Accused Persons arrested in Kottayam district from 08.09.2019to14.09.2019 Name of Name of the Name of the Place at Date & Arresting Court at Sl. Name of the Age & Cr. No & Sec Police father of Address of Accused which Time of Officer, which No. Accused Sex of Law Station Accused Arrested Arrest Rank & accused Designation produced 1 2 3 4 5 6 7 8 9 10 11 Palambadam Cr:1152/19 U/s Mundakayam 08.09.19 Shibukumar V , 1 Eappen Abraham 64 House,Kalathilpadi 15 © r/w 63 of Mundakayam Station Bail Byepass 12.40 Hrs IP SHO Jn,Vijayapuram Village Abkari Act Arangattu House, Cr:1152/19 U/s Near Hospital, Mundakayam 08.09.19 Shibukumar V , 2 Jacob James 52 15 © r/w 63 of Mundakayam Station Bail Collectrate P O, Byepass 12.40 Hrs IP SHO Abkari Act Muttambalam Vaniyapurackal Cr:1153/19 U/s Mundakayam 08.09.19 Shibukumar V , 3 Anil Mathew Mathew 52 House,Changanasseri 15 © r/w 63 of Mundakayam Station Bail Byepass 13.05 Hrs IP SHO P O,Changanasseri Abkari Act Cr:1153/19 U/s Kunnukattu Mundakayam 08.09.19 Shibukumar V , 4 Joy Saimon 69 15 © r/w 63 of Mundakayam Station Bail House,Changanassery Byepass 13.05 Hrs IP SHO Abkari Act Mathichiparambil Cr:1153/19 U/s Mundakayam 08.09.19 Shibukumar V , 5 Mathew John 59 House,, Chethippuzha, 15 © r/w 63 of Mundakayam Station Bail Byepass 13.05 Hrs IP SHO Cheeranchira Abkari Act Padiyara Cr:1153/19 U/s House,vazhappally Mundakayam 08.09.19 Shibukumar V , 6 JoJo Padiyara Joseph 49 15 © r/w 63 of Mundakayam Station Bail East Bhagom, Byepass 13.05 Hrs IP SHO Abkari Act Changanasseri Puthupparambil Cr:1157/19 U/s 08.09.19 KJ Mammmen, 7 Biju P Soman Soman 31 House, Thalunkal P O, Mundakayam 118(a) of KP Mundakayam Station Bail 20.35 Hrs GSI Koottickal Act Puthenplackal Cr:1158/19 U/s House,Vallakadu 08.09.19 KJ Mammmen, 8 Jeevan Binoy Thomas 45 Mundakayam 279 IPC & 185 Mundakayam Station Bail bhagom,Yendayar, 23.30 Hrs GSI MV Act Koottickal Poothakuzhiyil House,Punchavayal P Cr: 1163/19 JFMC Satheesh 10.09.19 KJ Mammmen, 9 Chellappan 39 O,504 Colony, 504 Colony U/s 55(A)1 of Mundakayam KANJIRAPPALL Kumar 16.35 Hrs GSI Ayyankaly Jn. -

Particulars of Some Temples of Kerala Contents Particulars of Some
Particulars of some temples of Kerala Contents Particulars of some temples of Kerala .............................................. 1 Introduction ............................................................................................... 9 Temples of Kerala ................................................................................. 10 Temples of Kerala- an over view .................................................... 16 1. Achan Koil Dharma Sastha ...................................................... 23 2. Alathiyur Perumthiri(Hanuman) koil ................................. 24 3. Randu Moorthi temple of Alathur......................................... 27 4. Ambalappuzha Krishnan temple ........................................... 28 5. Amedha Saptha Mathruka Temple ....................................... 31 6. Ananteswar temple of Manjeswar ........................................ 35 7. Anchumana temple , Padivattam, Edapalli....................... 36 8. Aranmula Parthasarathy Temple ......................................... 38 9. Arathil Bhagawathi temple ..................................................... 41 10. Arpuda Narayana temple, Thirukodithaanam ................. 45 11. Aryankavu Dharma Sastha ...................................................... 47 12. Athingal Bhairavi temple ......................................................... 48 13. Attukkal BHagawathy Kshethram, Trivandrum ............. 50 14. Ayilur Akhileswaran (Shiva) and Sri Krishna temples ........................................................................................................... -
