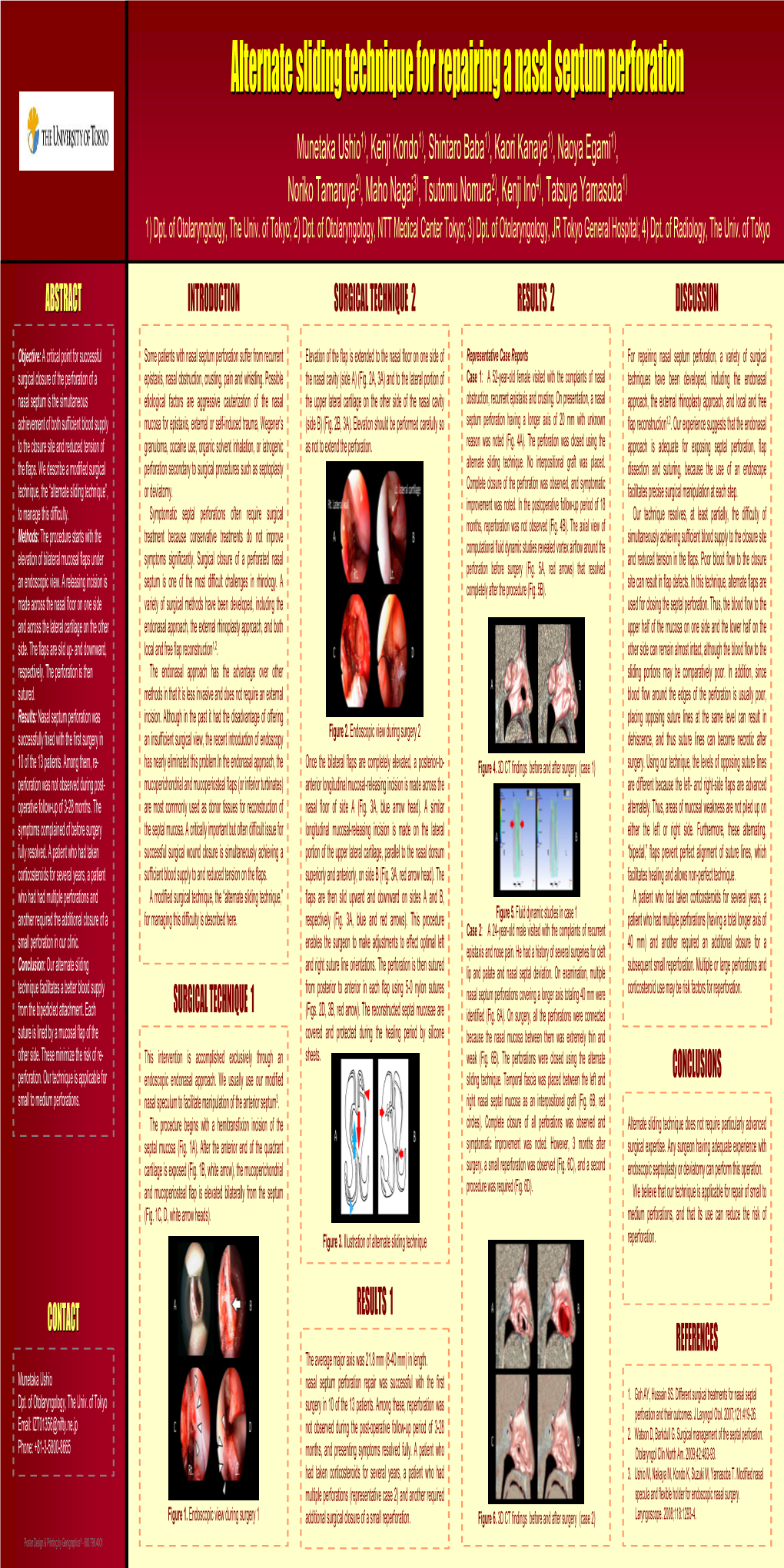
Alternate Sliding Technique for Repairing a Nasal Septum Perforation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pulmonary Cancer And/Or GPA? Diagnostic Implications of Pulmonary Nodules
Gaceta Médica de México. 2016;152 Contents available at PubMed www.anmm.org.mx PERMANYER Gac Med Mex. 2016;152:468-74 www.permanyer.com GACETA MÉDICA DE MÉXICO ORIGINAL ARTICLE Pulmonary pseucotumor in granulomatosis with polyangiitis (GPA). Pulmonary cancer and/or GPA? Diagnostic implications of pulmonary nodules Gabriel Horta-Baas1*, Esteban Meza-Zempoaltecatl2, Mario Pérez-Cristóbal2 and Barile-Fabris Leonor Adriana2 1Rheumatology Department, Hospital General Regional 220, IMSS, Toluca; 2Rheumatology Department, Hospital de Especialidades, Centro Médico Nacional Siglo XXI, IMSS, Mexico City, Mexico Abstract Granulomatosis with polyangiitis (GPA), formerly known as Wegener’s granulomatosis, is a systemic necrotizing vasculitis, which affects small and medium sized blood vessels and is often associated with cytoplasmic anti-neutrophil cytoplasmic antibodies (ANCA). Inflammatory pseudotumor is a rare condition characterized by the appearance of a mass lesion that mimics a malignant tumor both clinically and on imaging studies, but that is thought to have an inflammatory/reactive pathogenesis. We report a patient with a GPA which was originally diagnosed as malignancy. (Gac Med Mex. 2016;152:468-74) Corresponding author: Gabriel Horta-Baas, [email protected] KEY WORDS: Granulomatosis with polyangiitis. Pseudotumor. Malignancy. Introduction Presentation of the case According to the 2012 revised Chapel Hill classifica- This is the case of a 39-year old male who was tion, granulomatosis with polyangiitis (GPA), previously admitted in the hospital presenting with asthenia, gen- known as Wegener’s granulomatosis (WG), is an auto- eral malaise, intermittent fever (3 to 4 times a month), immune systemic disease of unknown etiology, charac- diaphoresis with no time of day predominance and loss terized by necrotizing granulomatous inflammation of the of 10-kg weight in 6 months. -

Rhinotillexomania in a Cystic Fibrosis Patient Resulting in Septal Perforation Mark Gelpi1*, Emily N Ahadizadeh1,2, Brian D’Anzaa1 and Kenneth Rodriguez1
ISSN: 2572-4193 Gelpi et al. J Otolaryngol Rhinol 2018, 4:036 DOI: 10.23937/2572-4193.1510036 Volume 4 | Issue 1 Journal of Open Access Otolaryngology and Rhinology CASE REPORT Rhinotillexomania in a Cystic Fibrosis Patient Resulting in Septal Perforation Mark Gelpi1*, Emily N Ahadizadeh1,2, Brian D’Anzaa1 and Kenneth Rodriguez1 1 Check for University Hospitals Cleveland Medical Center, USA updates 2Case Western Reserve University School of Medicine, USA *Corresponding author: Mark Gelpi, MD, University Hospitals Cleveland Medical Center, 11100 Euclid Avenue, Cleveland, OH 44106, USA, Tel: (216)-844-8433, Fax: (216)-201-4479, E-mail: [email protected] paranasal sinuses [1,4]. Nasal symptoms in CF patients Abstract occur early, manifesting between 5-14 years of age, and Cystic fibrosis (CF) is a multisystem disease that can have represent a life-long problem in this population [5]. Pa- significant sinonasal manifestations. Viscous secretions are one of several