The Sumatran Rhinoceros (Dicerorhinus Sumatrensis) Robin W
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Ancients' One-Horned
The Ancients’ One-Horned Ass: Accuracy and Consistency Chris Lavers HIS PAPER explores ancient Greek and Roman accounts of the one-horned ass.1 These narratives have been studied extensively by literary scholars and historians but have Tbeen largely ignored by zoologists and geographers. When the zoological and geographical underpinnings of the accounts are examined, however, it becomes apparent that these ancient writers may have had a more definite notion of the region about which they wrote than hitherto has been assumed. The animals contributing to the descriptions of the one-horned ass by Ctesias, Pliny, and Aelian can be found in the highlands of Central Asia. Indeed, Central Asia appears to be the only place on the Earth’s surface that could have given rise to the corpus of ancient accounts of the unicorned ass and the animals that shared its landscape. 1. Introduction Ctesias of Cnidus was a Greek physician who spent seventeen years ministering at the court of the King of Persia. In 398 B.C. he returned to Greece and began two reference works, a history of Persia in twenty-three volumes, now mostly lost, and Indica, a treatise on the region probably roughly coincident with 1 It will quickly become apparent to regular readers of this journal that the author is not a classicist. I am greatly indebted to Kent Rigsby, the editorial board of GRBS, and an anonymous reviewer for considering a manuscript from a zoologist, and for their kind assistance in turning a clumsy initial submission into the present, less clumsy version. All opinions and errors are mine. -

An Act Prohibiting the Import, Sale and Possession of African Elephants, Lions, Leopards, Black Rhinoceros, White Rhinoceros and Giraffes
Substitute Senate Bill No. 925 Public Act No. 21-52 AN ACT PROHIBITING THE IMPORT, SALE AND POSSESSION OF AFRICAN ELEPHANTS, LIONS, LEOPARDS, BLACK RHINOCEROS, WHITE RHINOCEROS AND GIRAFFES. Be it enacted by the Senate and House of Representatives in General Assembly convened: Section 1. (NEW) (Effective October 1, 2021) (a) For purposes of this section, "big six African species" means any specimen of any of the following members of the animal kingdom: African elephant (loxodonta africana), African lion (panthera leo), African leopard (panthera pardus pardus), black rhinoceros (diceros bicornis), white rhinoceros (ceratotherium simum cottoni) and African giraffe (giraffa camelopardalis), including any part, product or offspring thereof, or the dead body or parts thereof, except fossils, whether or not it is included in a manufactured product or in a food product. (b) No person shall import, possess, sell, offer for sale or transport in this state any big six African species. (c) Any law enforcement officer shall have authority to enforce the provisions of this section and, whenever necessary, to execute any warrant to search for and seize any big six African species imported, possessed, sold, offered for sale or transported in violation of this section. Substitute Senate Bill No. 925 (d) The provisions of subsection (b) of this section shall not apply if the possession of such specimen of a big six African species is expressly authorized by any federal law or permit, or if any of the following conditions exist that are not otherwise prohibited -