List of Lacs with Local Body Segments (PDF
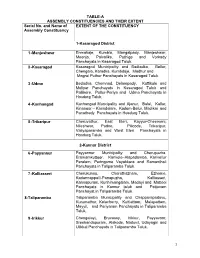
TABLE-A ASSEMBLY CONSTITUENCIES AND THEIR EXTENT Serial No. and Name of EXTENT OF THE CONSTITUENCY Assembly Constituency 1-Kasaragod District 1 -Manjeshwar Enmakaje, Kumbla, Mangalpady, Manjeshwar, Meenja, Paivalike, Puthige and Vorkady Panchayats in Kasaragod Taluk. 2 -Kasaragod Kasaragod Municipality and Badiadka, Bellur, Chengala, Karadka, Kumbdaje, Madhur and Mogral Puthur Panchayats in Kasaragod Taluk. 3 -Udma Bedadka, Chemnad, Delampady, Kuttikole and Muliyar Panchayats in Kasaragod Taluk and Pallikere, Pullur-Periya and Udma Panchayats in Hosdurg Taluk. 4 -Kanhangad Kanhangad Muncipality and Ajanur, Balal, Kallar, Kinanoor – Karindalam, Kodom-Belur, Madikai and Panathady Panchayats in Hosdurg Taluk. 5 -Trikaripur Cheruvathur, East Eleri, Kayyur-Cheemeni, Nileshwar, Padne, Pilicode, Trikaripur, Valiyaparamba and West Eleri Panchayats in Hosdurg Taluk. 2-Kannur District 6 -Payyannur Payyannur Municipality and Cherupuzha, Eramamkuttoor, Kankole–Alapadamba, Karivellur Peralam, Peringome Vayakkara and Ramanthali Panchayats in Taliparamba Taluk. 7 -Kalliasseri Cherukunnu, Cheruthazham, Ezhome, Kadannappalli-Panapuzha, Kalliasseri, Kannapuram, Kunhimangalam, Madayi and Mattool Panchayats in Kannur taluk and Pattuvam Panchayat in Taliparamba Taluk. 8-Taliparamba Taliparamba Municipality and Chapparapadavu, Kurumathur, Kolacherry, Kuttiattoor, Malapattam, Mayyil, and Pariyaram Panchayats in Taliparamba Taluk. 9 -Irikkur Chengalayi, Eruvassy, Irikkur, Payyavoor, Sreekandapuram, Alakode, Naduvil, Udayagiri and Ulikkal Panchayats in Taliparamba -
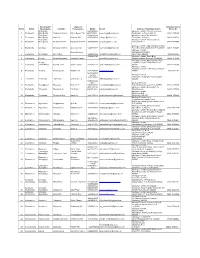
Sl.No. Block Location Mobile E-Mail Address of Akshaya Centre 1 Erattupetta Chennadu Kavala Sajida Beevi. T.M [email protected]
Panchayath/ Name of Akshaya Centre Sl.No. Block Municipality Location Entrepreneur Mobile E-mail Address of Akshaya Centre Phone No Erattupetta 9961985088, Akshaya e centre, Chennadu Kavala, 1 Erattupetta Municipality Chennadu Kavala Sajida Beevi. T.M 9447507691, [email protected] Erattupetta, Kottayam-686121 04822-275088 Erattupetta 9446923406, Akshaya e centre, Nadackal P O, 2 Erattupetta Municipality Hutha Jn. Shaheer PM 9847683049 [email protected] Erattupetta, Kottayam 04822-329714 Erattupetta Akshaya e centre, Thottumukku Jn., 3 Erattupetta Municipality Thottumukku Jn. Rasiya M Shereef 9847095886 [email protected] Erattupetta P O 04828-277550 Akshaya e centre, Opp. Melukavumattom 4 Erattupetta Melukavu Melukavu Mattom Anoop Mohan 9447515722 [email protected] Post office,Melukavumattom P O,686652 04822-220402 Akshaya e-centre, Minimol Antony Punnathaniyil Building 5 Erattupetta Moonnilavu Moonnilavu 9446861799 [email protected] Moonnilavu-686596 48222-86266 9745402710 Akshaya e centre, Chalil Bldg, 