factors in CF that result in chronic sinona- tients with CF can develop thick nasal secretions con- sal pathology, such as sinusitis, polyposis, congestion, and tributing to chronic rhinosinusitis (CRS), nasal conges- obstructive crusting. Persistent discomfort and nasal man- tion, nasal polyposis, headaches, and hyposmia [6-8]. ifestations of this disease significantly affect quality of life. Sinonasal symptoms of CF are managed medically with Digital manipulation and removal of crusting by the patient in an attempt to alleviate the discomfort can have unfore- topical agents and antibiotics, however surgery can be seen damaging consequences. We present one such case warranted due to the chronic and refractory nature of and investigate other cases of septal damage secondary to the symptoms, with 20-25% of CF patients undergoing digital trauma, as well as discuss the importance of sinona- sinus surgery in their lifetime [8]. -

Ear-Nose-Throat Manifestations in Inflammatory Bowel Diseases ANNALS of GASTROENTEROLOGY 2007, 20(4):265-274X Xx 265X
xx xx Ear-nose-throat manifestations in Inflammatory Bowel Diseases ANNALS OF GASTROENTEROLOGY 2007, 20(4):265-274x xx 265x Review Ear-nose-throat manifestations in Inflammatory Bowel Diseases C.D. Zois, K.H. Katsanos, E.V. Tsianos going activation of the innate immune system driven by SUMMARY the presence of luminal flora. Both UC and CD have a Inflammatory bowel diseases (IBD) refer to a group of chron- worldwide distribution and are common causes of mor- ic inflammatory disorders involving the gastrointestinal tract bidity in Western Europe and northern America. and are typically divided into two major disorders: Crohn’s The extraintestinal manifestasions of IBD, however, disease (CD) and ulcerative colitis (UC). CD is characterized are not of less importance. In some cases they are the first by noncontiguous chronic inflammation, often transmural clinical manifestation of the disease and may precede the with noncaseating granuloma formation. It can involve any onset of gastrointestinal symptoms by many years, playing portion of the alimentary tract and CD inflammation has of- also a very important role in disease morbidity. As multi- ten been described in the nose, mouth, larynx and esopha- systemic diseases, IBD, have been correlated with many gus in addition to the more common small bowel and colon other organs, including the skin, eyes, joints, bone, blood, sites. UC differs from CD in that it is characterized by con- kidney, liver and biliary tract. In addition, the inner ear, tiguous chronic inflammation without transmural involve- nose and throat should also be considered as extraintesti- ment, but extraintestinal manifestations of UC have also been nal involvement sites of IBD. -

A New Classification for Septal Perforation and Effects of Treatment
