Cameroon Developing Subnational Estimates of Hiv Prevalence and the Number of People
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Page 1 C H a D N I G E R N I G E R I a G a B O N CENTRAL AFRICAN
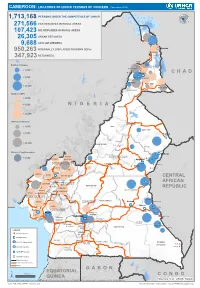
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (November 2019) 1,713,168 PERSONS UNDER THE COMPETENCENIGER OF UNHCR 271,566 CAR REFUGEES IN RURAL AREAS 107,423 NIG REFUGEES IN RURAL AREAS 26,305 URBAN REFUGEES 9,688 ASYLUM SEEKERS 950,263 INTERNALLY DISPLACED PERSONS (IDPs) Kousseri LOGONE 347,923 RETURNEES ET CHARI Waza Limani Magdeme Number of refugees EXTRÊME-NORD MAYO SAVA < 3,000 Mora Mokolo Maroua CHAD > 5,000 Minawao DIAMARÉ MAYO TSANAGA MAYO KANI > 20,000 MAYO DANAY MAYO LOUTI Number of IDPs < 2,000 > 5,000 NIGERIA BÉNOUÉ > 20,000 Number of returnees NORD < 2,000 FARO MAYO REY > 5,000 Touboro > 20,000 FARO ET DÉO Beke chantier Ndip Beka VINA Number of asylum seekers Djohong DONGA < 5,000 ADAMAOUA Borgop MENCHUM MANTUNG Meiganga Ngam NORD-OUEST MAYO BANYO DJEREM Alhamdou MBÉRÉ BOYO Gbatoua BUI Kounde MEZAM MANYU MOMO NGO KETUNJIA CENTRAL Bamenda NOUN BAMBOUTOS AFRICAN LEBIALEM OUEST Gado Badzere MIFI MBAM ET KIM MENOUA KOUNG KHI REPUBLIC LOM ET DJEREM KOUPÉ HAUTS PLATEAUX NDIAN MANENGOUBA HAUT NKAM SUD-OUEST NDÉ Timangolo MOUNGO MBAM ET HAUTE SANAGA MEME Bertoua Mbombe Pana INOUBOU CENTRE Batouri NKAM Sandji Mbile Buéa LITTORAL KADEY Douala LEKIÉ MEFOU ET Lolo FAKO AFAMBA YAOUNDE Mbombate Yola SANAGA WOURI NYONG ET MARITIME MFOUMOU MFOUNDI NYONG EST Ngarissingo ET KÉLLÉ MEFOU ET HAUT NYONG AKONO Mboy LEGEND Refugee location NYONG ET SO’O Refugee Camp OCÉAN MVILA UNHCR Representation DJA ET LOBO BOUMBA Bela SUD ET NGOKO Libongo UNHCR Sub-Office VALLÉE DU NTEM UNHCR Field Office UNHCR Field Unit Region boundary Departement boundary Roads GABON EQUATORIAL 100 Km CONGO ± GUINEA The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Sources: Esri, USGS, NOAA Source: IOM, OCHA, UNHCR – Novembre 2019 Pour plus d’information, veuillez contacter Jean Luc KRAMO ([email protected]). -

Characterisation of Fungi of Stored Common Bean Cultivars Grown in Menoua Division, Cameroon
bioRxiv preprint doi: https://doi.org/10.1101/2020.10.31.363184; this version posted November 1, 2020. The copyright holder has placed this preprint (which was not certified by peer review) in the Public Domain. It is no longer restricted by copyright. Anyone can legally share, reuse, remix, or adapt this material for any purpose without crediting the original authors. CHARACTERISATION OF FUNGI OF STORED COMMON BEAN CULTIVARS GROWN IN MENOUA DIVISION, CAMEROON TEH EXODUS AKWA*1, JOHN M MAINGI1, JONAH K. BIRGEN2 *Corresponding author: TEH EXODUS AKWA 1Department of Biochemistry, Microbiology and Biotechnology, Kenyatta University, Nairobi, Kenya 2Department of Plant Sciences, Kenyatta University, Nairobi, Kenya *Corresponding author: [email protected]; Tel.: +254 792 775729; Medical Microbiology, Department of Biochemistry, Microbiology and Biotechnology, Kenyatta University, Nairobi, Kenya, P.O BOX 43844-00100-NAIROBI 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.10.31.363184; this version posted November 1, 2020. The copyright holder has placed this preprint (which was not certified by peer review) in the Public Domain. It is no longer restricted by copyright. Anyone can legally share, reuse, remix, or adapt this material for any purpose without crediting the original authors. CHARACTERISATION OF FUNGI OF STORED COMMON BEAN CULTIVARS GROWN IN MENOUA DIVISION, CAMEROON. Abstract Common bean is a legume grown globally especially in developing countries including Cameroon for human consumption. In Cameroon it is grown in a wide variety of agro ecological zones in quantities enough to last through the off growing season after harvest. Stored common bean after harvest in Cameroon are prone to fungal spoilage which contributes to post harvest losses. -