Sumatran Rhinoceros
Sumatran rhinoceros Name and species • Common name: Sumatran rhino • Synonyms: Asian two-horned rhino or the Hairy rhino • Scientific name: Dicerorhinus sumatrensis, from the Greek “di”, meaning "two", “cero”, meaning "horn" and “rhinos”, meaning "nose"; “sumatrensis”, from Sumatra Physical characteristics • Sumatran rhinos have a reddish-brown skin, in the wild variably covered with short bristly hair. In captivity the hair can grow out to a shaggy fur, because of less abrasion from vegetation. The ears edges have a prominent fringe of longer hairs, and the tail is terminate with a tuft of thicker hairs. There are two prominent folds in the skin circling the body behind the front legs and before the hind legs, and lesser folds on the neck and at the basis of the legs. The skin is rather thin, about 10-16 mm, and soft and pliable. Subcutaneous fat is absent in wild animals, but may occur in zoo specimens • The Sumatran rhino is considered the most “primitive” rhino species, because of its hairy skin and other ancient characteristics. It is the closest relative alive of the famous woolly rhinoceros that lived in the frigid lands of Europe and Asia during the past ice-ages • Sumatran rhinos are by far the smallest of the five living species of rhino. They weigh between 500-800 kilos, often more in captivity), stand 1.20-1.45 metres tall at the shoulder, and are about 2.50 metres long • The head is 70-80 cm in length and the tails vary in length from 35-60 cm • Sumatran rhinos have two horns, dark grey to black in colour. -
Greater One-Horned Rhinoceros Or Indian Rhino
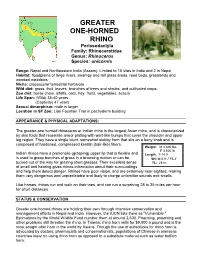
GREATER ONE-HORNED RHINO Perissodactyla Family: Rhinocerotidae Genus: Rhinoceros Species: unicornis Range: Nepal and Northeastern India (Assam). Limited to 10 sites in India and 2 in Nepal Habitat: floodplains of large rivers, swampy and tall grass areas, reed beds, grasslands and wooded meadows Niche: crepuscular terrestrial herbivore Wild diet: grass, fruit, leaves, branches of trees and shrubs, and cultivated crops. Zoo diet: horse chow, alfalfa, oats, hay, fruits, vegetables, acacia Life Span: (Wild) 35-40 years (Captivity) 47 years Sexual dimorphism: male is larger Location in SF Zoo: Lion Fountain Trail in pachyderm building APPEARANCE & PHYSICAL ADAPTATIONS: The greater-one horned rhinoceros or Indian rhino is the largest Asian rhino, and is characterized by skin folds that resemble armor plating with wart-like bumps that cover the shoulder and upper leg region. They have a single blunt, somewhat stubby horn that sits on a bony knob and is composed of hardened, compressed keratin (hair-like) fibers. Weight: M 4,800 lbs. F 3,500 lb Indian rhinos have a prehensile (grasping) upper lip that is flexible and Length: 7-14 ft is used to grasp bunches of grass in a browsing motion or can be SH: M 5.9' / F5.2' tucked out of the way for grazing short grasses. Their excellent sense TL: 28 in. of smell and hearing gives rhinos information about their surroundings and help them detect danger. Rhinos have poor vision, and are extremely near-sighted, making them very dangerous and unpredictable and likely to charge unfamiliar sounds and smells. Like horses, rhinos run and walk on their toes, and can run a surprising 28 to 35 miles per hour for short distances. -

La Brea and Beyond: the Paleontology of Asphalt-Preserved Biotas
La Brea and Beyond: The Paleontology of Asphalt-Preserved Biotas Edited by John M. Harris Natural History Museum of Los Angeles County Science Series 42 September 15, 2015 Cover Illustration: Pit 91 in 1915 An asphaltic bone mass in Pit 91 was discovered and exposed by the Los Angeles County Museum of History, Science and Art in the summer of 1915. The Los Angeles County Museum of Natural History resumed excavation at this site in 1969. Retrieval of the “microfossils” from the asphaltic matrix has yielded a wealth of insect, mollusk, and plant remains, more than doubling the number of species recovered by earlier excavations. Today, the current excavation site is 900 square feet in extent, yielding fossils that range in age from about 15,000 to about 42,000 radiocarbon years. Natural History Museum of Los Angeles County Archives, RLB 347. LA BREA AND BEYOND: THE PALEONTOLOGY OF ASPHALT-PRESERVED BIOTAS Edited By John M. Harris NO. 42 SCIENCE SERIES NATURAL HISTORY MUSEUM OF LOS ANGELES COUNTY SCIENTIFIC PUBLICATIONS COMMITTEE Luis M. Chiappe, Vice President for Research and Collections John M. Harris, Committee Chairman Joel W. Martin Gregory Pauly Christine Thacker Xiaoming Wang K. Victoria Brown, Managing Editor Go Online to www.nhm.org/scholarlypublications for open access to volumes of Science Series and Contributions in Science. Natural History Museum of Los Angeles County Los Angeles, California 90007 ISSN 1-891276-27-1 Published on September 15, 2015 Printed at Allen Press, Inc., Lawrence, Kansas PREFACE Rancho La Brea was a Mexican land grant Basin during the Late Pleistocene—sagebrush located to the west of El Pueblo de Nuestra scrub dotted with groves of oak and juniper with Sen˜ora la Reina de los A´ ngeles del Rı´ode riparian woodland along the major stream courses Porciu´ncula, now better known as downtown and with chaparral vegetation on the surrounding Los Angeles. -