Braz J Otorhinolaryngol. 2019;85(6):716---723 Brazilian Journal of OTORHINOLARYNGOLOGY www.bjorl.org ORIGINAL ARTICLE A new classification for septal perforation and effects ଝ of treatment methods on quality of life a,∗ b a Emrah Sapmaz , Yuksel Toplu , Battal Tahsin Somuk a Gaziosmanpas¸a University Medical Faculty, Department of Otorhinolaryngology, Tokat, Turkey b Inonu University Medical Faculty, Department of Otorhinolaryngology, Malatya, Turkey Received 7 March 2018; accepted 6 June 2018 Available online 17 July 2018 KEYWORDS Abstract Septal perforation Introduction: Septal perforation is a condition characterized by loss of cartilage and/or bony Quality of life; structures along with the mucoperichondrium and mucoperiosteum lining them. The etiology Septal button includes a history of nasal surgery or trauma, nose picking, bilateral septal cauterization, overuse of nasal sprays, cocaine abuse, vasculitis, and malignancies. Objective: Comparison of quality of life in patients with septal perforation after conservative or surgical treatment, and a new approach for the determination of the diameter of the perforation from a different point of view. Methods: The diameter of septal perforation, total vertical diameter of septum, and horizontal diameter of the perforation were measured in a total of 34 patients. Nineteen of the patients underwent surgical septal perforation repair, and 15 of them received septal button application. The patients were asked to complete the Glasgow Benefit Inventory quality of life questionnaire. Results: The septal perforation successfully healed in 18 of 19 patients who underwent surgi- cal treatment. The quality of life scores were statistically significantly higher in the surgical treatment group when compared to the button group (p < 0.05). -

Tests on Otorhinolaryngology
Tests on Otorhinolaryngology Part I OTOLOGY 1. SC. Choose the correct answer. A healthy ear hears a shouting voice at a distance of : a. 100 m b. 300 m c. 50 m d. 200 m e. 500 m 2. SC. Choose the correct answer. Negative Rinne's test , lateralized Weber's test in an affected or healthy ear , prolonged or shortened Schwabach's test are known as the triad of : a. Rozen b. Gelle c. Bedzold d. Bing e. Schuller 3. SC. Choose the correct answer. Otoscopic sign of Schwartz is frequently observed in : a. Tympanosclerosis b. Otosclerosis c. Perceptive deafness d. Adhesive otitis media e. Meniere's disease 4. SC. Choose the correct answer. Which of the following tests presents the comparison of the air and bone conduction: a. Rinne’s test b. Schwabach’s test c. Weber’s test d. Gelle’s test e. Vomer’s test 5. SC. Choose the correct answer. In case of acute otitis media Rinne's test is: a. Positive b. Negative c. Prolonged d. Lateralized in the healthy ear e. Lateralized in the affected ear 6. SC. Choose the correct answer. What does Schwabach's test examine : a. Duration of air conductivity b. Duration of bone conduction c. Stapes mobility d. Tympanum mobility e. Malleus mobility 7. SC. Choose the correct answer. Gelle's test allows to reveal : a. Cholesteatoma b. Labyrinth fistula c. Tubal obstruction d. Otosclerosis e. Adhesive otitis 8. SC. Choose the correct answer. Which of the following diagnostic methods is the most informative in detecting (of) acoustic neuroma : a. -

Septal Deviation Operation Informed Consent Form
