Inclusion Body Disease in Australian Snakes Jun 2013
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Problems of Python Classification and Hybrid Pythons
PROBLEMS OF PYTHON CLASSIFICATION AND HYBRID PYTHONS. By: Raymond Hoser, 170 Lawson Street, Redfern, NSW, 2016, Australia. Contents: Introduction - Summary of the problems in classifying Australia's pythons - Hybrids between species - Acknowledge ments - References. INTRODUCTION Australasia's pythons attract disproportionate in terest from herpetologists within Australia and elsewhere. There is also considerable debate in relation to the relationships between species, with various arrangements being proposed. Authors including Cogger (1986), Schmida (1985), and Stafford (1986), have tended to follow 'con sensus opinion' when assigning generic names to Australasian pythons. References in relation to general and more specific aspects of Australian pythons can be found in Haser (1981 a , 1981 b, 1981 c and 1982), and elsewhere. This short paper gives a summary of the problems facing Australian python taxonomists and gives details of an unusual captive breeding that resulted in hybrids between species being produced. SUMMARY OF THE PROBLEMS IN CLASSIFYING AUSTRALIA'S PYTHONS With the exception of the Black headed python and Woma (Genus Aspidites), all other Australian py thons have at various times been assigned to a number of different genera. Numerous schemes of 134 classification for the rema1n1ng Australian spe cies of python have been proposed. These include Hoser (1982), McDowell (1975), and Stull (1935). The schemes range from the placing of all species in the genus Python shared with other non Austra lian species, to placing the species in question in up to seven genera. Namely Bot"h:PochiZus3 Chon dropython3 Liasis3 LisaZia3 Liasis3 MoreZia3 and Python. The assignment of given species within a particular genus is also a matter of conflict. -

Investigations Into the Presence of Nidoviruses in Pythons Silvia Blahak1, Maria Jenckel2,3, Dirk Höper2, Martin Beer2, Bernd Hoffmann2 and Kore Schlottau2*
Blahak et al. Virology Journal (2020) 17:6 https://doi.org/10.1186/s12985-020-1279-5 RESEARCH Open Access Investigations into the presence of nidoviruses in pythons Silvia Blahak1, Maria Jenckel2,3, Dirk Höper2, Martin Beer2, Bernd Hoffmann2 and Kore Schlottau2* Abstract Background: Pneumonia and stomatitis represent severe and often fatal diseases in different captive snakes. Apart from bacterial infections, paramyxo-, adeno-, reo- and arenaviruses cause these diseases. In 2014, new viruses emerged as the cause of pneumonia in pythons. In a few publications, nidoviruses have been reported in association with pneumonia in ball pythons and a tiger python. The viruses were found using new sequencing methods from the organ tissue of dead animals. Methods: Severe pneumonia and stomatitis resulted in a high mortality rate in a captive breeding collection of green tree pythons. Unbiased deep sequencing lead to the detection of nidoviral sequences. A developed RT-qPCR was used to confirm the metagenome results and to determine the importance of this virus. A total of 1554 different boid snakes, including animals suffering from respiratory diseases as well as healthy controls, were screened for nidoviruses. Furthermore, in addition to two full-length sequences, partial sequences were generated from different snake species. Results: The assembled full-length snake nidovirus genomes share only an overall genome sequence identity of less than 66.9% to other published snake nidoviruses and new partial sequences vary between 99.89 and 79.4%. Highest viral loads were detected in lung samples. The snake nidovirus was not only present in diseased animals, but also in snakes showing no typical clinical signs. -

Carpet Python Morelia Spilota (Lacépède, 1804) Including Undisturbed Remnant Bushland Near Perth and the Darling Size Ranges, Yanchep National Park, and Garden Island
