Out of Zone Enrolment Form
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
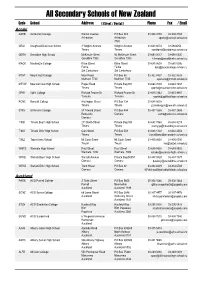
Secondary Schools of New Zealand
All Secondary Schools of New Zealand Code School Address ( Street / Postal ) Phone Fax / Email Aoraki ASHB Ashburton College Walnut Avenue PO Box 204 03-308 4193 03-308 2104 Ashburton Ashburton [email protected] 7740 CRAI Craighead Diocesan School 3 Wrights Avenue Wrights Avenue 03-688 6074 03 6842250 Timaru Timaru [email protected] GERA Geraldine High School McKenzie Street 93 McKenzie Street 03-693 0017 03-693 0020 Geraldine 7930 Geraldine 7930 [email protected] MACK Mackenzie College Kirke Street Kirke Street 03-685 8603 03 685 8296 Fairlie Fairlie [email protected] Sth Canterbury Sth Canterbury MTHT Mount Hutt College Main Road PO Box 58 03-302 8437 03-302 8328 Methven 7730 Methven 7745 [email protected] MTVW Mountainview High School Pages Road Private Bag 907 03-684 7039 03-684 7037 Timaru Timaru [email protected] OPHI Opihi College Richard Pearse Dr Richard Pearse Dr 03-615 7442 03-615 9987 Temuka Temuka [email protected] RONC Roncalli College Wellington Street PO Box 138 03-688 6003 Timaru Timaru [email protected] STKV St Kevin's College 57 Taward Street PO Box 444 03-437 1665 03-437 2469 Redcastle Oamaru [email protected] Oamaru TIMB Timaru Boys' High School 211 North Street Private Bag 903 03-687 7560 03-688 8219 Timaru Timaru [email protected] TIMG Timaru Girls' High School Cain Street PO Box 558 03-688 1122 03-688 4254 Timaru Timaru [email protected] TWIZ Twizel Area School Mt Cook Street Mt Cook Street -

New Zealand's Food Story the Pukekohe Hub Prepared For
Paerata Patumahoe Mauku Pukekohe Puni Pokeno Tuakau Aka Aka Te ohanga newhero Pukekawa New Zealand’s Food Story The Pukekohe Hub Prepared for Horticulture New Zealand August 2018 Foreword Horticulture is one of the success stories of New Zealand’s primary industries. In 2017, the industry generated $5.68 billion in value. Export revenue has grown nearly 50% in five years, illustrating the trust the world places in New Zealand-grown food, and the country’s ability to meet that demand. But the industry cannot rest. New Zealand faces opportunities with a growing population and the need to grow fresh produce. Nowhere is this more apparent than in Auckland, and its surrounding rural land. The population is set to rise to 2.3 million by 2043, straining natural resources and infrastructure. And growers are feeling that pressure. The Pukekohe growing hub straddles the Auckland and Waikato District boundaries, and it is key to sustaining the fresh food supply to the country’s largest city. The squeeze on prime growing land in the Pukekohe hub, access to water, and the tensions between the existing industry and new neighbourhoods all mean a more considered and concerted approach to planning is needed. It is the right time to start the conversation about New Zealand’s sustainable food supply with a focus on a growing area experiencing change. Our economic analysis suggests that, over the next 25 years, the Pukekohe hub could face constrained horticulture production. If left unchecked, less production could result in lost economic value, higher prices for customers, and job losses for the industry itself and the sectors it supports. -