Fencing Affects African Wild Dog Movement Patterns and Population Dynamics
Fencing affects African wild dog movement patterns and population dynamics H ELEN M. K. O’ N EILL,SARAH M. DURANT S TEFANIE S TREBEL and R OSIE W OODROFFE Abstract Wildlife fences are often considered an important Introduction tool in conservation. Fences are used in attempts to pre- vent human–wildlife conflict and reduce poaching, despite abitat fragmentation is a leading threat to global bio- known negative impacts on landscape connectivity and ani- Hdiversity (Millennium Ecosystem Assessment, ). mal movement patterns. Such impacts are likely to be par- As habitats become increasingly fragmented, wildlife pop- ticularly important for wide-ranging species, such as the ulations also become fragmented in smaller, genetically African wild dog Lycaon pictus, which requires large areas isolated, subpopulations that will be at greater risk of of continuous habitat to fulfil its resource requirements. extinction (Lande, ). This is of particular concern for Laikipia County in northern Kenya is an important area wide-ranging species that are reliant on accessing large for wild dogs but new wildlife fences are increasingly areas to fulfil their resource requirements, meaning that being built in this ecosystem. Using a long-term dataset fragmentation can lead to such species being extirpated, from the area’s free-ranging wild dog population, we evalu- even when habitat may remain (Løvschal et al., ). Frag- ated the effect of wildlife fence structure on the ability of mentation often increases the cost incurred by wildlife wild dogs to cross them. The extent to which fences im- in obtaining vital resources and may even cut access off en- peded wild dog movement differed between fence designs, tirely (Epps et al., ; Løvschal et al., ). -

Detomidine and Butorphanol for Standing Sedation in a Range of Zoo-Kept Ungulate Species
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Ghent University Academic Bibliography Journal of Zoo and Wildlife Medicine 48(3): 616–626, 2017 Copyright 2017 by American Association of Zoo Veterinarians DETOMIDINE AND BUTORPHANOL FOR STANDING SEDATION IN A RANGE OF ZOO-KEPT UNGULATE SPECIES Tim Bouts, D.V.M., M.Sc., Dip. E.C.Z.M., Joanne Dodds, V.N., Karla Berry, V.N., Abdi Arif, M.V.Sc., Polly Taylor, Vet. M. B., Ph. D., Dip. E.C.V.A.A., Andrew Routh, B. V. Sc., Cert. Zoo. Med., and Frank Gasthuys, D.V.M., Ph. D., Dip. E.C.V.A.A. Abstract: General anesthesia poses risks for larger zoo species, like cardiorespiratory depression, myopathy, and hyperthermia. In ruminants, ruminal bloat and regurgitation of rumen contents with potential aspiration pneumonia are added risks. Thus, the use of sedation to perform minor procedures is justified in zoo animals. A combination of detomidine and butorphanol has been routinely used in domestic animals. This drug combination, administered by remote intramuscular injection, can also be applied for standing sedation in a range of zoo animals, allowing a number of minor procedures. The combination was successfully administered in five species of nondomesticated equids (Przewalski horse [Equus ferus przewalskii; n ¼ 1], onager [Equus hemionus onager; n ¼ 4], kiang [Equus kiang; n ¼ 3], Grevy’s zebra [Equus grevyi; n ¼ 4], and Somali wild ass [Equus africanus somaliensis; n ¼ 7]), with a mean dose range of 0.10–0.17 mg/kg detomidine and 0.07–0.13 mg/kg butorphanol; the white (Ceratotherium simum simum; n ¼ 12) and greater one-horned rhinoceros (Rhinoceros unicornis; n ¼ 4), with a mean dose of 0.015 mg/kg of both detomidine and butorphanol; and Asiatic elephant bulls (Elephas maximus; n ¼ 2), with a mean dose of 0.018 mg/kg of both detomidine and butorphanol. -