Back Grou Di Formatio O the Co Servatio Status of Bubi Ga Ad We Ge Tree
BACK GROUD IFORMATIO O THE COSERVATIO STATUS OF BUBIGA AD WEGE TREE SPECIES I AFRICA COUTRIES Report prepared for the International Tropical Timber Organization (ITTO). by Dr Jean Lagarde BETTI, ITTO - CITES Project Africa Regional Coordinator, University of Douala, Cameroon Tel: 00 237 77 30 32 72 [email protected] June 2012 1 TABLE OF COTET TABLE OF CONTENT......................................................................................................... 2 ACKNOWLEDGEMENTS................................................................................................... 4 ABREVIATIONS ................................................................................................................. 5 ABSTRACT.......................................................................................................................... 6 0. INTRODUCTION ........................................................................................................10 I. MATERIAL AND METHOD...........................................................................................11 1.1. Study area..................................................................................................................11 1.2. Method ......................................................................................................................12 II. BIOLOGICAL DATA .....................................................................................................14 2.1. Distribution of Bubinga and Wengé species in Africa.................................................14 -

Aerial Surveys of Wildlife and Human Activity Across the Bouba N'djida
Aerial Surveys of Wildlife and Human Activity Across the Bouba N’djida - Sena Oura - Benoue - Faro Landscape Northern Cameroon and Southwestern Chad April - May 2015 Paul Elkan, Roger Fotso, Chris Hamley, Soqui Mendiguetti, Paul Bour, Vailia Nguertou Alexandre, Iyah Ndjidda Emmanuel, Mbamba Jean Paul, Emmanuel Vounserbo, Etienne Bemadjim, Hensel Fopa Kueteyem and Kenmoe Georges Aime Wildlife Conservation Society Ministry of Forests and Wildlife (MINFOF) L'Ecole de Faune de Garoua Funded by the Great Elephant Census Paul G. Allen Foundation and WCS SUMMARY The Bouba N’djida - Sena Oura - Benoue - Faro Landscape is located in north Cameroon and extends into southwest Chad. It consists of Bouba N’djida, Sena Oura, Benoue and Faro National Parks, in addition to 25 safari hunting zones. Along with Zakouma NP in Chad and Waza NP in the Far North of Cameroon, the landscape represents one of the most important areas for savanna elephant conservation remaining in Central Africa. Aerial wildlife surveys in the landscape were first undertaken in 1977 by Van Lavieren and Esser (1979) focusing only on Bouba N’djida NP. They documented a population of 232 elephants in the park. After a long period with no systematic aerial surveys across the area, Omondi et al (2008) produced a minimum count of 525 elephants for the entire landscape. This included 450 that were counted in Bouba N’djida NP and its adjacent safari hunting zones. The survey also documented a high richness and abundance of other large mammals in the Bouba N’djida NP area, and to the southeast of Faro NP. In the period since 2010, a number of large-scale elephant poaching incidents have taken place in Bouba N’djida NP. -

Cameroon Watershed