6 Erattupetta Poonjar Panachikkappara Aniamma Suresh [email protected] Panachikkapara, Poonjar P O-686581 04822-276506 Akshaya e centre, Panchayathu office Poonjar Complex,Poonjar Thekkekkara P O- 7 Erattupetta Thekkekkara Poonjar Town Shymol Jacob 9745402710 [email protected] 686582 04822-276506 Akshaya e centre, Panchayat Junction, Theekoy, Kottayam- 8 Erattupetta Teekkoy Panchayat Jn. Sulfath K H 9400233778 [email protected] 686581 48222-81145 9847093283 Suresh- Akshaya e-centre, 8547672267 Thalanadu, Thalanadu -

Agenda and Notes of the Meeting of the Rta Kottayam Dated 30/11/2017
1 AGENDA AND NOTES OF THE MEETING OF THE RTA KOTTAYAM DATED 30/11/2017. Item No - 01 G1/109928/2017/K Agenda-To consider the application for the grant of fresh regular permit to SC KL 34 C 1427 / another suitable vehicle to operate on the route KUZHIMAVU – ERUMELY Via, Koruthodu, Panackachira, Vandanpathal, Mundakayam, Kannimala, Pulikkunnu, Kottaramkada as Ordinary Service Applicant- Sri. Binu P S, Pazhoor [H], Palampra P.O., Kanjirappally. Proposed Timings Kuzhimavu Mundakayam Erumely A D A D A D 6.05[S] 6.43 7.00 7.33 8.16 7.43 9.20 8.42 9.30 10.08 11.03 10.25 11.20 11.58 12.40 1.13 2.36 2.03 3.09 3.42 4.53 4.20 5.35 6.08 6.58 6.25 7.55 [H] 7.17 Notes- This is an application for the grant of a of a fresh regular permit to SC KL 34 C 1427 / another suitable vehicle to operate on the route KUZHIMAVU – ERUMELY Via, Koruthodu, Panackachira, Vandanpathal, Mundakayam, Kannimala, Pulikkunnu, Kottaramkada as Ordinary Service. The enquiry report of MVI Kanjirappally revealed the following. 1. Total distance of the route : 28.2 Kms. 2. Intra/ Inter District route : Intra District. 3. Details of Virgin Portion : Nil 2 4. Details of Road Fitness certificate : N.A. 5. Details of Overlapping : Total overlapping is 150 meter ie, 0.53 % of the total route length [28.2 km] which is within the permissible limit. 1) Route portion of 150 meter from Mundakayam B S Jn. -
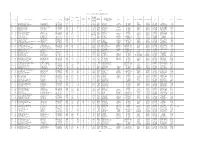
Sheet1 Page 1 LIST of SCHOOLS in KOTTAYAM DISTRICT 10 Sl. No
Sheet1 LIST OF SCHOOLS IN KOTTAYAM DISTRICT No of Students HS/HSS/ Year of VHSS/H Name of Panch- Std. Std. Boys/ 10 Sl. No. Name of School Address with Pincode Phone No Establishm SS ayat /Muncipality/ Block Taluk Name of Parliament Name of Assembly DEO AEO MGT Remarks (From) (To) Girls/ Mixed ent Boys Girls &VHSS/ Corporation TTI 10 1 Areeparambu Govt. HSS Areeparambu P.O. 0481-2700300 1905 42 36 I XII HSS Mixed Manarcadu Pallam Kottayam Err:514 Err:514 Kottayam Pampady Govt 10 2 Arpookara Medical College VHSS Gandhinagar P.O. 0481-2597401 1966 73 33 V XII HSS&VHSS Mixed Arpookara Ettumanoor Kottayam Err:514 Err:514 Kottayam Kottayam West Govt 10 3 Changanacherry Govt. HSS Changanacherry P.O. 0481-2420748 1871 43 23 V XII HSS Mixed Changanacherry ( M ) Changanacherry Err:514 Err:514 Kottayam Changanassery Govt 10 4 Chengalam Govt. HSS Chengalam South P.O. 0481-2524828 1917 127 107 I XII HSS Mixed Thiruvarpu Pallam Kottayam Err:514 Err:514 Kottayam Kottayam West Govt 10 5 Karapuzha Govt. HSS Karapuzha P.O. 0481-2582936 1895 56 34 I XII HSS Mixed Kottayam( M ) Kottayam Err:514 Err:514 Kottayam Kottayam West Govt 10 6 Karipputhitta Govt. HS Arpookara P.O. 0481-2598612 1915 74 44 I X HS Mixed Arpookara Ettumanoor Kottayam Err:514 Err:514 Kottayam Kottayam West Govt 10 7 Kothala Govt. VHSS S.N. Puram P.O. 0481-2507726 1912 48 64 I XII VHSS Mixed Kooroppada Pampady Kottayam Err:514 Err:514 Kottayam Pampady Govt 10 8 Kottayam Govt. -