Tapir Tracks Dear Educator
TAPIR TRACKS A Curriculum Guide for Educators 2 Tapir Tracks Dear Educator, Welcome to Tapir Tracks! This curriculum was created for classroom teachers and educators at zoos and other nonformal science learning centers to enable you and your students to discover tapirs of the Americas and Asia. Because tapirs spread seeds from the fruits they eat, these little-known mammals are essential to the health of the forests they inhabit. However, tapir populations are rapidly declining. Loss of their habitat and hunting threaten tapir survival. An international team of scientists and conservationists works to study wild tapirs, manage the zoo-based population, protect habitat, and educate local communities. We collaborate through the Tapir Specialist Group, of the International Union for Conservation of Nature (IUCN) Species Survival Commission. This packet includes background information along with lesson plans and activities that can easily be adapted for kindergarten, elementary and secondary school students (grades K-12). An online link is included for you to download images and videos to use in your teaching: http://tapirs.org/resources/educator-resources. This toolkit is designed to enable you to meet curriculum requirements in multiple subjects. Students can explore the world’s tapirs through science, environmental studies, technology, social studies, geography, the arts and creative writing activities. We hope that by discovering tapirs through these lessons and engaging activities that students will care and take action to protect tapirs -

The Interspecific Relationships of Black Rhinoceros (Diceros Bicornis) in Hluhluwe-Imfolozi Park
The interspecific relationships of black rhinoceros (Diceros bicornis) in Hluhluwe-iMfolozi Park Roan David Plotz B.Sc. (ConsBiolEcol) (Hons1); GradDipEd (Sec) A thesis submitted to Victoria University of Wellington in fulfilment of the requirement for the degree of Doctor of Philosophy in Ecology and Biodiversity 2014 1 “To Ryker, may the wild places of this world long remain protected to captivate and inspire you” Black rhino near the Black iMfolozi River in Hluhluwe-iMfolozi Park, Zululand, South Africa (Photograph by Dale Morris). “We learn more by looking for the answer to a question and not finding it than we do from learning the answer itself.” Lloyd Alexander 2 ABSTRACT As habitat loss, predators (human and non-human) and disease epidemics threaten species worldwide, protected sanctuaries have become vital to species conservation. Hluhluwe-iMfolozi Park (HiP) in South Africa is at the centre of one of the world’s greatest conservation success stories. The formal proclamation of HiP in 1895 prevented the extinction of the south-central black rhino (Diceros bicornis minor) population. In recent times HiP has been a strategic source population for the D. b. minor range expansion program, facilitating an 18-fold population increase across southern Africa. However, HiP’s own black rhino population appears to be in decline. Evidence for decline is most often attributed to overpopulation and poor habitat quality that is driving apparently significant increases in the average home range sizes, poor growth rates (i.e., low calf recruitment) and poor body condition of black rhino. Other factors such as non-human calf predation and parasitism have also been raised as potential causes of decline but remain untested. -
Deciduous Forest
Biomes and Species List: Deciduous Forest, Desert and Grassland DECIDUOUS FOREST Aardvark DECIDUOUS FOREST African civet DECIDUOUS FOREST American bison DECIDUOUS FOREST American black bear DECIDUOUS FOREST American least shrew DECIDUOUS FOREST American pika DECIDUOUS FOREST American water shrew DECIDUOUS FOREST Ashy chinchilla rat DECIDUOUS FOREST Asian elephant DECIDUOUS FOREST Aye-aye DECIDUOUS FOREST Bobcat DECIDUOUS FOREST Bornean orangutan DECIDUOUS FOREST Bridled nail-tailed wallaby DECIDUOUS FOREST Brush-tailed phascogale DECIDUOUS FOREST Brush-tailed rock wallaby DECIDUOUS FOREST Capybara DECIDUOUS FOREST Central American agouti DECIDUOUS FOREST Chimpanzee DECIDUOUS FOREST Collared peccary DECIDUOUS FOREST Common bentwing bat DECIDUOUS FOREST Common brush-tailed possum DECIDUOUS FOREST Common genet DECIDUOUS FOREST Common ringtail DECIDUOUS FOREST Common tenrec DECIDUOUS FOREST Common wombat DECIDUOUS FOREST Cotton-top tamarin DECIDUOUS FOREST Coypu DECIDUOUS FOREST Crowned lemur DECIDUOUS FOREST Degu DECIDUOUS FOREST Working Together to Live Together Activity—Biomes and Species List 1 Desert cottontail DECIDUOUS FOREST Eastern chipmunk DECIDUOUS FOREST Eastern gray kangaroo DECIDUOUS FOREST Eastern mole DECIDUOUS FOREST Eastern pygmy possum DECIDUOUS FOREST Edible dormouse DECIDUOUS FOREST Ermine DECIDUOUS FOREST Eurasian wild pig DECIDUOUS FOREST European badger DECIDUOUS FOREST Forest elephant DECIDUOUS FOREST Forest hog DECIDUOUS FOREST Funnel-eared bat DECIDUOUS FOREST Gambian rat DECIDUOUS FOREST Geoffroy's spider monkey -

