2011 NHGRI Strategic Plan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Use of Cell Culture in Virology for Developing Countries in the South-East Asia Region © World Health Organization 2017
USE OF CELL C USE OF CELL U LT U RE IN VIROLOGY FOR DE RE IN VIROLOGY V ELOPING C O U NTRIES IN THE NTRIES IN S O U TH- E AST USE OF CELL CULTURE A SIA IN VIROLOGY FOR R EGION ISBN: 978-92-9022-600-0 DEVELOPING COUNTRIES IN THE SOUTH-EAST ASIA REGION World Health House Indraprastha Estate, Mahatma Gandhi Marg, New Delhi-110002, India Website: www.searo.who.int USE OF CELL CULTURE IN VIROLOGY FOR DEVELOPING COUNTRIES IN THE SOUTH-EAST ASIA REGION © World Health Organization 2017 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial- ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition.” Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. -
Peptide-Based Scaffolds for the Culture and Maintenance of Primary
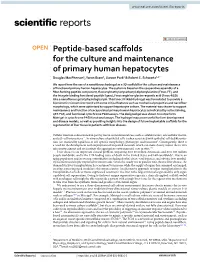
www.nature.com/scientificreports OPEN Peptide‑based scafolds for the culture and maintenance of primary human hepatocytes Douglas MacPherson1, Yaron Bram1, Jiwoon Park1 & Robert E. Schwartz1,2* We report here the use of a nanofbrous hydrogel as a 3D scafold for the culture and maintenance of functional primary human hepatocytes. The system is based on the cooperative assembly of a fber‑forming peptide component, fuorenylmethyloxycarbonyl‑diphenylalanine (Fmoc‑FF), and the integrin‑binding functional peptide ligand, Fmoc‑arginine‑glycine‑aspartic acid (Fmoc‑RGD) into a nanofbrous gel at physiological pH. This Fmoc‑FF/RGD hydrogel was formulated to provide a biomimetic microenvironment with some critical features such as mechanical properties and nanofber morphology, which were optimized to support hepatocyte culture. The material was shown to support maintenance and function of encapsulated primary human hepatocytes as indicated by actin staining, qRT‑PCR, and functional cytochrome P450 assays. The designed gel was shown to outperform Matrigel in cytochrome P450 functional assays. The hydrogel may prove useful for liver development and disease models, as well as providing insights into the design of future implantable scafolds for the regeneration of liver tissue in patients with liver disease. Cellular function is determined in part by micro-environmental cues such as soluble factors, extracellular matrix, and cell–cell interactions 1,2. In vitro culture of epithelial cells is ofen associated with epithelial cell dediferentia- tion (i.e. marked by rapid loss of cell-specifc morphology, phenotype, and function)3. Consequently, there is a need for the development and employment of improved materials which can more closely mimic the in vivo microenvironment and reconstitute the appropriate environmental cues in vitro1–3. -

Nano-Silver Particles Reduce Contaminations in Tissue Culture but Decrease Regeneration Rate and Slows Down Growth and Development of Aldrovanda Vesiculosa Explants
applied sciences Article Nano-Silver Particles Reduce Contaminations in Tissue Culture but Decrease Regeneration Rate and Slows Down Growth and Development of Aldrovanda vesiculosa Explants Marzena Parzymies Subdepartment of Ornamental Plants and Dendrology, Institute of Horticultural Production, Faculty of Horticulture and Landscape Architecture, University of Life Sciences in Lublin, Ul. Gł˛eboka28, 20-612 Lublin, Poland; [email protected] Abstract: Aldrovanda vesiculosa is a carnivorous water plant which is endangered by extinction worldwide. The number of natural stands and populations has decreased; therefore, there is a need for its active protection. The best method would be an in vitro culture. One of the main problems is disinfection of the explants. Therefore, it was decided that we should treat the explants with nano- silver particles. The explants were shoot fragments which were disinfected with sodium hypochlorite and then placed in a liquid 1/5 MS medium, supplemented with silver nanoparticles (AgNPs) at a concentration of 5 mg·dm−3. It was observed that AgNPs reduced the number of contaminations but also led to necrosis of the shoots. The shoots, which undertook regeneration in presence of AgNPs, were smaller and did not form traps; however, after being moved to fresh media twice, they started to develop normal leaves. Taking into consideration both disinfection and regeneration rates, it might be advisable to disinfect aldrovanda shoots in sodium hypochlorite only, without AgNPs. The results Citation: Parzymies, M. Nano-Silver of the research might indicate a toxic activity of AgNPs towards water plants, which seems a big Particles Reduce Contaminations in problem, as nanoparticles are commonly used in all the fields of life. -

