[ Captioner Standing by ] 1 >> the Broadcast Is Now Starting. All Attendees Are in Listen-Only Mode. >> JESSIE
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
06 4-15-14 TV Guide.Indd
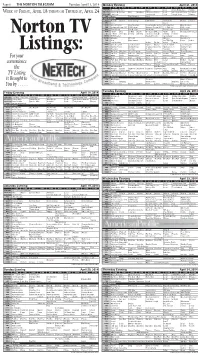
Page 6 THE NORTON TELEGRAM Tuesday, April 15, 2014 Monday Evening April 21, 2014 7:00 7:30 8:00 8:30 9:00 9:30 10:00 10:30 11:00 11:30 KHGI/ABC Dancing With Stars Castle Local Jimmy Kimmel Live Nightline WEEK OF FRIDAY, APRIL 18 THROUGH THURSDAY, APRIL 24 KBSH/CBS 2 Broke G Friends Mike Big Bang NCIS: Los Angeles Local Late Show Letterman Ferguson KSNK/NBC The Voice The Blacklist Local Tonight Show Meyers FOX Bones The Following Local Cable Channels A&E Duck D. Duck D. Duck Dynasty Bates Motel Bates Motel Duck D. Duck D. AMC Jaws Jaws 2 ANIM River Monsters River Monsters Rocky Bounty Hunters River Monsters River Monsters CNN Anderson Cooper 360 CNN Tonight Anderson Cooper 360 E. B. OutFront CNN Tonight DISC Fast N' Loud Fast N' Loud Car Hoards Fast N' Loud Car Hoards DISN I Didn't Dog Liv-Mad. Austin Good Luck Win, Lose Austin Dog Good Luck Good Luck E! E! News The Fabul Chrisley Chrisley Secret Societies Of Chelsea E! News Norton TV ESPN MLB Baseball Baseball Tonight SportsCenter Olbermann ESPN2 NFL Live 30 for 30 NFL Live SportsCenter FAM Hop Who Framed The 700 Club Prince Prince FX Step Brothers Archer Archer Archer Tomcats HGTV Love It or List It Love It or List It Hunters Hunters Love It or List It Love It or List It HIST Swamp People Swamp People Down East Dickering America's Book Swamp People LIFE Hoarders Hoarders Hoarders Hoarders Hoarders Listings: MTV Girl Code Girl Code 16 and Pregnant 16 and Pregnant House of Food 16 and Pregnant NICK Full H'se Full H'se Full H'se Full H'se Full H'se Full H'se Friends Friends Friends SCI Metal Metal Warehouse 13 Warehouse 13 Warehouse 13 Metal Metal For your SPIKE Cops Cops Cops Cops Cops Cops Cops Cops Jail Jail TBS Fam. -

The Porn Circuit Understand Your Brain and Break Porn Habits in 90 Days XXX
XXX tHe porn Circuit Understand your brain and break porn habits in 90 days XXX Table of Contents Introduction: Stop Looking at Porn, You Sicko! 3 www.covenanteyes.com Chapter 1: Your Sexy Plastic Brain 6 1.877.479.1119 1525 W. King St., PO Box 637 Chapter 2: Owosso, MI 48867 Your Brain’s Sexual Cocktail 9 Copyright © 2013 Covenant Eyes, Inc. All rights reserved. Chapter 3: Stuck in a Rut 14 You are free to distribute print copies of this e-book to anyone you choose. As a courtesy, e-mail us at [email protected] Chapter 4: and let us know you are doing this so we can 32 Flavors: Why We Like Sexual Variety 20 keep you informed of other similar resources. To distribute this e-book electronically, we ask that you share the page: Chapter 5: www.covenanteyes.com/science-of-porn- Ain’t Nothing Like the Real Thing, Baby 24 addiction-ebook For more information about sharing our Chapter 6: materials electronically, see: Habits of Freedom 29 www.covenanteyes.com/permissions-policy/ Resources that can help 42 Endnotes 44 About The Author: Sam Black Sam Black is an Internet Safety Consultant and a manager at Covenant Eyes. He joined the Covenant Eyes team in 2007 after 18 years as a journalist, serving as a reporter and editor for newspapers and magazines in six states. He has been married for 17 years and is a father of two. The Porn Circuit | 2 XXX Introduction: Stop Looking at Porn, You Sicko! Comedian Bob Newhart has been making people laugh for decades. -
Heartthrob Can't Inject Life Into Latest Nicholas Sparks Tale
PAGE b8 THE STATE JOURNAL Ap RiL 19, 2012 Thursday ALMANAC 50 YEARS AGO Danny Rodgers set a new ‘Lucky One’ not Zac Efron school record for the high jump and Frankie Brown picked up 10 individual points in two hurdles events Heartthrob can’t inject life into latest Nicholas Sparks tale to lead the Franklin County Flyers to a 71.5 to 46.5 victory over Clark County in a dual By RogeR MooRe (Blythe Danner). Zac track meet at Kentucky State McT clA chy-TriBune news service Logan (Zac Efron) is a Efron College’s Alumni Field. brooding ex-soldier, and “The Lucky One” is the attends chivalrous. edgiest-ever film adaptation Warner 25 YEARS AGO “Isn’t