SEPTAL DEVIATION OPERATION INFORMED CONSENT FORM FIRST DOCUMEN RB.FR. PUBLIS REVISION REVISION PAGE 01.02.2010 09.12.2015 1 1/6 T NO 15 HING DATE NO NO DATE Revision Cause: PATIENT’S Name Surname:……………………………………………... Birthdate :…………………………………………. Hospital Admission Date:………………………………. Hospitalization Date:…………………………………… Protocol Number:…………………………………….. Telephone Number:……………………………………… Address:………………………………………………………………………………………………………… …………………………………………………………………………………………………………………… Please read this form carefully and answer the questions. As a result of the examinations, it has been decided that you should undergo surgical intervention because of “septal deviation”. Before the procedure, your doctor will give you information about the course and the different forms of the procedure and the risks involved. Accordingly, you will be free to decide on the interventions. This written form is intended to provide you with basic information about the intervention and associated complications (problems that may occur during or after the procedure). What you should know about your disease: The nasal septum deviation (see figure) occurs due to the development of deformities of the facial bones, as well as fractures of the nasal bone that may occur during birth. If the deviation is causing the following problems, surgery is required: 1. Difficulty in nasal respiration 2. Drying, burning sensation, feeling of foreign body in the throat due to continuous oral breathing 3. Snoring, sleep acnea (occasionally) 4. Head/face ache 5. Recurrent sinusitis, 6. Laryngitis and bronchi inflammation 7. İnfection of the Eustachian tube and tendency to middle ear infections . In some sinus operations and certain types of nasal bleeding, nasal septum deviation surgery may be necessary. SEPTAL DEVIATION OPERATION INFORMED CONSENT FORM FIRST DOCUMEN RB.FR. -

Extranodal Nk/T-Cell Lymphoma, Nasal Type: Case Report
case reports 2021; 7(1) https://doi.org/10.15446/cr.v7n1.85915 EXTRANODAL NK/T-CELL LYMPHOMA, NASAL TYPE: CASE REPORT Keywords: Lymphoma; Cellulitis; Sinusitis; Herpesvirus 4, Human; T lymphocytes. Palabras clave: Linfoma; Celulitis; Sinusitis; Herpesvirus Humano 4; Linfocitos T. María Fernanda Ochoa-Ariza Marly Esperanza Camargo-Lozada Universidad Autónoma de Bucaramanga Universidad Nacional de Colombia - - Faculty of Health Sciences - Medical Program Bogotá Campus - Faculty of Medicine - - Bucaramanga - Colombia. Bogotá, D.C. - Colombia. Clínica La Riviera - Outpatient Surgery Service Clínica Chicamocha - Inpatient Service - - Bucaramanga - Colombia. Bucaramanga - Colombia. Silvia Juliana García-Guevara Viviana Catalina Jiménez-Andrade Universidad Autónoma de Bucaramanga Universidad Industrial de Santander - - Faculty of Health Sciences - Medical Program Faculty of Health Sciences - Medical Program - - Bucaramanga - Colombia. Bucaramanga - Colombia. Marlon Adrián Laguado-Nieto Universidad Autónoma de Bucaramanga - Faculty of Health Sciences - Medical Program - Bucaramanga - Colombia. Clínica FOSCAL - Intensive Care Unit Service - Colombia. Corresponding author Viviana Catalina Jiménez-Andrade. Facultad de Ciencias de la Salud, Universidad Industrial de Santander. Bucaramanga. Colombia. Email: [email protected]. Received: 27/03/2020 Accepted: 28/05/2020 case reports Vol. 7 No. 1: 7-14 8 RESUMEN ABSTRACT Introducción. El linfoma extranodal nasal de Introduction: Extranodal NK/T-cell lympho- células T/natural killer (ENKL) es un linfoma ma, nasal type (ENKL), is a highly aggressive no Hodgkin altamente agresivo y de etiología non-Hodgkin’s lymphoma of unknown etiology. desconocida. Sus manifestaciones clínicas suel- Clinical manifestations are usually nasal obstruc- en ser obstrucción nasal, epistaxis y signos in- tion, epistaxis, and inflammatory signs. Diagnosis flamatorios; sin embargo, el diagnóstico puede can be difficult to achieve and requires histo- llegar a ser difícil, requiriendo histopatología e pathology and immunohistochemistry studies. -