Chapter 11: Virology
CHAPTER 11 Virology Ken Peters USFWS – Bozeman Fish Health Center Bozeman, Montana NWFHS Laboratory Procedures Manual - Second Edition, June 2004 Chapter 11 - Page 1 I. Introduction Detection of aquatic animal viruses historically has been by growth and isolation on living cell cultures appropriately researched and chosen for the propagation of target viruses and species of host. Viral detection can also include immunological and nucleotide testing procedures. The determination of a testing procedure is a complex decision involving factors of cost, timeliness, sensitivity, specificity, efficiency, and available host tissues and technology. For the purposes of the Wild Fish Health Survey, the USFWS has chosen the use of cell culture for initial screening and corroboration of test results using appropriate nucleotide primers of specific viral pathogens in polymerase chain reaction (PCR) tests. Other corroborative tests may also be utilized, including serum neutralization, indirect fluorescent antibody techniques, biotinylated DNA probes, and immuno-dot blot tests (see Chapter 12 - Corroborative Testing of Viral Isolates). The following sections describe the procedures and methods for virology using standard cell culture techniques. Definitions: Several terms are used routinely in virology and throughout this section. A full Glossary of terms can be found in Appendix A. Media Formulations: See Appendix B: Media Used in Tissue Culture and Virology. II. Selection of Appropriate Cell Lines All viral testing will utilize cell lines traceable to cell lines from the American Type Culture Collection (ATCC) when available. At the minimum, cell lines will be tested annually for viral sensitivity and mycoplasma infection: see section VI. Quality Control in Tissue Culture, in Chapter 10 -Tissue Culture of Fish Cell Lines. -

Introduction to Mammalian Cell Culture
Workshop Training Series Biomedical and Obesity Research Core Nebraska Center for the Prevention of Obesity Diseases through Dietary Molecules Introduction to Mammalian Cell Culture April 9, 2019 Yongjun Wang Ph.D. Director of Biomedical and Obesity Research Core Nebraska Center for the Prevention of Obesity Diseases through Dietary Molecules What Is Cell Culture Cell culture is the process by which cells are grown in controlled conditions outside of their native environment. Timeline: key milestone in cell cultures History of Cell Culture http://dx.doi.org/10.5772/66905 Primary vs Cell line Primary cells Cell lines Lifespan and division capacity Limited Indefinite Isolated in the lab or bought from Source Bought from commercial provider commercial provider Care and maintenance Complex and difficult Easy to maintain or proliferate Chromosomal aberration Minimal Several Retention of functional markers and Yes Not always signaling pathways Functional study, diagnosis, Drug development, vaccine and protein Application Gene therapy, et al. production, et al. Three Types of Cells Epithelial-like cells Fibroblast-like cells Lymphoblast-like cells Cell differentiation 3T3L1 cells C212 cells Cell Culture Vessels • Most adherent cells require attachment to proliferate • Polystyrene are treated to become hydrophilic and negatively charged once medium is added • Coating with basic synthetic polymers • Poly-L-lysine • Coating with matrix proteins • Collagen, laminin, gelatin, fibronectin Class II Biological Safety Cabinet The Class II Biological Safety -