he chivalrous, dear?” of the writings of Nicholas Bros. Franklin County School granny says, elbowing Beth. Sparks. Pic- board members attended Which isn’t saying much. And the viewer. tures the Kentucky School Boards Logan met Beth before she Yeah, it has the violence of “The Association conference in knew it. He found her photo Louisville. Mac Quarles, war, and the heat of near-sex. Lucky And profanity! Don’t forget in the dust after a fierce fire- Jack Badgett, Billy Perkins, fight in Iraq. He lost comrades One” Dr. Harry Cowherd and Lee the profanity! pre- But it still has the ro- that day, and one of them had Troutwine heard speakers miere mance novelist’s favorite her photo. Somehow, Logan offering national and state- tropes – most of them, any- manages to track Beth down held at wide perspectives on issues way. -
A Decade of Deceit How TV Content Ratings Have Failed Families EXECUTIVE SUMMARY Major Findings
A Decade of Deceit How TV Content Ratings Have Failed Families EXECUTIVE SUMMARY Major Findings: In its recent report to Congress on the accuracy of • Programs rated TV-PG contained on average the TV ratings and effectiveness of oversight, the 28% more violence and 43.5% more Federal Communications Commission noted that the profanity in 2017-18 than in 2007-08. system has not changed in over 20 years. • Profanity on PG-rated shows included suck/ Indeed, it has not, but content has, and the TV blow, screw, hell/damn, ass/asshole, bitch, ratings fail to reflect “content creep,” (that is, an bastard, piss, bleeped s—t, bleeped f—k. increase in offensive content in programs with The 2017-18 season added “dick” and “prick” a given rating as compared to similarly-rated to the PG-rated lexicon. programs a decade or more ago). Networks are packing substantially more profanity and violence into youth-rated shows than they did a decade ago; • Violence on PG-rated shows included use but that increase in adult-themed content has not of guns and bladed weapons, depictions affected the age-based ratings the networks apply. of fighting, blood and death and scenes We found that on shows rated TV-PG, there was a of decapitation or dismemberment; The 28% increase in violence; and a 44% increase in only form of violence unique to TV-14 rated profanity over a ten-year period. There was also a programming was depictions of torture. more than twice as much violence on shows rated TV-14 in the 2017-18 television season than in the • Programs rated TV-14 contained on average 2007-08 season, both in per-episode averages and 84% more violence per episode in 2017-18 in absolute terms. -

Candidates Gearing up for Election by Erik Burriss "But Not Without Leadership," She Said
The island's newspaper of record ' Business Expo page 12A Week of November 26-December 3,2003 SANIBEL&CAPTIVA, FLORIDA VOLUME 30, NUMBER 47, 36 PAGES. TWO SECTIONS 75 CENTS Candidates gearing up for election By Erik Burriss "But not without leadership," she said. Managing editor "Leadership that rises above rhetoric and S,t • -<r"- partisanship and ideology." It seems like she's just about every other Veterans have expressed concern to her job in state and local politics, now Betty about the way they have been treated, she Castor wants the Senate seat that will said. While in the process of visiting every become vacant with the retirement of Bob Veterans Affairs hospital and clinic in Graham. Florida, she has learned it takes six months Castor was the guest of honor at a Nov. or longer for a veteran to get a primary care 15 lunch hosted by the Democratic Club of appointment. the Islands at the Helm's Club in South Fort "I think this is an opportunity for the Myers. 30 minute speech. Democrats to say we will treat you better," ' v ;H- .;. She got her start in politics almost 30 Castor said. '"We will take better care of years ago as a Hillsborough county com- you." missioner. Since then, she has been elected While the recently passed veterans care to the state Senate — where she was the bill sounds good, she said, it will take 10 first woman president pro tempore — and years to put in place. served in the Cabinet as education commis- Similarly, Castor said the Reserve and sioner. -