Diocese of Kottayam
THE MALANKARA SYRIAN CHRISTIAN ASSOCIATION List of Members 2017- 2022 Diocese : KOTTAYAM Sl. Name of the Name & Address of the Age Remarks No. Parish Church representatives KTM-01/01 01 Amayannoor Rev.Fr. Kuriakose V. Mani 37 Kazhunnuvalam Vettathu (H), Pangada P.O., Methranchery St.Thomas Via. Pampady, Kottayam 686 502. Mob: 9447623293 KTM-01/02 Sri. Mathew P. Mathew 57 Valleeparampil House, Amayannoor P.O., Kottayam 686019. Mob: 9526856947 KTM-01/03 Sri. P.I. Mathew 57 Alackapparambil House, Amayannoor P.O., Kottayam 686019. Mob: 9447756042 KTM-01/04 Sri. Thomas Stephen 56 Mavelil House, Puthuppally P.O., Kottayam 686011. Mob: 9447119644 KTM-02/01 02 Amayannoor Rev.Fr. Kurian Kuriakose 33 Karattukunnel St.Mary’s Puthenkandathil (Akkara) S.N. Puram P.O., Pampady, Kottayam 686 502. KTM-02/02 Sri. Sleeba C. Abraham 43 Cheriyil House, Amayannoor P.O. Kottayam. KTM-02/03 Sri. P.M. Kuriakose 58 FINALPurankavil House, LIST Amayannoor P.O. Kottayam. KTM-02/04 Sri. P.V. Thomas 62 Puthenparambil House, Thiruvanchoor P.O., Kottayam. KTM-03/01 03 Areeparambu St.George Rev. Fr. Varghese Jacob Pacheril (H), 40 Amayannoor P.O., Kottayam 686 564. 2 KTM-03/02 Sri. P.T. Kuruvila 57 Puliyayil House, Areeparampu P.O., Kottayam 686501. Mob: 9846697369 KTM-03/03 Sri. P.S. Georgekutty 62 Palliyampil House, Areeparampu P.O., Kottayam 686501. Mob: 9446071331 KTM-04/01 04 Anicadu Mar Gregorios Rev.Fr. Mathew P. Kurian Parackal, Pongamthanam P.O., Kottayam 686 538. Mob: 9946799502, 8281830607 KTM-04/02 Sri. Manu Tom Jacob 41 Poovathumkal House, Anicadu P.O., Kayoori, Kottayam 686503. -

Agenda for the Meeting of Rta Kottayam Scheduled to Be Held on 08.02.2019 at Collectorate Conference Hall, Civil Station, Kottayam
1 AGENDA FOR THE MEETING OF RTA KOTTAYAM SCHEDULED TO BE HELD ON 08.02.2019 AT COLLECTORATE CONFERENCE HALL, CIVIL STATION, KOTTAYAM. ******************************************************************************************** Item No : 01 G1/em 744/2018/K Agenda:- To consider the direction of the Transport Commissioner, Thiruvananthapuram for giving delegation of power under Rule 133 of KMV Rules to the Secretaries of RTAs for issuing permits to KSRTC, on their applications submitted along with current records of the vehicles, on the notified routes. Ref:-Letter NO D3/25536/STA/2014 dtd 21.11.2018 of Transport Commissioner, Thiruvananthapuram. ************************************************************************************************ Item No: 02 G1/em 417/2018/K Agenda:- To consider the recommendation of the Traffic Committee Meeting of Kanjirappally Grama Panchayat for the implementation of traffic reforms at Kanjirappally Pettah Jn. Ref:- Decision number 6(1) in the minutes of the meeting of Kanjirappally Grama Panchayat held on 29.09.2018. ************************************************************************************************ Item No: 03 G1/6072/2018/K Agenda:- To consider the complaint filed against the unauthorized Bus Shelter erected at Mundangal Jn. on Pala – Thodupuzha route. Complainant : Smt. Mili Alex, Katankavil, Mundankal P.O. **************************************************************************************************** Item No: 04 G1/12845/2018/K Agenda:-To consider the proposal for Bus Stop at Meladukkam -