Basic Pluripotent Stem Cell Culture Protocols Maria Borowski∗, Maria Giovino-Doherty, Lan Ji, Meng-Jiao Shi, Kelly P
Basic pluripotent stem cell culture protocols Maria Borowski∗, Maria Giovino-Doherty, Lan Ji, Meng-Jiao Shi, Kelly P. Smith and Joseph Laning, Massachusetts Stem Cell Bank, University of Massachusetts Medical School, Shrewsbury, MA 01545 USA Abstract Stem cell research is a rapidly expanding field with the potential to develop therapeutic agents to treat diseases as well as study disease development from early stages. The culture of human pluripotent stem cells shares many of the same protocols as standard mammalian cell culture. However, the successful culture and maintenance of human pluripotent stem cells (hPSCs) in an undifferentiated state requires additional consider- ations to ensure that cells maintain their key characteristics of self-renewal and pluripotency. There are several basic techniques needed for the culturing of mammalian cells, including thawing frozen stocks, plating cells in culture vessels, changing media, passaging and cryopreservation. The protocols in this document represent a subset of the standard operating procedures used to maintain and culture stem cells at the Massachusetts Human Stem Cell Bank, and have been thoroughly testing and verified. A Stem cell culture considerations Stem cell research is a rapidly expanding field with the potential to develop therapeutic agents to treat diseases as well as study disease development from early stages. However, to fulfill this promise, researchers need to have access to standardized protocols for the development, maintenance and differentiation of these unique cells. Such “best practices” will allow comparisons of different studies and hasten the refinement of these techniques. Such standardization can be driven by resources such as StemBook and by stem cell banks. -
From 2D Culture to Organ-On-Chip Lab on a Chip
Volume 18 Number 9 07 May 2018 Pages 1267–1390 Lab on a Chip Devices and applications at the micro- and nanoscale rsc.li/loc ISSN 1473-0197 CRITICAL REVIEW Jochen Kieninger et al. Microsensor systems for cell metabolism – from 2D culture to organ-on-chip Lab on a Chip View Article Online CRITICAL REVIEW View Journal | View Issue Microsensor systems for cell metabolism – from Cite this: Lab Chip,2018,18,1274 2D culture to organ-on-chip Jochen Kieninger, * Andreas Weltin, Hubert Flamm and Gerald A. Urban Microsensor systems for cell metabolism are essential tools for investigation and standardization in cell cul- ture. Electrochemical and optical read-out schemes dominate, which enable the marker-free, continuous, online recording of transient effects and deliver information beyond microscopy and end-point tests. There has been much progress in microfluidics and microsensors, but the translation of both into standard cell culture procedures is still limited. Within this critical review, we discuss different cell culture formats ranging from standard culture vessels to dedicated microfluidic platforms. Key aspects are the appropriate supply of cells, mass transport of metabolites to the sensors and generation of stimuli. Microfluidics enable the transition from static to dynamic conditions in culture and measurement. We illustrate the parameters oxy- gen (respiration), pH (acidification), glucose and lactate (energy metabolism) as well as short-lived reactive Creative Commons Attribution 3.0 Unported Licence. species (ROS/RNS) from the perspective of microsensor integration in 2D and 3D cell culture. We discuss different sensor principles and types, along with their limitations, microfabrication technologies and mate- Received 1st September 2017, rials. -