Porn Sex Vs. Real Sex: Exploring Pornography's Impact on Sexual Behaviors, Attitudes, and Relationships
Georgia State University ScholarWorks @ Georgia State University Sociology Dissertations Department of Sociology Spring 5-10-2014 Porn Sex vs. Real Sex: Exploring Pornography's Impact on Sexual Behaviors, Attitudes, and Relationships Stacy Gorman Follow this and additional works at: https://scholarworks.gsu.edu/sociology_diss Recommended Citation Gorman, Stacy, "Porn Sex vs. Real Sex: Exploring Pornography's Impact on Sexual Behaviors, Attitudes, and Relationships." Dissertation, Georgia State University, 2014. https://scholarworks.gsu.edu/sociology_diss/76 This Dissertation is brought to you for free and open access by the Department of Sociology at ScholarWorks @ Georgia State University. It has been accepted for inclusion in Sociology Dissertations by an authorized administrator of ScholarWorks @ Georgia State University. For more information, please contact [email protected]. PORN SEX VS. REAL SEX: EXPLORING PORNOGRAPHY’S IMPACT ON SEXUAL BEHAVIORS, ATTITUDES, AND RELATIONSHIPS by STACY GORMAN Under the Direction of Wendy Simonds ABSTRACT For over forty years, researchers, activists, and policymakers have questioned how, if at all, pornography affects its viewers. Previous research has focused on how pornography relates to many factors including sexual risks, sexual permissiveness, violence, rape myth acceptance, and sexual behaviors. Much of this research, though, has been unable to identify the direction of the relationship between viewing sexually explicit material and various sexual attitudes and behaviors, and rarely studies a sample that is representative of the U.S. adult population. Instead, much of the research on pornography has relied on college student samples or other convenience samples. My study addresses these gaps by exploring a wide range of sexual behaviors and attitudes through surveying a sample of respondents who participate in online survey research panels. -
1-3 Front CFP 4-6-11.Indd 2 4/6/11 1:22:43 PM
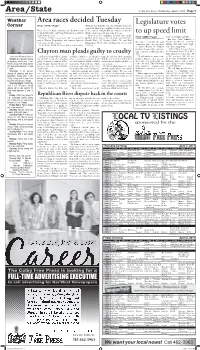
Area/State Colby Free Press Wednesday, April 6, 2011 Page 3 Weather Area races decided Tuesday Legislature votes Corner From “VOTE,” Page 1 Williams has held the seat since Dennis Allison re- signed. R. Alan Jones and Matt Vogler were elected There were no fi led candidates for Brewster City to the council. Dwight Williams was elected to the Council. Bill Selby and Craig Fulwider won with 19 third council seat with fi ve write-in votes. to up speed limit and 8 write-in votes. There were fi ve candidates for four seats on the From “LIMIT,” Page 1 In Gem, Phyllis Ziegelmeier was re-elected as Golden Plains School Board. Vogler got 84 votes; state’s total highway miles. mayor. Warren Ziegelmeier and Annette Spresser Brandi Wark, 97; Jeremy Schiltz, 78; and Paul But Sen. Vicki Schmidt, a were elected to the council. Bruggeman, 98. Joe Broeckelman missed out with the state’s economy. He said Topeka Republican, said the In Rexford, David Williams was elected mayor. 73 votes. companies have an incentive change will make major high- to bypass Kansas in shipping ways more dangerous. products because they can save “I think when the speed lim- time with routes through other it’s 70, people drive 75 or 80. I Clayton man pleads guilty to cruelty states. think when it’s 75, they drive 80 National Weather Service A Clayton man will be spend- on Friday, March 6, the sheriff’s farm, he said, but after consulting “It will make us more com- or 85,” she said. -

Racialized Sexualities Within the Romance Tour Industry: the Influence of Affect and Emotion Upon Transnational Hierarchies of Desire Julia H
Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 6-24-2014 Racialized Sexualities within the Romance Tour Industry: the Influence of Affect and Emotion Upon Transnational Hierarchies of Desire Julia H. Meszaros Florida International University, [email protected] DOI: 10.25148/etd.FI14071123 Follow this and additional works at: https://digitalcommons.fiu.edu/etd Recommended Citation Meszaros, Julia H., "Racialized Sexualities within the Romance Tour Industry: the Influence of Affect and Emotion Upon Transnational Hierarchies of Desire" (2014). FIU Electronic Theses and Dissertations. 1458. https://digitalcommons.fiu.edu/etd/1458 This work is brought to you for free and open access by the University Graduate School at FIU Digital Commons. It has been accepted for inclusion in FIU Electronic Theses and Dissertations by an authorized administrator of FIU Digital Commons. For more information, please contact [email protected]. FLORIDA INTERNATIONAL UNIVERSITY Miami, Florida RACIALIZED SEXUALITIES WITHIN THE ROMANCE TOUR INDUSTRY: THE INFLUENCE OF AFFECT AND EMOTION UPON TRANSNATIONAL HIERARCHIES OF DESIRE A dissertation submitted in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY in GLOBAL AND SOCIOCULTURAL STUDIES by Julia Meszaros 2014 To: Interim Dean Michael R. Heithaus College of Arts and Sciences This dissertation, written by Julia Meszaros, and entitled Racialized Sexualities within the Romance Tour Industry: the Influence of Affect and Emotion -
Sunday Morning Grid 11/23/14 Latimes.Com/Tv Times
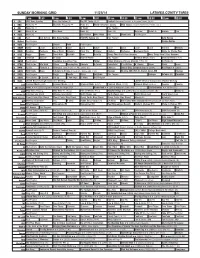
SUNDAY MORNING GRID 11/23/14 LATIMES.COM/TV TIMES 7 am 7:30 8 am 8:30 9 am 9:30 10 am 10:30 11 am 11:30 12 pm 12:30 2 CBS CBS News Sunday Face the Nation (N) The NFL Today (N) Å Football Cincinnati Bengals at Houston Texans. (N) Å 4 NBC News (N) Å Meet the Press (N) Å News (N) World/Adventure Sports MLS Soccer: Eastern Conference Finals, Leg 1 5 CW News (N) Å In Touch Paid Program 7 ABC News (N) Å This Week News (N) News (N) News Å Vista L.A. Explore Paid 9 KCAL News (N) Joel Osteen Mike Webb Paid Woodlands Paid Program 11 FOX Paid Joel Osteen Fox News Sunday FOX NFL Sunday (N) Paid Program Auto Racing 13 MyNet Paid Program Pirates-Worlds 18 KSCI Paid Program Church Faith Paid Program 22 KWHY Como Local Jesucristo Local Local Gebel Local Local Local Local Transfor. Monkey 24 KVCR Painting Dewberry Joy of Paint Wyland’s Paint This Painting Kitchen Barbecue Heirloom Meals Home for Christy Rost 28 KCET Raggs Space Travel-Kids Biz Kid$ News Asia Biz Things That Aren’t Here Anymore More Things Aren’t Here Anymore 30 ION Jeremiah Youssef In Touch Hour Of Power Paid Program Criminal Minds (TV14) Criminal Minds (TV14) 34 KMEX Paid Program República Deportiva (TVG) Fútbol Fútbol Mexicano Primera División (9:50) (N) Al Punto (N) 40 KTBN Walk in the Win Walk Prince Redemption Liberate In Touch PowerPoint It Is Written B. Conley Super Christ Jesse 46 KFTR Tu Dia Fórmula 1 Fórmula 1 Gran Premio de Abu Dhabi. -
Bulletin of Duke University Summer Session 2010 University’S Mission Statement James B
bulletin of Duke University Summer Session 2010 University’s Mission Statement James B. Duke’s founding Indenture of Duke University directed the members of the University to “provide real leadership in the educational world” by choosing individuals of “outstanding character, ability and vision” to serve as its officers, trustees and faculty; by carefully selecting students of “character, determination and application;” and by pursuing those areas of teaching and scholarship that would “most help to develop our resources, increase our wisdom, and promote human happiness.” To these ends, the mission of Duke University is to provide a superior liberal education to undergraduate students, attending not only to their intellectual growth but also to their development as adults committed to high ethical standards and full participation as leaders in their communities; to prepare future members of the learned professions for lives of skilled and ethical service by providing excellent graduate and professional education; to advance the frontiers of knowledge and contribute boldly to the international community of scholarship; to promote an intellectual environment built on a commitment to free and open inquiry; to help those who suffer, cure disease and promote health, through sophisticated medical research and thoughtful patient care; to provide wide ranging educational opportunities, on and beyond our campuses, for traditional students, active professionals and life-long learners using the power of information technologies; and to promote a deep appreciation for the range of human difference and potential, a sense of the obligations and rewards of citizenship, and a commitment to learning, freedom and truth. By pursuing these objectives with vision and integrity, Duke University seeks to engage the mind, elevate the spirit, and stimulate the best effort of all who are associated with the University; to contribute in diverse ways to the local community, the state, the nation and the world; and to attain and maintain a place of real leadership in all that we do. -