Carpet Python Morelia spilota (Lacépède, 1804) including undisturbed remnant bushland near Perth and the Darling Size Ranges, Yanchep National Park, and Garden Island. Populations also occur on St Francis Island (South Australia), and islands of the Averages 2.0 m total length, though individuals have been reported Archipelago of the Recherche (Western Australia). to 4.0 m in length. Morelia spilota variegata Weight Distributed across South Australia, Victoria, inland NSW, Morelia spilota imbricata Queensland, Northern Territory, and the Kimberley region of Western Australia. Males For further information regarding the distribution of this species Up to 1.1 kg please refer to www.naturemap.dec.wa.gov.au Females Up to 4.5 kg Habitat Subspecies Photo: Babs & Bert Wells/DEC Morelia spilota variegata Occurs in mesic (areas with moderate amounts of moisture) to semi- Three subspecies are currently recognised: arid habitats, from the Kimberley region to northern Victoria. • Morelia spilota imbricata (southern Western Australia and eastern South Australia) Morelia spilota imbricata • Morelia spilota spilota (eastern NSW and lowland New Guinea) This subspecies has been recorded in semi-arid coastal and inland habitats consisting of Banksia woodland, eucalypt woodlands, and • Morelia spilota variegata (remainder of range including northern grasslands. Western Australia) Behaviour Description In the summer months, the Carpet Python is active either at night, or Colour patterns vary across their geographic range. In Western at dawn and dusk. In cooler months it may be active during the Australia, the colour varies from pale to dark brown, with blackish daytime and occasionally has been seen to bask in the sun on cool blotches or variegations, which may form cross bands. -

Israel's System for Risk Assessment of Imported Wildlife for the Pet Trade
Israel ’s System for Risk Assessment of Imported Wildlife for the Pet Trade Dr. Simon Nemtzov Israel Nature and Parks Authority Jerusalem, Israel [email protected] 1 Univ. Notre Dame – April 2008 Israel is especially susceptible to invasive species because of its rich diversity of habitats and ecosystems. Why does Israel have such a high level of biodiversity? Species per m 2 in Mediterranean countries Eurostat 2008 2 1 EUROPE ASIA AFRICA 3 Biogeography of Israel Northern Israel: – Mediterranean ecosystem – Up to 1000 mm rainfall Central Israel Iraq – Dense urban population Israel Southern Israel: – Sudanese desert ecosystem – < 100 mm rainfall – Relatively low human impact Saudi Arabia 40 miles / 60 km 4 2 Israel ’s geographic factors Small area: ~21,700 km 2 (~ 8,400 sq mi) – (about the size of New Jersey) Intersection of 3 continents: – Asia, Africa and Europe – 4 biogeographical regions: Rich diversity of ecotones and biota Sea of Galilee - Lake Kinneret 5 Wildlife biodiversity in Israel 16 species of Carnivores: Striped hyena (Hyena hyena ) 5 species of canids: wolf (Canis lupus ), 3 foxes, golden jackal (C. aureus ) 5 sp. of mustelids : 2 badgers, beech marten, marbled polecat, otter (Lutra lutra ) Egyptian mongoose (Herpestes ichneumon ) 4 species of felids 6 3 Wildlife biodiversity in Israel 4 species of felids: Caracal (Felis caracal ) Leopard (Panthera pardus ) Wild cat (Felis silvestris ) Jungle cat (Felis chaus ) (Sand cat (Felis margarita) ) 7 Risk Assessment Procedure Simplified system based on Australia ’s system (Bomford 1991, 2003) Importer requests an import permit from INPA No application fee! INPA ecologist collects biological data (answers “The Questions ”), prepares opinion, and assigns initial risk category (H / M / L) 3 ecologist referees → Consensus category Coypu 8 4 The risk assessment questions 1. -
Diamond Python Morelia Spilota Spilota
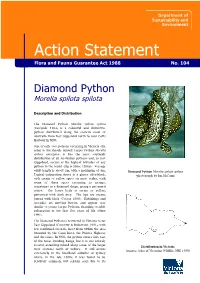
Action Statement FloraFlora and and Fauna Fauna Guarantee Guarantee Act Act 1988 1988 No. No. ### 104 Diamond Python Morelia spilota spilota Description and Distribution The Diamond Python Morelia spilota spilota (Lacépède 1804) is a colourful and distinctive python distributed along the eastern coast of Australia from East Gippsland north to near Coffs Harbour in NSW. One of only two pythons occurring in Victoria (the other is the closely related Carpet Python Morelia spilota variegata), it has the most southerly distribution of all Australian pythons and, in East Gippsland, occurs at the highest latitudes of any python in the world (Slip & Shine 1988d). Average adult length is about 2m, with a maximum of 4m. Diamond Python Morelia spilota spilota Typical colouration above is a glossy olive-black, (photograph by Ian McCann) with cream or yellow spots on most scales, with some of these spots occurring as groups, sometimes in a diamond shape, giving a patterned effect. The lower body is cream or yellow, patterned with dark grey. The lips are cream, barred with black (Cogger 1996). Hatchlings and juveniles are mottled brown, and appear very similar to young Carpet Pythons, changing to adult colouration in the first few years of life (Shine 1991). The Diamond Python is restricted in Victoria to far East Gippsland (Coventry & Robertson 1991), with few confirmed records, most from within the area bounded by the Cann River, the Princes Highway and the coast. In NSW, the python occurs only east of the Great Dividing Range, but it is not entirely coastal, extending inland along some of the larger Distribution in Victoria river systems north of Sydney. -