(SASJS) Nasal Septal Perforation Management:A Challenging Task
SAS Journal of Surgery (SASJS) ISSN 2454-5104 Abbreviated Key Title: SAS J. Surg. ©Scholars Academic and Scientific Publishers (SAS Publishers) A Unit of Scholars Academic and Scientific Society, India Nasal Septal Perforation Management:A Challenging Task Selçuk Kuzu1, Fatih Çapanoğlu1 1Emirdağ State Hospital Otorhinolaryngology Clinic, Afyonkarahisar, Türkiye Abstract: Nasal septum perforation is an anatomic defect that develops as a Short Communication consequence of necrosis of mucosa, bone and cartilage structures of septum. Although relatively rare, septal perforations are difficult problems that the otolaryngologist has to *Corresponding author solve. There are many etiological causes of nasal septum perforation. As it may be Selçuk Kuzu idiopathic, the most common cause is iatrogenic as nasal surgeries. The majority of nasal septal perforations are asymptomatic. Septum perforations can cause complaints Article History such as whistling in the respiratory tract, drying, epistaxis, cacosmia and nasal Received: 15.12.2017 discharge. Nasal saline lavages and shell softening creams are conservative treatment Accepted: 20.12.2017 methods to prevent scaling and bleeding after septal perforation. Besides septal silicone Published: 30.12.2017 button application, the main treatment is surgical repair of perforation. In this review, etiology of nasal septal perforation, clinic and treatment options are discussed in the DOI: light of current literature. 10.21276/sasjs.2017.3.12.2 Keywords: Nasal septum, perforation, respiratory tract, drying INTRODUCTION The midline cartilage (septum) that divides the nasal cavity in two and the mucosa that covers it may be pierced in some cases as a full layer. This condition is called nasal septal perforation. Nasal septum perforation is an anatomic defect that develops as a consequence of necrosis of mucosa, bone and cartilage structures of septum. -
ERS Statement on Obstructive Sleep Disordered Breathing in 1- to 23-Month-Old Children
ERS OFFICIAL DOCUMENT ERS STATEMENT ERS statement on obstructive sleep disordered breathing in 1- to 23-month-old children Athanasios G. Kaditis1, Maria Luz Alonso Alvarez2, An Boudewyns3, Francois Abel4, Emmanouel I. Alexopoulos5, Refika Ersu6, Koen Joosten7, Helena Larramona8, Silvia Miano9, Indra Narang10, Hui-Leng Tan11, Ha Trang12, Marina Tsaoussoglou1, Nele Vandenbussche13, Maria Pia Villa14, Dick Van Waardenburg15, Silke Weber16 and Stijn Verhulst17 @ERSpublications Obstructive sleep disordered breathing in young children is a heterogeneous group of disorders http://ow.ly/qqgc30fGvaj Cite this article as: Kaditis AG, Alonso Alvarez ML, Boudewyns A, et al. ERS statement on obstructive sleep disordered breathing in 1- to 23-month-old children. Eur Respir J 2017; 50: 1700985 [https://doi.org/ 10.1183/13993003.00985-2017]. ABSTRACT The present statement was produced by a European Respiratory Society Task Force to summarise the evidence and current practice on the diagnosis and management of obstructive sleep disordered breathing (SDB) in children aged 1–23 months. A systematic literature search was completed and 159 articles were summarised to answer clinically relevant questions. SDB is suspected when symptoms or abnormalities related to upper airway obstruction are identified. Morbidity (pulmonary hypertension, growth delay, behavioural problems) and coexisting conditions (feeding difficulties, recurrent otitis media) may be present. SDB severity is measured objectively, preferably by polysomnography, or alternatively polygraphy or nocturnal oximetry. Children with apparent upper airway obstruction during wakefulness, those with abnormal sleep study in combination with SDB symptoms (e.g. snoring) and/or conditions predisposing to SDB (e.g. mandibular hypoplasia) as well as children with SDB and complex conditions (e.g. -

What Are the Factors Leading to Nasal Septal Perforations After Septoplasty?
ISSN: 2572-4193 YILDIZ et al. J Otolaryngol Rhinol 2019, 5:065 DOI: 10.23937/2572-4193.1510065 Volume 5 | Issue 3 Journal of Open Access Otolaryngology and Rhinology REsEARCH ARtıCLE What are the Factors Leading to Nasal Septal Perforations after Septoplasty? Erkan YILDIZ1*, Şahin ULU2 and Orhan Kemal KAHVECİ2 Check for 1Department of Otorhinolaringology, Afyonkarahisar Şuhut State Hospital, Afyonkarahisar, Turkey updates 2Department of Otorhinolaringology, Healty Science University Hospital, Afyonkarahisar, Turkey *Corresponding author: Dr. Erkan YILDIZ, Department of Otorhinolaringology, Afyonkarahisar Şuhut State Hospital, 03800 Şuhut/Afyonkarahisar, Turkey, Tel: 05308950416, ORCID: 0000-0002-0265-7327 Abstract Introduction Objective: Nasal septal perforation is the most common Nasal septal perforation; the nasal septum consists complication in the long term after septoplasty. Nasal septal of the cartilage, the bone septum and the mucosal layer perforation is the partial opening of the wall between both nasal cavities. In this study, we will evaluate the causes of covering it. The bone septum consists of the vomer, septal perforation after septoplasty. the lamina perpendicular of the ethmoid bone and the Materials and methods: 400 patients aged between maxillary crest. As a result of necrosis of the septum 18 and 50 years who underwent septoplasty operation due to damage to these layers, there is a gap between in Afyonkarahisar Şuhut State Hospital between 2016- the two nasal cavities. Therefore, the nasal airflow is 2019 were evaluated retrospectively. These patients were disturbed and leads to deterioration in the quality of divided into groups with and without perforation. Smoking life of the patient [1]. and alcohol use of patients with perforation, gender and septum stabilization was used for the technique. -

Endoscopic Sandwich Technique for Moderate Nasal Septal Perforations