Kottayam District Disaster Management Plan
District Disaster Management Plan, 2015 Kottayam District Disaster Management Plan Published under Section 30 (2) (i) of the Disaster Management Act, 2005 (Central Act 53 of 2005) District Disaster Management Plan 2015 30th July 2016; Pages: 136 District This document is for official purposes only. All reasonable precautions have been taken by the District Disaster Management Authority to verify the information and ensure stakeholder consultation and inputs prior to publication of this document. The publisher welcomes suggestions for improved future editions. District Disaster Management Plan – KOTTAYAM 2015 CONTENTS INTRODUCTION ......................................................................................................................................................................... 4 1.1 VISION ............................................................................................................................................................................................ 4 1.2 MISSION ........................................................................................................................................................................................ 4 1.3 POLICY ........................................................................................................................................................................................... 4 1.4 OBJECTIVES OF THE PLAN ................................................................................................................................................ -

Deputy Director of Panchayaths, Kottayam
Deputy Director of Panchayaths, Kottayam. Sub: Establishment-Panchayath Department-Kottayam District-General Transfer 2008-Transfer and postings-order issued. Read : 1.G.O(M.S) No. 105/07/LSGD dated 4/4/07 2. G.O.(M.S) NO. 54/08/LSGD dated 3/3/08 3.This office Order No. Dated E2/880/08(1) dated 24/4/08. Order No. E2/880/08(1) Dated 29/5/08 As per this office order read as 3rd a draft list of transfer and postings of the U.D.Clerk, L.D.Clerk and Librarians as part of General Transfer 2008 was published inviting objections in view of the guidelines issued by Government vide G.O read as 1st and 2nd. The objections received in response to the Draft list within the time limit has examined in detail. Having considering its merit necessary modifications is made and accordingly the draft list is finalised as follows. The following incumbents are transferred and posted in the offices noted against their name with immediate effect. The incumbents who had submitted applications seeking transfer under general transfer 2008 and could not be considered for want of vacancies shall be arranged in the order of seniority and those vacancies that may arise in between two general transfers will be filled up from this queue list. This queue list in this regard is published in this office. The head of office concerned will give effect to this order forthwith and report the date of relief and joining duty of the incumbents to this office and to all concerned promptly. -