Mass Propagation of Plant Cells – an Emerging Technology Platform for Sustainable Production of Biopharmaceuticals
mac har olo P gy : Georgiev, Biochem Pharmacol (Los Angel) 2015, 4:5 & O y r p t e s i n DOI: 10.4172/2167-0501.1000e180 A m c e c h e c s Open Access o i s Biochemistry & Pharmacology: B ISSN: 2167-0501 Editorial Open Access Mass Propagation of Plant Cells – An Emerging Technology Platform for Sustainable Production of Biopharmaceuticals Vasil Georgiev* Center for Viticulture and Small Fruit Research, College of Agriculture and Food Sciences, Florida A & M University, 6505 Mahan Drive, Tallahassee, FL 32317, USA Editorial continuous supply of high quality biomass from exotic, rare, protected, or endangered plants, or plants growing in remote, barely accessible Plants have been used as a source of natural compounds with areas [15]. Recently, several PMIs obtained by PCCT have been released, unique chemical structures and wide range of biological activities since including anti-ageing, calming, and protecting cosmetic supplement time immemorial, and to this day, 11% of the essential drugs for human “ResistemTM” Sederma (www.sederma.fr); UV-protective additive application originate in plants [1]. The expanded demand for medicinal PhytoCellTec™ Solar Vitis, anti-aging and delaying the senescence of plants raise issues of concern about sustainability, conservation and hair follicles supplement PhytoCellTec™ Malus Domestica, and anti- the preservation of natural habitats. Overharvesting of some species aging and UV-protective supplement PhytoCellTec™ nunatak® from for commercial uses reduced the stocks of wild populations and has cell culture of rare and protected plant species Saponaria pumila placed some species under threat [2]. Moreover, most of the medicinal (recognized as an Eco breakthrough at the UN Conference Rio+20) by plants are rare or endemic species, growing under specific climate, Mibelle Biochemistry (www.mibellebiochemistry.com). -

LABORATORY TECHNIQUES in VIROLOGY by Marie P
LABORATORY TECHNIQUES IN VIROLOGY by Marie P. Fried Number 29 LABORATORY TECHNIQUES IN VIROLOGY by Marie P. Fried Number 29 Alaska Department of Fish and Game Division of Fisheries Rehabilitation, Enhancement and Development Don W. Collinsworth Commissioner Stanley A. Moberly Director P.O. Box 3-2000 Juneau, Alaska 99802 April 1984 TABLE OF CONTENTS PAGE Glossary' ........................................................... 1 Maintenance of stock cell lines: passage of confluent cell monolayer ................................................4 Incubating cell lines ..............................................6 Cytopathic effect of virus infection on tissue culture cells .........................................................7 Assays used in virology ............................................ 9 Collecting ovarian fluid, whole fish, and tissue samples for traditional assay ........................................ 10 Processing ovarian fluid, whole fish, and tissue samples for traditional assay ........................................ 13 Traditional assay .................................................15 Processing ovarian fluid, whole fish, and tissue samples for plaque assay .............................................19 Plaque assay ......................................................20 Serum neutralization assay ........................................25 Media .............................................................28 Detecting and avoiding bacterial and fungal contaminants ..........33 Washing glassware .................................................34 -

Bioreactors and Cultivation Systems for Cell and Tissue Culture
BIOTECHNOLOGY – Bioreactoes and Cultivation Systems for Cell and Tissue Culture - M.K. Popovic , Ralf Portner BIOREACTORS AND CULTIVATION SYSTEMS FOR CELL AND TISSUE CULTURE M.K. Popović Beuth Hochschule für Technik,University of Applied Sciences, Berlin, Germany Ralf Pörtner Hamburg University of Technology, Institute of Bioprocess and Biosystems Engineering, Germany Keywords: Mammalian cells, insect cells, plant cells, tissue engineering, stem cells, bioreactors Contents 1. Introduction 2. Mammalian cells 2.1. Products from mammalian cells 2.2. Properties and medium requirements of mammalian cells 2.3. Bioreactors for mammalian cells 2.3.1. Categorization 2.3.2. Immobilization of cells 2.3.3. Process strategies 2.4. Bioreactor design and scale-up 2.4.1. Bioreactors for cell suspension 2.4.2. Fixed bed and fluidized bed reactors 2.4.3. Hollow fiber and membrane reactors 2.4.4. Single-use bioreactors 3. Insect cell culture 4. Plant cell culture 5. Tissue engineering and stem cell culture 5.1 Bioreactor concepts for tissue engineering 5.2 Propagation of stem cells 6. Regulatory and safety issues 7. Conclusions 8. ReferencesUNESCO – EOLSS Summary SAMPLE CHAPTERS Cell and tissue culture is the complex process by which cells, mostly of mammalian or plant origin, are grown under controlled conditions. The importance of cell and tissue culture in large scale is reflected in the many valuable products for human health. Products from mammalian cells such as monoclonal antibodies, cytokines, recombinant glycoproteins, and, increasingly, vaccines dominate the biopharmaceutical industry. Regenerative medicine using human primary and stem cells opens new therapeutic concepts. Additionally, plant cell and tissue cultures for the production of biologically active substances (low molecular secondary metabolites and recombinant proteins) are of growing importance. -