Schools Advisors Territories
SCHOOLS ADVISORS TERRITORIES Gaynor Matthews Northland Gaynor Matthews Auckland Gaynor Matthews Coromandel Gaynor Matthews Waikato Angela Spice-Ridley Waikato Angela Spice-Ridley Bay of Plenty Angela Spice-Ridley Gisborne Angela Spice-Ridley Central Plateau Angela Spice-Ridley Taranaki Angela Spice-Ridley Hawke’s Bay Angela Spice-Ridley Wanganui, Manawatu, Horowhenua Sonia Tiatia Manawatu, Horowhenua Sonia Tiatia Welington, Kapiti, Wairarapa Sonia Tiatia Nelson / Marlborough Sonia Tiatia West Coast Sonia Tiatia Canterbury / Northern and Southern Sonia Tiatia Otago Sonia Tiatia Southland SCHOOLS ADVISORS TERRITORIES Gaynor Matthews NORTHLAND REGION AUCKLAND REGION AUCKLAND REGION CONTINUED Bay of Islands College Albany Senior High School St Mary’s College Bream Bay College Alfriston College St Pauls College Broadwood Area School Aorere College St Peters College Dargaville High School Auckland Girls’ Grammar Takapuna College Excellere College Auckland Seven Day Adventist Tamaki College Huanui College Avondale College Tangaroa College Kaitaia College Baradene College TKKM o Hoani Waititi Kamo High School Birkenhead College Tuakau College Kerikeri High School Botany Downs Secondary School Waiheke High School Mahurangi College Dilworth School Waitakere College Northland College Diocesan School for Girls Waiuku College Okaihau College Edgewater College Wentworth College Opononi Area School Epsom Girls’ Grammar Wesley College Otamatea High School Glendowie College Western Springs College Pompallier College Glenfield College Westlake Boys’ High -

VOLUME 1 Rural Fire Force and Community Volunteers, the Mayor and Principal Rural Fire Officer at the Groundbreaking for the New Hunua Fire Station
Franklin District Council Community Plan 2009 - 2019 WORKING TOGETHER FOR OUR FUTURE VOLUME 1 Rural fire force and community volunteers, the Mayor and Principal Rural Fire Officer at the groundbreaking for the new Hunua Fire Station. CONTENTS From the Mayor and CEO . 3 Representing You . 4 Management Team . 5 District Profile . 6 Key Decisions . 7 Guide to this Plan . 8 Community Outcomes . 9 Financial Overview . 15 Summary Financial Statements . 16 Funding Impact Statement . 20 Significant Assumptions . 28 Statement Of Accounting Policies . 34 Leading the Franklin District Strategic Planning and Policy . 44 Representation . 48 Growing the Franklin Economy Economic Development . 53 Town Centre Management . 57 Moving Around Franklin Transportation . 63 1 Protecting the Franklin Environment Emergency Management . 74 Regulatory . 78 Solid Waste . 83 Stormwater . 88 Wastewater . 97 Water Supply . 104 Living and Playing in Franklin Arts and Culture and Heritage . 118 Community Services . 122 Community Facilities . 128 Open Spaces . 135 Support Communications . 145 Corporate Property . 147 Corporate Support . 149 Financial Statements Income Statement . 156 Statement of Financial Position . 157 Statement of Movement in Equity . 158 Statement of Cash Flows . 159 Other Supporting Financial Information . 160 Glossary . 164 Appendix A Community Outcomes Indicators and Measures 2006 - 2009 . 166 Appendix B Auditor’s Letter . 169 2 3 FROM THE MAYOR AND CEO Community Plan 2009-19 has been a massive but satisfying task. It Council Accommodation Building – This project has been is fair to say that this work was made more difficult by two external removed from the Plan. factors: the world wide economic downturn and the changes to Auckland governance following the report of the Royal Commission Wastewater Funding Policy – The policy for this activity has been Mark Ball Sally Davis on Auckland Governance. -

Recruitment Information Form
Job Information Pack Position Summary Business Name: Kelliher Charitable Trust – Glencairn Property Summary: Glencairn is a 920ha Sheep and Beef property in North Waikato. The property was acquired by the Kelliher Charitable Trust in February 2014. Glencairn is the amalgamation of 3 properties. After completing the first stage of the development process the second stage has commenced. This second stage has a strong focus on environmental enhancement. During this second phase of development there will be an upgrade of fencing on one of the recently acquired blocks. The business is also establishing a dedicated cattle unit (this is not a techno system). Position Title: Senior Shepherd/Stock Manager Position Overview: As the Senior Shepherd/Stock Manager you will be working closely and reporting through to the Farm Manager. Glencairn has a farm plan in place and you will be working to this with support and guidance from the Farm Manager. The expectation is that you will take the lead with the stock management; this will include the pasture management, animal health and preparation for shearing and docking/weaning. A team of 4-5 working dogs will be required for this position and some previous horse experience would be helpful as there is the opportunity to use them for mustering. A strong understanding of lamb finishing, body condition scoring and the ability to work to timelines and achieve set KPI’s around the stock performance is required. You will need to measure and monitor pasture and complete feed budgets in order to understand your feed wedge. Part of this role will be General R&M work; this will include but is not limited to R&M fencing, water reticulation and handpiece work. -