The Discovery of XY Sex Chromosomes in a Boa and Python
Current Biology, Volume 27 Supplemental Information The Discovery of XY Sex Chromosomes in a Boa and Python Tony Gamble, Todd A. Castoe, Stuart V. Nielsen, Jaison L. Banks, Daren C. Card, Drew R. Schield, Gordon W. Schuett, and Warren Booth Figure S1. PCR validation of male-specific RAD markers in boa and python. Related to Figure 1. A. Male-biased amplification of RAD marker TCBoa_2918 in eleven male and eleven female Boa imperator. Individual specimen ID numbers are listed below the gel image. B. Male-biased amplification of RAD marker TCBoa_2918 in an additional eight male and eleven female Boa imperator. Individual specimen ID numbers are listed below the gel image. C. Photograph of South American Boa (Boa constrictor) from Goiás, Brazil. D. Male-biased amplification of RAD marker TCBoa_2918 in three male and three female Boa constrictor. Individual specimen ID numbers are listed below the gel image. E. Male-biased amplification of RAD marker M3 in twelve male and twelve female Python bivittatus. Individual specimen ID numbers are listed below the gel image in panel F. F. Male-specific restriction digest of PCR amplicon (PCR-RFLP) from RAD marker M10 in twelve male and twelve female Python bivittatus. Individual specimen ID numbers are listed below the gel image. G. Cartoon illustrating PCR amplicons from the python RAD marker M10. The X and Y alleles are illustrated including the approximate position of the Y chromosome-specific SpeI restriction site. H. Gel image of python RAD marker M10 showing difference between digested and undigested PCR amplicons from a male Python bivittatus. -

Spatial Ecology of a Threatened Python (Morelia Spilota Imbricata) and the Effects of Anthropogenic Habitat Change
Austral Ecology (2005) 30, 261–274 Spatial ecology of a threatened python (Morelia spilota imbricata) and the effects of anthropogenic habitat change D. PEARSON,1 R. SHINE2* AND A. WILLIAMS1 1Department of Conservation and Land Management, Wanneroo, Western Australia, Australia and 2School of Biological Sciences A08, University of Sydney, Sydney, New South Wales 2006, Australia (Email: [email protected]) Abstract Large predators play important ecological roles, but often are sensitive to habitat changes and thus are early casualties of habitat perturbation. Pythons are among the largest predators in many Australian environments, and hence warrant conservation-orientated research. Carpet pythons (Morelia spilota imbricata) have declined across much of south-western Australia presumably because of habitat clearance and degradation. Information on habitat use, home range sizes and movements is needed to plan for the conservation of this important predator. We studied pythons at two study sites (Garden Island and Dryandra Woodland) with markedly different climates, habitat types and disturbance histories. We surgically implanted radio-transmitters in 91 pythons and tracked them for periods of 1 month to 4 years. Dryandra pythons remained inactive inside tree hollows during cooler months (May–September), whereas some (especially small) pythons on Garden Island continued to move and feed. Overall weekly displacements (mean = 100–150 m) were similar at the two study sites and among sex/ age classes, except that reproductive females were sedentary during summer while they were incubating eggs. Home ranges averaged 15–20 ha. Adult male pythons had larger home ranges than adult females at Dryandra, but not at Garden Island. Radio-tracked snakes at Dryandra exhibited high site fidelity, returning to previously occupied logs after long absences and reusing tree hollows for winter shelter. -
G Iant Snakes