Journal(of(Materials(and(( J. Mater. Environ. Sci., 2018, Volume 9, Issue 11, Page 3094-2104 Environmental(Sciences( ISSN(:(2028;2508( CODEN(:(JMESCN( http://www.jmaterenvironsci.com! Copyright(©(2018,( University(of(Mohammed(Premier(((((( (Oujda(Morocco( A typological study of the physicochemical quality of water in the Menoua- Cameroon watershed Santsa Nguefack Charles Vital1*, Ndjouenkeu Robert1, Ngassoum Martin Benoit2 , 1Laboratory of Food Physicochemistry, Department of Food Science and Nutrition National Advanced School of Agro- Industrial Sciences, University of Ngaoundéré, PO BOX 455,Ngaoundéré, Cameroon. 2Department of Industrial Chemistry and Environment, National Advanced School of Agro-Industrial Sciences, University of Ngaoundéré, PO BOX 455, Ngaoundéré, Cameroon. Received 29 Oct 2017 Abstract Revised 25 Dec 2018 Cameroon, a country in Central Africa with an outlet to the Atlantic Ocean in the Gulf Accepted 28 Dec 2018 of Guinea, holds enormous potentialities of water resources. These resources used for the supply of water for human consumption, etc., would be polluted by the Keywords intensification of anthropogenic activities, of which the most important recorded in the !!physicochemical, Menoua watershedof West Cameroon are agriculture and breeding. The objective of this !!pollution, work was to study the spatiotemporal parameters of the physicochemical quality !!Menoua watershed, parameters (temperature, pH, electrical conductivity, Turbidity, Nitrates, Ortho !!Anthropogenic Phosphates, Sulphates, Chloride, Potassium and Calcium) the Menoua activities, watershedthrough a main Principal Component Analysis (ACP). The results obtained showed that the pH, turbidity and orthophosphate have levels which are in contradiction !!Water for human consumption. with WHO standards. The physicochemical parameters of this water showed significant spatial and seasonal variations, the causes of which probably related to the human activities generating pollutants. -

Dictionnaire Des Villages Du Fako : Village Dictionary of Fako Division
OFFICE DE LA RECHERCHE SCIENTIFIOUE ET TECHNIOUE OUTRE· MER Il REPUBLIQUE UNIE DU CAMEROUN DICTIONNAIRE DES VILLAGES DU FAKO VILLAGE DICTIONARY OF FAKO DIVISION SECTION DE GEOGRAPHIE 1 OFFICE DE LA RECHERCHE SCIm~TIFIQUE REPUBLIQUE UNIE ET TECmUQUE OUTRE-lViER DU CAlvŒROUN UNITED REPUBLIC OF CANEROON CENTRE O.R.S.T.O.N DE YAOUNDE DICTIONNAIRE DES VILLAGES DU FAKO VILLAGE DICTIONARY OF FAKO DIVISION Juillet 1973 July 1973 COPYRIGHT O.R.S.T.O.M 1973 TABLE DES NATIERES CONTENTS i l j l ! :i i ~ Présentation •••••.•.•.....••....•.....•....••••••.••.••••••.. 1 j Introduction ........................................•• 3 '! ) Signification des principaux termes utilisés •.............• 5 î l\lIeaning of the main words used Tableau de la population du département •...••.....•..•.•••• 8 Population of Fako division Département du Fako : éléments de démographie •.•.... ..••.•• 9 Fako division: demographic materials Arrondissements de Muyuka et de Tiko : éléments de . démographie 0 ••••••••••••••••••••••••••••••••••••••• 10 11uyul{a and Tileo sl)..bdivisions:demographic materials Arrondissement de Victoria: éléments de démographie •••.••• 11 Victoria subdivision:demographic materials Les plantations (12/1972) •••••••••••.•••••••••••••••••••••• 12 Plantations (12/1972) Liste des villages par arrondissement, commune et graupement 14 List of villages by subdivision, area council and customary court Signification du code chiffré •..•••...•.•...•.......•.•••.• 18 Neaning of the code number Liste alphabétique des villages ••••••.••••••••.•.•..•••.•.• 19 -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -

CMR-3W-Cash-Transfer-Partners V3.4
CAMEROON: 3W Operational Presence - Cash Programming [as of December 2016] Organizations working for cash 10 programs in Cameroon Organizations working in Organizations by Cluster Food security 5 International NGO 5 Multi-Sector cash 5 Government 2 Economic Recovery 3 Red Cross & Red /Livelihood 2 Crescent Movement Nutrition 1 UN Agency 1 WASH 1 Number of organizations Multi-Sector Cash by departments 15 5 distinct organizations 9 organizations conducting only emergency programs 1 organizations conducting only regular programs Number of organizations by departments 15 Economic Recovery/Livelihood Food security 3 distinct organizations 5 