On the Awaroa Ki Tuakau Map, 28 to 104 (Even Number Are on Mill Road)
“What number(s) on Mill Road is the Waikato District Council boundary” On the Awaroa ki Tuakau map, 28 to 104 (even number are on Mill Road). On the online maps the numbers are visible 28 through to 104. “What number(s) on Mill Road is the Waikato District Council boundary for Whangamarino Ward? Mill Road does not cross into Whangamarino Ward, Mill road runs between Harrisville Road (in Waikato District) and crosses into Auckland at 104 Mill Road. Mill road crosses SH1 and joins Bombay Road, These are still some distance way from Lyons Road which is where the Whangamarino Ward boundary. The orange marker is 104 Mill Road, the blue area to the East is Whangamarino. “What number on Mill Road is the Waikato District Council boundary for Awaroa ki Tuakau? 28, 52A, 64,80,86,90,104 Mill road are in Awaroa ki Tuakau “What number on Mill Road is the Waikato District Council boundary for the Onewhero Tuakau Community Board? 28, 52A, 64,80,86,90,104 Mill road are in Onewhero Tuakau Community Board, the dotted area on the online maps shows the OTCB. From the PDF version of the Community Board map, “What number(s) on King Road is the Waikato District Council boundary” King Road is not a Territorial Authority Boundary, King Road is entirely within the Waikato District. The Orange marker is on King road “What number(s) on King Road is the Waikato District Council boundary for Awaroa ki Tuakau?” All areas to the West and South West of King road are in the Awaroa ki Tuakau Ward. -

Te Kuiti Piopio Kawhia Raglan Regional
Helensville 1 Town/City Road State Highway Expressway Thermal Explorer Highway Cycle Trails Waikato River REGIONAL MAP Hamilton Airport i-SITE Visitor Information Centre Information Centre Thermal Geyser Surf Beach Water Fall Forest Mountain Range AUCKLAND Coromandel Peninsula Clevedon To Whitianga Miranda Thames Pukekohe Whangamata Waiuku POKENO To Thames Maramarua 2 Mangatarata to River TUAKAU Meremere aika W Hampton Downs Hauraki 25 Rail Trail Paeroa PORT WAIKATO Te Kauwhata Waihi 2 Rangiriri 2 Glen 1 Murray Tahuna 26 Kaimai-Mamaku Mount Forest Park Lake Hakanoa Te Aroha Mt Te Aroha Lake Puketirni HUNTLY TE AROHA 27 26 Waiorongomai Valley Taupiri Tatuanui 2 1B Gordonton Te Akau Te Awa NGARUAWAHIA MORRINSVILLE River Ride Ngarua Waingaro TAURANGA 39 Horotiu 2 27 Walton Wairere Falls Raglan HAMILTON Harbour Waharoa 2 Whatawhata Matangi RAGLAN MATAMATA Manu Bay Tamahere 1B 29 23 Te Puke Mt Karioi Raglan Trails CAMBRIDGE 29 Ngahinapouri Ruapuke 27 Beach Ohaupo Piarere 3 Te Awa Lake Te Pahu Bridal Veil Pirongia Forest Park River Ride Karapiro 1 Aotea Falls TIRAU Harbour 5 Mt Pirongia Pirongia Sanctuary TE AWAMUTU Mountain KAWHIA Kihikihi Mt Maungatautari PUTARURU 33 Pukeatua To Rotorua Parawera Arapuni 5 Kawhia 31 Harbour Tihiroa 3 Te Puia Springs 39 1 ROTORUA Hot Water Beach Waikato Optiki River Trails Taharoa OTOROHANGA WAITOMO CAVES Marokopa Falls 3 TOKOROA To Rotorua Waimahora 1 5 Marokopa TE KUITIKUITI 32 30 Mangakino Rangitoto 3 Pureora Forest Park Whakamaru to River Waika PIOPIOPIOPIO 30 4 Pureora Forest Park 32 3 30 To Taumarunui -