Leisa 17¥4.2
major modern biotechnologies amongst a larger public is indispensable. The aim of this article is to describe four major modern biotechnologies, their applications and the inputs they require, i.e. in vitro technologies, detection technologies, genomics and genetic modification. Although the last application is discussed in more detail, care should be taken not to equate biotechnology to genetic modification of living organisms. In-vitro technologies The meaning of the Latin words ‘in vitro’ is ‘in glass’. In-vitro technologies separate parts of living organisms in closed containers to manipulate and maintain this material. Several well- known and relatively older applications belong to this category. Plant tissue culture became established in the 1970s. It involves the maintenance of plant material (complete plants, specific organs or cells) under sterile conditions and in the presence of nutrients. Plant tissue culture allows the rapid multiplication of crop plants at a small scale in comparison to ‘in vivo’ (living) conditions. Starter material for crops can thus be supplied in large quantities, solving bottle-necks in supply to farmers. Particularly for crops that are propagated vegetatively (not through seed), plant tissue culture forms a useful instrument to multiply starter material. Plant tissue culture also allows for the cleaning of virus- infected starter material. A third use of plant tissue culture is to Small farmers need a basket of options to meet their site-specific conserve useful crop genetic resources in a less vulnerable requirements Photo: Bert Lof environment than in the field. Finally, plant tissue culture, done in-vitro, can be used to transfer useful traits from wild relatives into crop varieties by crossing sexual barriers that do not take place under normal (in vivo) conditions. -

A Practical Guide to Hydrogels for Cell Culture Steven R Caliari & Jason a Burdick
REVIEW A practical guide to hydrogels for cell culture Steven R Caliari & Jason A Burdick There is growing appreciation of the role that the extracellular environment plays in regulating cell behavior. Mechanical, structural, and compositional cues, either alone or in concert, can drastically alter cell function. Biomaterials, and particularly hydrogels, have been developed and implemented to present defined subsets of these cues for investigating countless cellular processes as a means of understanding morphogenesis, aging, and disease. Although most scientists concede that standard cell culture materials (tissue culture plastic and glass) do a poor job of recapitulating native cellular milieus, there is currently a knowledge barrier for many researchers in regard to the application of hydrogels for cell culture. Here, we introduce hydrogels to those who may be unfamiliar with procedures to culture and study cells with these systems, with a particular focus on commercially available hydrogels. Introduction: why hydrogels for cell culture? (Fig. 2) since they mimic salient elements of native Our collective understanding of many cell-based pro- extracellular matrices (ECMs), have mechanics similar Nature America, Inc. All rights reserved. America, Inc. Nature cesses is derived from experiments performed on flat, to those of many soft tissues, and can support cell adhe- 6 unphysiologically stiff materials such as polystyrene sion and protein sequestration3. © 201 and glass. Although the simplicity of these platforms Hydrogels have proven useful in a range of cell cul- is attractive, cells cultured in these environments tend ture applications, revealing fundamental phenom- to display aberrant behaviors: flattened shape, abnor- ena regulating cell behavior and providing tools for mal polarization, altered response to pharmaceutical the expansion and directed differentiation of various npg reagents, and loss of differentiated phenotype (Fig.