Copyrighted Material Some pages are omitted from this book preview. Giant Snakes Giant Giant Snakes A Natural History John C. Murphy & Tom Crutchfield Snakes, particularly venomous snakes and exceptionally large constricting snakes, have haunted the human brain for a millennium. They appear to be responsible for our excellent vision, as well as the John C. Murphy & Tom Crutchfield & Tom C. Murphy John anxiety we feel. Despite the dangers we faced in prehistory, snakes now hold clues to solving some of humankind’s most debilitating diseases. Pythons and boas are capable of eating prey that is equal to more than their body weight, and their adaptations for this are providing insight into diabetes. Fascination with snakes has also drawn many to keep them as pets, including the largest species. Their popularity in the pet trade has led to these large constrictors inhabiting southern Florida. This book explores what we know about the largest snakes, how they are kept in captivity, and how they have managed to traverse ocean barriers with our help. Copyrighted Material Some pages are omitted from this book preview. Copyrighted Material Some pages are omitted from this book preview. Giant Snakes A Natural History John C. Murphy & Tom Crutchfield Copyrighted Material Some pages are omitted from this book preview. Giant Snakes Copyright © 2019 by John C. Murphy & Tom Cructhfield All rights reserved. No part of this book may be reproduced in any form or by any electronic or mechanical means including information storage and retrieval systems, without permission in writing from the publisher. Printed in the United States of America First Printing March 2019 ISBN 978-1-64516-232-2 Paperback ISBN 978-1-64516-233-9 Hardcover Published by: Book Services www.BookServices.us ii Copyrighted Material Some pages are omitted from this book preview. -

NSW REPTILE KEEPERS' LICENCE Species Lists 1006
NSW REPTILE KEEPERS’ LICENCE SPECIES LISTS (2006) The taxonomy in this list follows that used in Wilson, S. and Swan, G. A Complete Guide to Reptiles of Australia, Reed 2003. Common names generally follow the same text, when common names were used, or have otherwise been lifted from other publications. As well as reading this species list, you will also need to read the “NSW Reptile Keepers’ Licence Information Sheet 2006.” That document has important information about the different types of reptile keeper licenses. It also lists the criteria you need to demonstrate before applying to upgrade to a higher class of licence. THESE REPTILES CAN ONLY BE HELD UNDER A REPTILE KEEPERS’ LICENCE OF CLASS 1 OR HIGHER Code Scientific Name Common Name Code Scientific Name Common Name Turtles Monitors E2018 Chelodina canni Cann’s Snake-necked Turtle G2263 Varanus acanthurus Spiney-tailed Monitor C2017 Chelodina longicollis Snake-necked Turtle Q2268 Varanus gilleni Pygmy Mulga Monitor G2019 Chelodina oblonga Oblong Turtle G2271 Varanus gouldii Sand Monitor Y2028 Elseya dentata Northern Snapping Turtle M2282 Varanus tristis Black-Headed Monitor K2029 Elseya latisternum Saw-shelled Turtle Y2776 Elusor macrurus Mary River Turtle E2034 Emydura macquarii Murray Short-necked Turtle Skinks T2031 Emydura macquarii dharra Macleay River Turtle A2464 Acritoscincus platynotum Red-throated Skink T2039 Emydura macquarii dharuk Sydney Basin Turtle W2331 Cryptoblepharus virgatus Cream-striped Wall Skink T2002 Emydura macquarii emmotti Emmott’s Short-necked Turtle W2375 -

Genus Antaresia
MONITOR - JOURNAL OF THE VICTORIAN HERPETOLOGICAL SOCIETY 10 (2/3) 1999:24-32MONITOR Copyright - JOURNALVictorian OFHerpetological THE VICTORIAN Society HERPETOLOGICAL SOCIETY 10 (2/3) 1999 AUSTRALIA’S DWARF PYTHONS – GENUS ANTARESIA RAYMOND T. HOSER 41 Village Avenue, Doncaster, Victoria, 3108, Australia. Phone:+61 3 9857-4491 Fax: +61 3 9857-4664 E-mail: [email protected] INTRODUCTION comment as dogma, readers should be aware that it Australia’s dwarf pythons were, until the early 1980’s, has been argued by some that the Wells and Wellington classified by most herpetologists as a single species, description was inadequate in terms of diagnostic namely the Children’s Python (Liasis childreni). An information and is therefore invalid. Wells and 1873 classification of the eastern form ‘maculosus’ had Wellington counter that their information as printed is long been regarded as being a junior synonym and sufficient as per ICZN rules, particularly when thus a part of the same species. Few herpetologists in referenced with the specimen lodged at a public the early 1980’s were even aware that such a synonymy museum, to wit the Australian Museum in Sydney. even existed. However the preceding dispute is probably not the main Things began to change when in 1981 I wrote a paper reason why the Wells and Wellington name wasn’t formally describing the Western Australian form as a adopted by most authors following its publication. You new species. At the same time I also sought to see shortly thereafter there was a petition to the ICZN redescribe the Ant-hill Python as Liasis perthensis (as by a substantial number of Australian herpetologists a full species) in a separate paper, which was by that that called for the complete suppression of three works stage erroneously regarded by most as being an invalid by Wells and Wellington (1984, 1985a, 1985b), which name applied to western populations of the so-called included the one relevant here. -