210202-Otcb-Agenda.Pdf
1 Agenda for a meeting of the Onewhero-Tuakau Community Board to be held in the Board Room, Tuakau Memorial Hall, George Street, Tuakau on TUESDAY, 2 FEBRUARY 2021 commencing at 6.00pm. Information and recommendations are included in the reports to assist the Board in the decision making process and may not constitute Council’s decision or policy until considered by the Board. 1. APOLOGIES AND LEAVE OF ABSENCE 2. CONFIRMATION OF STATUS OF AGENDA 3. DISCLOSURES OF INTEREST 4. CONFIRMATION OF MINUTES Meeting held on Monday, 23 November 2021 2 5. PUBLIC FORUM 6. REPORTS 6.1 Northern Waikato/Southern Auckland Enhanced Transport Connections Strategic Case 12 6.2 Pokeno and Tuakau Bus Service Photo Competition 28 6.3 Community Led Development Programme 32 6.4 Discretionary Fund Report to 15 January 2021 34 6.5 Year to Date Service Request Report 36 6.6 Projects – Issues - Activities and Actions February 2021 46 6.7 Update for Tuakau Pool Usage to 14 January 2020 51 6.8 Waikato District Council Executive Update Verbal 6.9 Chairperson’s Report Verbal 6.10 Councillors’ and Community Board Members’ Report Verbal GJ Ion CHIEF EXECUTIVE Waikato District Council Onewhero-Tuakau Community Board 1 Agenda: 2 February 2021 2 Open Meeting To Onewhero-Tuakau Community Board From Gavin Ion Chief Executive Date 11 January 2021 Prepared by Lynette Wainwright Committee Secretary Chief Executive Approved Y Reference # GOV0502 Report Title Confirmation of Minutes 1. EXECUTIVE SUMMARY To confirm the minutes of the Onewhero-Tuakau Community Board meeting held on Monday, 23 November 2020. -

Agenda for a Meeting of the Onewhero-Tuakau
1 Agenda for a meeting of the Onewhero-Tuakau Community Board to be held in the Board Room, Tuakau Memorial Hall, George Street, Tuakau on MONDAY 6 NOVEMBER 2017 commencing at 7.30pm. Note: A public forum will be held at 7.00pm prior to the commencement of the meeting. Information and recommendations are included in the reports to assist the Board in the decision making process and may not constitute Council’s decision or policy until considered by the Board. 1. APOLOGIES AND LEAVE OF ABSENCE 2. CONFIRMATION OF STATUS OF AGENDA Sergeant Tod Kirker, NZ Police, will be in attendance from 7.00pm to discuss item 5.1. 3. DISCLOSURES OF INTEREST 4. CONFIRMATION OF MINUTES Meeting held on Monday 2 October 2017 3 5. REPORTS 5.1 NZ Police 8 5.2 Discretionary Fund Report to 24 October 2017 9 5.3 Application for Funding – Lions Club of Tuakau Inc. 11 5.4 Application for Funding – Sunset Beach Lifeguard Service Inc. 29 5.5 Application for Funding – Tuakau and Districts Development Association 53 5.6 Application for Funding – Tuakau Youth Sport Trust 68 5.7 Application for Funding – Te Kohanga School 86 5.8 Year to Date Service Request Report 135 5.9 Change of Public Forum Commencement Time 145 5.10 ANZAC Day 2018 146 5.11 Joint Community Board and Community Committee December Meeting 147 5.12 Works & Issues Report - November 149 Waikato District Council Onewhero-Tuakau Community Board 1 Agenda: 6 November 2017 2 5.13 Wastewater Overflow CIP Education Programme update 158 5.14 Long Term Plan Update Verbal 5.15 Tuakau and Districts Development Association -

PR4878- Biostratigraphy, Sr-Isotope Chronology and Chronostratigraphy-Te Kuiti Group.Pdf
PETROLEUM REPORT SERIES PR4878 Title Biostratigraphy, Sr isotope chronology and chronostratigraphy of the Late Eocene – earliest Miocene Te Kuiti Group, Waikato – King Country Basin, New Zealand Operator Author Peter J.J. Kamp, Anand R.P. Tripathi, Campbell S. Nelson and Austin J.W. Hendy Date 2014 Summary This report reviews and synthesises the biostratigraphy of the Te Kuiti Group based on existing sample data archived in the Fossil Record Electronic Database (FRED). Based on these faunal and floral data, New Zealand biostratigraphic stages for the Late Eocene to Early Miocene are assigned to the formations and members within the group. Analytical strontium (Sr) data and resulting numerical ages are reported here for 26 new macrofossil samples from the Te Kuiti Group, but they do not improve the accuracy of the biostratigraphy and the age information that can be derived from it. The identification of unconformity-bound sequences, the boundaries of which align with the formation contacts within the group, provide an important set of time planes within the group. The integration of the biostratigraphy and sequence stratigraphy produces a robust chronostratigraphy for the Te Kuiti Group. This report has been compiled from material submitted to the New Zealand Government under legislation or voluntarily by exploration companies. An acknowledgement of this work in the following bibliographic format would be appreciated: Kamp, P.J.J., Tripathi A.R.P., Nelson, C.S and Hendy, A.J.W. 2014: Biostratigraphy, Sr isotope chronology and chronostratigraphy of the Late Eocene – earliest Miocene Te Kuiti Group, Wai- kato – King Country Basin, New Zealand. Ministry of Business, Innovation and Employment, New Zealand, unpublished Petroleum Report PR4878, 31 p. -