The New Sex Worker in American Popular Culture, 2006-2016
BEYOND THE MARKED WOMAN: THE NEW SEX WORKER IN AMERICAN POPULAR CULTURE, 2006-2016 By Lauren Kirshner Bachelor of Education, University of Toronto, 2009 Master of Arts, University of Toronto, 2007 Honours Bachelor of Arts, University of Toronto, 2005 A dissertation presented to Ryerson University and York University in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the joint program of Communication and Culture Toronto, Ontario, Canada, 2019 © Lauren Kirshner, 2019 AUTHOR’S DECLARATION FOR ELECTRONIC SUBMISSION OF A DISSERTATION I hereby declare that I am the sole author of this dissertation. This is a true copy of the dissertation, including any required final revision, as required by my examiners. I authorize Ryerson University to lend this dissertation to other institutions or individuals for the purpose of scholarly research. I further authorize Ryerson University to lend this dissertation by photocopying or by other means, in total or in part, at the request of other institutions or individuals for the purpose of scholarly research. I understand that my dissertation may be made electronically available to the public. ii BEYOND THE MARKED WOMAN: THE NEW SEX WORKER IN AMERICAN POPULAR CULTURE, 2006-2016 Doctor of Philosophy 2019 Lauren Kirshner Communication and Culture, Ryerson University and York University This dissertation argues that between 2006 and 2016, in a context of rising tolerance for sex workers, economic shifts under neoliberal capitalism, and the normalization of transactional intimate labour, popular culture began to offer new and humanizing images of the sex worker as an entrepreneur and care worker. This new popular culture legitimatizes sex workers in a growing services industry and carries important de-stigmatizing messages about sex workers, who continue to be among the most stigmatized of women workers in the U.S. -

Sex Trafficking: a Gender-Based Violation of Civil Rights
U.S. COMMISSION ON CIVIL RIGHTS SEX TRAFFICKING: A GENDER-BASED CIVIL RIGHTS VIOLATION BRIEFING REPORT U.S. COMMISSION ON CIVIL RIGHTS Washington, DC 20425 Official Business SEPTEMBER 2014 Penalty for Private Use $300 Visit us on the Web: www.usccr.gov U.S. COMMISSION ON CIVIL RIGHTS MEMBERS OF THE COMMISSION The U.S. Commission on Civil Rights is an independent, Martin R. Castro, Chairman bipartisan agency established by Congress in 1957. It is Abigail Thernstrom, Vice Chair (term expired November 2013) directed to: Roberta Achtenberg Todd F. Gaziano (term expired December 2013) • Investigate complaints alleging that citizens are Gail L. Heriot being deprived of their right to vote by reason of their Peter N. Kirsanow race, color, religion, sex, age, disability, or national David Kladney origin, or by reason of fraudulent practices. Michael Yaki • Study and collect information relating to discrimination or a denial of equal protection of the laws under the Constitution Marlene Sallo, Staff Director because of race, color, religion, sex, age, disability, or national origin, or in the administration of justice. U.S. Commission on Civil Rights 1331 Pennsylvania Ave NW Suite 1150 • Appraise federal laws and policies with respect to Washington, DC 20425 discrimination or denial of equal protection of the laws because of race, color, religion, sex, age, disability, or (202) 376-7700 national origin, or in the administration of justice. www.usccr.gov • Serve as a national clearinghouse for information in respect to discrimination or denial of equal protection of the laws because of race, color, religion, sex, age, disability, or national origin.