Review of Species Selected on the Basis of the Analysis of 2016 CITES Export Quotas
UNEP-WCMC technical report Review of species selected on the basis of the Analysis of 2016 CITES export quotas (Version edited for public release) Review of species selected on the basis of the Analysis of 2016 CITES export quotas. Prepared for The European Commission, Directorate General Environment, Directorate E - Global & Regional Challenges, LIFE ENV.E.2. – Global Sustainability, Trade & Multilateral Agreements, Brussels, Belgium Published September 2016 Copyright European Commission 2016 Citation UNEP-WCMC. 2016. Review of species selected on the basis of the Analysis of 2016 CITES export quotas. UNEP-WCMC, Cambridge. The UNEP World Conservation Monitoring Centre (UNEP-WCMC) is the specialist biodiversity assessment centre of the United Nations Environment Programme, the world’s foremost intergovernmental environmental organization. The Centre has been in operation for over 30 years, combining scientific research with policy advice and the development of decision tools. We are able to provide objective, scientifically rigorous products and services to help decision-makers recognize the value of biodiversity and apply this knowledge to all that they do. To do this, we collate and verify data on biodiversity and ecosystem services that we analyze and interpret in comprehensive assessments, making the results available in appropriate forms for national and international level decision-makers and businesses. To ensure that our work is both sustainable and equitable we seek to build the capacity of partners where needed, so that they can provide the same services at national and regional scales. The contents of this report do not necessarily reflect the views or policies of UNEP, contributory organisations or editors. The designations employed and the presentations do not imply the expressions of any opinion whatsoever on the part of UNEP, the European Commission or contributory organisations, editors or publishers concerning the legal status of any country, territory, city area or its authorities, or concerning the delimitation of its frontiers or boundaries. -

Super Glue As a Means to Fix Open Wounds in Reptiles
62 Australasian Journal of Herpetology Australasian Journal of Herpetology 40:62-64. Published 10 July 2019. ISSN 1836-5698 (Print) ISSN 1836-5779 (Online) Hi-tech medicine and surgery! Super Glue as a means to fix open wounds in reptiles. LSID urn:lsid:zoobank.org:pub:35D5C9BA-CDC4-4BC8-878D-FFBE32C26D7F RAYMOND T. HOSER 488 Park Road, Park Orchards, Victoria, 3134, Australia. Phone: +61 3 9812 3322 Fax: 9812 3355 E-mail: snakeman (at) snakeman.com.au Received 20 May 2018, Accepted 30 June 2019, Published 10 July 2019. ABSTRACT Stitching large lesions in emaciated small reptiles poses logistical problems in that the skin is too weak to hold the sutures required to keep the wound shut. As a means to get over the problem, commercially available “Super Glue”, a common type of quick drying super strength glue, as sold in shops has been found to be a quick and effective means to seal gaping wounds by joining skin tight with healing success the usual outcome. Keywords: Snake; python; Olive Python; Centralian Carpet Python Liasis olivaceous; Morelia bredli; Australia; super glue; open wounds; sealing. DETAIL Over more than two decades, I have used so-called “Super While the snake had been hatched a year prior, it had not eaten Glue” as means to seal wounds in snakes and lizards that would for most of the previous year and so had only grown slightly otherwise be difficult to suture up in the usual way. since hatching and was extremely thin. While there are numerous examples I can give, all of which have In effect the snake presented as a newborn sized snake in been successful (none unsuccessful), only a limited number of emaciated condition.