200629 CCL Open Minutes Confirmed
Minutes of a meeting of the Waikato District Council held in the Council Chambers, District Office, 15 Galileo Street, Ngaruawahia on MONDAY, 29 JUNE 2020 commencing at 9.30am. Present: His Worship the Mayor, Mr AM Sanson (Chairperson) Cr AD Bech Cr JA Church Cr CA Eyre Cr JM Gibb Cr SL Henderson Cr SD Lynch [until 10.21am and then from 10.25am] Cr RC McGuire Cr FM McInally Cr EM Patterson Cr JD Sedgwick Cr NMD Smith Cr LR Thomson Cr CT Woolerton Attending: Mrs D Lovell (Chairperson, Taupiri Community Board) Mr GJ Ion (Chief Executive) Mr TG Whittaker (Chief Operating Officer) Mr R MacCulloch (General Manager Service Delivery Mrs S O’Gorman (General Manager Customer Support) Mr J Quinn (Communications, Engagement and Marketing Manager) Ms L Shirley (Zero Harm Manager) Mr C Bailey (Finance Manager) Mr B Stringer (Democracy Manager) APOLOGIES AND LEAVE OF ABSENCE All members were present Waikato District Council 1 Minutes: 29 June 2020 Document Set ID: 2660539 Version: 1, Version Date: 02/07/2020 CONFIRMATION OF STATUS OF AGENDA ITEMS Resolved: (Crs McInally/Henderson) THAT the agenda for a meeting of the Waikato District Council held on Monday, 29 June 2020 be confirmed and all items therein be considered in open meeting with the exception of those items detailed at agenda item 6 which shall be considered with the public excluded; AND THAT in accordance with Standing Order 9.12 the Committee resolves that the following items be added to the agenda as a matter of urgency as advised by His Worship the Mayor as the item needed to be considered prior to 30 June 2020: Public Excluded Agenda Item 1.1 - Solid Waste and Recycling Contract Renegotiation. -

Agenda for a Meeting of the Onewhero-Tuakau
1 Agenda for a meeting of the Onewhero-Tuakau Community Board to be held in the Board Room, Tuakau Memorial Hall, George Street, Tuakau on MONDAY, 19 JULY 2021 commencing at 6.00pm. Information and recommendations are included in the reports to assist the Board in the decision making process and may not constitute Council’s decision or policy until considered by the Board. 1. APOLOGIES AND LEAVE OF ABSENCE 2. CONFIRMATION OF STATUS OF AGENDA 3. DISCLOSURES OF INTEREST 2 The Register of Interests for the Onewhero-Tuakau Community Board is attached for information purposes and for members to update any interests they may have. 4. CONFIRMATION OF MINUTES Meeting held on Tuesday, 8 June 2021 4 5. PUBLIC FORUM 6. REPORTS 6.1 NZ Police Update 15 6.2 Solid Waste Review 16 6.3 Discretionary Fund Report to 7 July 2021 32 6.4 Placemaking 34 6.5 Projects-Issues-Activities and Actions July 2021 39 6.6 Waikato District Council Executive Update Verbal 6.7 Chairperson’s Report Verbal 6.8 Councillors’ Report Verbal 6.9 Community Board Members’ Report Verbal GJ Ion CHIEF EXECUTIVE Waikato District Council Onewhero-Tuakau Community Board 1 Agenda: 19 July 2021 2 Open Meeting To Onewhero-Tuakau Community Board From Gavin Ion Chief Executive Date 6 July 2021 Prepared by Lynette Wainwright Democracy Advisor Chief Executive Approved Y Reference # GOV0303 Report Title Register of Interests 1. EXECUTIVE SUMMARY A copy of the Register of Interests is attached for the Board’s information. The register will be updated following receipt of information during the year.