Bill Analysis for File Copy
OLR Bill Analysis sSB 925 AN ACT PROHIBITING THE IMPORT, SALE AND POSSESSION OF AFRICAN ELEPHANTS, LIONS, LEOPARDS, BLACK RHINOCEROS, WHITE RHINOCEROS AND GIRAFFES. SUMMARY This bill generally bans importing, possessing, selling, offering for sale, or transporting in Connecticut a specimen (dead or alive) of any of six types of African animals, which the bill collectively refers to as the “big six African species.” It applies to certain elephants, lions, leopards, giraffes, and two rhinoceros species. The bill establishes a graduated penalty structure for violations, ranging from no penalty for someone who, unaware and in good faith, violates the ban, to a class D felony for someone with at least two prior violations subject to penalty. In all cases, the bill requires seizing the specimen and any other property or item used in connection with the violation. The specimen, property, or item is then forfeited and, unless the specimen is alive, destroyed. The bill contains several exemptions, including for a specimen that is already legally in the state or distributed to a beneficiary or heir, as long as the owner or distributee timely obtains a certificate of possession from the Department of Energy and Environmental Protection (DEEP). The ban also does not apply to fossils and ivory and the following under certain conditions: circuses; museums; zoological institutions; and motion picture, television, or digital media production companies. Lastly, the bill specifies that the ban does not prohibit transporting through the state endangered or threatened species subject to the terms of another state’s permit, which existing law allows. The United States regulates the trade of the species covered by the Researcher: KLM Page 1 5/8/21 2021SB-00925-R010637-BA.DOCX bill, except the African giraffe, through the Convention on International Trade in Endangered Species of Wild Fauna and Flora (CITES) and laws such as the Endangered Species Act (16 U.S.C. -

Natsca News Issue 22-1.Pdf
http://www.natsca.org NatSCA News Title: The Horns of Dilemma: The Impact of Illicit Trade in Rhino Horn Author(s): Paolo Viscardi Source: Viscardi, P. (2012). The Horns of Dilemma: The Impact of Illicit Trade in Rhino Horn. NatSCA News, Issue 22, 8 ‐ 13. URL: http://www.natsca.org/article/107 NatSCA supports open access publication as part of its mission is to promote and support natural science collections. NatSCA uses the Creative Commons Attribution License (CCAL) http://creativecommons.org/licenses/by/2.5/ for all works we publish. Under CCAL authors retain ownership of the copyright for their article, but authors allow anyone to download, reuse, reprint, modify, distribute, and/or copy articles in NatSCA publications, so long as the original authors and source are cited. NatSCA News Issue 22 The Horns of a Dilemma: The Impact of the Illicit Trade in Rhino Horn Paolo Viscardi Deputy Keeper, Horniman Museum and Gardens Email: [email protected] Abstract Rhinoceros horn has recently become highly sought after on the black market for use in Traditional Asian Medicine. Demand has increased levels of poaching and has led to the theft of material from collections across Europe through 2011. This article provides background to the situation and reiterates guidance on protecting both rhinoceros horn and staff in natural science collections. Keywords Rhinoceros, rhino, horn, poaching, security, theft, auction, legislation, threat, CITES, DEFRA, AHVLA Introduction It has been a bad year for rhinoceros and for natural history collections holding their horn. The international black market dealing in rhino horn has been particularly active recently, following a rumour that Traditional Asian Medicine (TAM) containing powdered horn could successfully treat and prevent cancer.