distinct organizations Number of organizations Number of organizations by department by department 15 15 Nutrition WASH 3 distinct organizations 1 organization Number of organizations Number of organizations by department by department 15 15 Creation: December 2016 Sources: Cash Working group, UNOCHA and NGOs More information: https://www.humanitarianresponse.info/en/operations/cameroon/cash )HHGEDFNRFKDFDPHURRQ#XQRUJ 7KHERXQGDULHVDQGQDPHVVKRZQDQGWKHGHVLJQDWLRQVXVHGRQWKLVPDSGRQRWLPSO\RI̙FLDOHQGRUVHPHQWRUDFFHSWDQFHE\WKH8QLWHG1DWLRQV CAMEROON:CAMEROON: 3W Operational Presence - Cash Programming [as of December 2016] ADAMAOUA FAR NORTH NORTH 4 distinct organizations 9 distinct organizations 1 organization DJEREM DIAMARE FARO MINJEC CRF MINEPAT CRS IRC MAYO-BANYO LOGONE-ET-CHARI MAYO-LOUTI MINEPAT MINEPAT WFP, PLAN CICR MMBERE MAYO-REY PLAN PUI MINEPAT CENTRE MAYO-DANAY 1 organization MINEPAT LITTORAL 1 organization -
CAMEROON Perspectives on Food Security October 2020 to May 2021 Food Security Improved in the Far North, but Worsened in the Northwest and Southwest
CAMEROON Perspectives on food security October 2020 to May 2021 Food security improved in the Far North, but worsened in the Northwest and Southwest KEY MESSAGES • Despite the recent surge in attacks by Boko Haram, and Current food security situation, October 2020 excessive rainfall leading to flooding in some locations in the Far North, ongoing new harvests have improved food security for many poor households that currently subsist on their own harvests. The harvest of rainfed grains from the primary agricultural campaign in 2020 is estimated to be average, due to favorable weather conditions. Slightly lower than average production is expected in the Logone-et-Chari, Mayo Sava, and Mayo Tsanga departments, where Boko Haram is most active, as well as in locations where harvests were lost to flooding. • Current prices at the primary markets in the Far North appear stable or are decreasing. Since July 2020, staple food prices have increased above typical levels. Sorghum and maize are selling at 46 to 60 percent, and 30 to 47 percent higher (respectively) than in July 2019. Although current prices are still above average, sorghum and groundnut prices have decreased by 17 percent and 18 percent as compared to the Source: FEWS NET previous three months. FEWS NET classification is IPC-compatible (Integrated Phase Classification). IPC-compatible analysis follows key IPC protocols but • In the Northwest and Southwest regions, where agricultural does not necessarily reflect the consensus of national food security production was lower than average for four consecutive years partners. due to ongoing socio-political conflicts, this year's harvests are running out earlier than usual. -
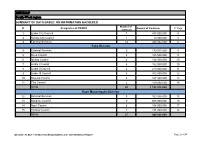
MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Limbe City Council 7 475 000 000 4 2 Kumba City Council 1 10 000 000 5 3 External Services 14 440 032 000 6 Fako Division 4 External Services 9 179 015 000 8 5 Buea Council 5 125 500 000 9 6 Idenau Council 4 124 000 000 10 7 Limbe I Council 4 152 000 000 10 8 Limbe II Council 4 219 000 000 11 9 Limbe III Council 6 102 500 000 12 10 Muyuka Council 6 127 000 000 13 11 Tiko Council 5 159 000 000 14 TOTAL 43 1 188 015 000 Kupe Muanenguba Division 12 External Services 5 100 036 000 15 13 Bangem Council 9 605 000 000 15 14 Nguti Council 6 104 000 000 17 15 Tombel Council 7 131 000 000 18 TOTAL 27 940 036 000 MINMAP / PUBLIC CONTRACTS PROGRAMMING AND MONITORING DIVISION Page 1 of 34 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Lebialem Division 16 External Services 5 134 567 000 19 17 Alou Council 9 144 000 000 19 18 Menji Council 3 181 000 000 20 19 Wabane Council 9 168 611 000 21 TOTAL 26 628 178 000 Manyu Division 18 External Services 5 98 141 000 22 19 Akwaya Council 6 119 500 000 22 20 Eyomojock Council 6 119 000 000 23 21 Mamfe Council 5 232 000 000 24 22 Tinto Council 6 108 000 000 25 TOTAL 28 676 641 000 Meme Division 22 External Services 5 85 600 000 26 23 Mbonge Council 7 149 000 000 26 24 Konye Council 1 27 000 000 27 25 Kumba I Council 3 65 000 000 27 26 Kumba II Council 5 83 000 000 28 27 Kumba III Council 3 84 000 000 28 TOTAL 24 493 600 000 MINMAP / PUBLIC CONTRACTS -