The Laryngoscope VC 2012 The American Laryngological, Rhinological and Otological Society, Inc. Endoscopic Sandwich Technique for Moderate Nasal Septal Perforations Feng-Hong Chen, MD; Xu Rui, MD, PhD; Jie Deng, MD; Yi-Hui Wen, MD; Geng Xu, MD, PhD; Jian-Bo Shi, MD, PhD Objectives/Hypothesis: The aim of this article was to describe our surgical technique for the treatment of nasal septal perforations with diameters of 1 to 2 cm. Study Design: Retrospective clinical research. Methods: We reviewed 13 patients with moderate nasal septal perforations (1–2 cm diameter) treated with a sandwich technique (bone or cartilage and quadriceps fascia graft as an interposition graft) by an endoscope-assisted intranasal approach from January 2008 to June 2011. Follow-up periods were 3 months. Results: Thirteen patients were treated with the sandwich technique. Twelve cases (92.3%) were completely healed. One case received incomplete closures without any postoperative symptoms. All patients were found not to have any compli- cations after surgery. Conclusions: The transnasal endoscopic sandwich technique for repairing moderate nasal septal perforation (1–2 cm) has a high success rate and is easy to perform. Key Words: Endoscopes, reconstructive surgical procedure, nasal septum, perforation. Level of Evidence: 4. Laryngoscope, 122:2367–2372, 2012 INTRODUCTION The purpose of this article is to report our surgical Nasal septal perforation implies a complete defect technique repairing nasal septal perforations between 1 of cartilage or bone and mucosa in bilateral nasal sep- and 2 cm in diameter via nasal endoscopy. tum. It may cause the symptoms of crusting, nasal bleeding and obstruction, dryness, discharge, and so on. -

Combination Treatment Bolsters COPD Control
July 1, 2008 • www.familypracticenews.com Pulmonary Medicine 37 Combination Treatment Bolsters COPD Control BY NANCY WALSH bination of the long-acting anticholiner- to forced vital capacity was less than 70%. an international conference of the Amer- New York Bureau gic tiotropium plus the long-acting β2-ag- Spirometric measurements were per- ican Thoracic Society. onist formoterol to improve symptom formed weekly, and the number of puffs of Daytime albuterol puffs were reduced T ORONTO — Patients with chronic ob- control and lessen the need for rescue al- rescue medication was recorded in patient by 1.16/day in the combination group, structive pulmonary disease treated with buterol to a greater degree than the anti- diaries. The majority of patients were white which also was significantly greater than a combination of formoterol and tiotropi- cholinergic alone. men, and the average age was 64 years. the reduction of 0.76 in the monothera- um required less rescue medication than The 255 participating patients were aged Overall daily rescue medication use was py group. did those treated with tiotropium alone. 40 years or older and had at least a 10 pack- reduced by 0.81 puffs/day in the combi- Overall nighttime albuterol use was re- In a 12-week double-blind trial spon- year history of smoking. Postbron- nation group, which was significantly duced by 0.44 puffs/day and 0.28 puffs/day sored by Schering-Plough, Dr. Donald P. chodilator forced expiratory volume in 1 greater than the reduction in the in the combination and monotherapy Tashkin of the University of California, second (FEV1) was 30%-70% of predicted monotherapy group of 0.53 puffs/day, groups, respectively.