Master Plan for Sabarimala Regional Module IL&FS Ecosmart
Master Plan for Sabarimala Regional Module MASTER PLAN MODULES REGIONAL MODULE 1. BACKGROUND ......................................................................................................................1 1.1 Introduction and Relevance....................................................................................................1 1.2 Aims and Objectives ................................................................................................................2 1.3 Methodology.............................................................................................................................2 1.4 Scope of the Study....................................................................................................................3 1.5 Structure of the Report ...........................................................................................................3 2. PLANNING REGION FOR REGIONAL PLANNING.......................................................4 2.1 Introduction..............................................................................................................................4 2.2 Planning Region .......................................................................................................................5 2.2.1 Description of Outlined Planning Regions ................................................................................5 2.2.2 Components of Study in Wider Planning Regions......................................................................6 2.3 Planning Time Frames -
Guidelines and List of Officials for AUG 2014 Admission Closing
ADMISSION CLOSING LIST OF OFFICIALS 2014 AUGUST Sl No of ITI Dist Code District NAME OF INSTITUTES GOVT ITI /OFFICE NAME OF OFFICAL DESIGNATION 1 1 TVPM BETHANY PRIVATE ITI, KALLAMPARA, NEDUMANGAD ARYANAD JOJO K.L SENIOR SUPERINTENDENT 2 1 TVPM BVDM PRIVATE ITI, CHULLIMANOOR ARYANAD JOJO K.L SENIOR SUPERINTENDENT 3 1 TVPM MEERA PRIVATE ITI, KARIPUR,NEDUMANGAD ARYANAD JOJO K.L SENIOR SUPERINTENDENT 4 1 TVPM MITHRANEKETHAN PRIVATE ITI,VELLANAD ARYANAD JOJO K.L SENIOR SUPERINTENDENT NET ENGINEERING TECHNOLOGY PRIVATE ITI, 5 1 TVPM NEDUMANGAD ARYANAD JOJO K.L SENIOR SUPERINTENDENT KERALA INSTITUTE OF TECHNOLOGY PRIVATE ITI, 6 1 TVPM VEDIVACHANCOVIL ARYANAD JOJO K.L SENIOR SUPERINTENDENT K.K.P.M PRIVATE ITI, MARUTHINAKAM, MANCHA, 7 1 TVPM NEDUMANGAD, THIRUVANANTHAPURAM ARYANAD SUDHA SHANKAR PRINCIPAL CLASS-II KALLUR KASSIM PILLAI MEMORIAL PRIVATE ITI, 8 1 TVPM NEDUMANGAD ARYANAD SUDHA SHANKAR PRINCIPAL CLASS-II QUAIDE A MILLATH PRIVATE ITI(QAM PRIVATE ITI) 9 1 TVPM KOCHUKARIKKAKOM, DAIVAPPURA P.O, PERINGAMALA ARYANAD SUDHA SHANKAR PRINCIPAL CLASS-II 10 1 TVPM SALVATION ARMY VTC PRIVATE ITI, NEDUMAGAD ARYANAD SUDHA SHANKAR PRINCIPAL CLASS-II 11 1 TVPM GURUDEV PRIVATE ITI, KILIMANOOR ATTINGAL SALEEMUDEEN A SENIOR SUPERINTENDENT 12 1 TVPM JAMIUL KHAIRATH PRIVATE ITI, ATTINGAL ATTINGAL SALEEMUDEEN A SENIOR SUPERINTENDENT MGM PRIVATE ITI, NEAR KSEB SUBSTATION, KILIMANOOR 13 1 TVPM P.O ATTINGAL SALEEMUDEEN A SENIOR SUPERINTENDENT 14 1 TVPM PENTAGON PRIVATE ITI ATTINGAL, ATTINGAL SALEEMUDEEN A SENIOR SUPERINTENDENT 15 1 TVPM U TECH COMPUTER CENTRE