Cahiers Du BUCREP Volume 01, Numéro 01
Cahiers du BUCREP Volume 01, Numéro 01 Analyses préliminaires des données communautaires dans la Province du sud Cameroun en 2003 Tome 1 Analyses Bureau Central des Recensements Juin 2008 et des Etudes de Population - BUCREP 1 Cahiers du BUCREPvolume 01,numéro 01 DIRECTEUR DE PUBLICATION Madame Bernadette MBARGA, Directeur Général CONSEILLE EDITORIAL Monsieur ABDOULAYE OUMAROU DALIL, Directeur Général Adjoint Monsieur Raphaël MFOULOU, Conseiller Technique Principal - UNFPA / 3ème RGPH COORDONNATEUR TECHNIQUE YOUANA Jean PUBLICATION MBARGA MIMBOE EQUIPE DE REDACTION DE CE TOME Joseph-Blaise DJOUMESSI, Gérard MEVA’A, Ambroise HAKOUA, Pascal MEKONTCHOU, André MIENGUE, Mme Marthe ONANA, Martin TSAFACK, P. Kisito BELINGA, Hervé Joël EFON, Jules Valère MINYA, Lucien FOUNGA COLLABORATION DISTRIBUTION Cellule de la Communication et des Relations Publiques Imprimerie Presses du BUCREP 2 Analyses préliminaires des données communautaires dans la province du SUD CAMEROUN en 2003 SOMMAIRE UNE NOUVELLE SOURCE DE DONNEES 5 METHODOLOGIE DES TRAVAUX CARTOGRAPHIQUES 7 1- PRODUCTIONS DU VILLAGE 8 2- INFRASTRUCTURES SCOLAIRES 12 3- INFRASTRUCTURES SANITAIRES 18 4- INFRASTRUCTURES SOCIOCULTURELLES 23 5- CENTRES D’ETAT CIVIL 25 6- AUTRES INFRASTRUCTURES 29 7- INFRASTRUCTURES TOURISTIQUES 31 8- RESEAU DE DISTRIBUTION D’EAU ET D’ELECTRICITE 36 9- VIE ASSOCIATIVE 39 3 4 Analyses préliminaires des données communautaires dans la province du SUD CAMEROUN en 2003 UNE NOUVELLE SOURCE DE DONNNEES : LE QUESTIONNAIRE LOCALITE Les travaux de cartographie censitaire déjà -

Assessing Cost Efficiency Among Small Scale Rice Producers in the West Region of Cameroon: a Stochastic Frontier Model Approach
International Journal of Humanities Social Sciences and Education (IJHSSE) Volume 3, Issue 6, June 2016, PP 1-7 ISSN 2349-0373 (Print) & ISSN 2349-0381 (Online) http://dx.doi.org/10.20431/2349-0381.0306001 www.arcjournals.org Assessing Cost Efficiency among Small Scale Rice Producers in the West Region of Cameroon: A Stochastic Frontier Model Approach Djomo, Raoul Fani*1, Ewung, Bethel1, Egbeadumah, Maryanne Odufa2 1Department of Agricultural Economics. University of Agriculture, Makurdi. Benue-State, Nigeria PMB 2373, Makurdi 2Department of Agricultural Economics and Extension, Federal University Wukari, PMB 1020 Wukari. Taraba State, Nigeria *[email protected] Abstract: Local farmers’ techniques and knowledge in rice cultivation being deficient and the aid system and research to support such farmers’ activities likewise insufficient, technological progress and increase in rice production are not yet assured. Therefore, this Study was undertaken to assess cost efficiency among small scale rice farmers in the West Region of Cameroon using stochastic frontier model approach. A purposive, multistage and stratified random sampling technique was used in selecting the respondents. A total of 192 small scale rice farmers were purposively selected from four (4) out of eight divisions. Data were collected using structured questionnaires and interview schedule, administered on the respondents were analyzed using descriptive statistics and stochastic frontier cost functions. The result indicates that the coefficient of cost of labour was found positive and significantly influence cost of production in small scale rice production at 1 percent level of probability, implying that increases in cost of labour by one unit will also increase cost of production in small scale rice farming by the value of it coefficient.