January 2007
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
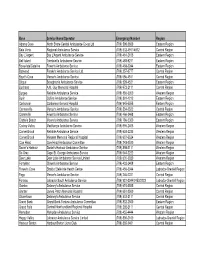
Revised Emergency Contact #S for Road Ambulance Operators
Base Service Name/Operator Emergency Number Region Adams Cove North Shore Central Ambulance Co-op Ltd (709) 598-2600 Eastern Region Baie Verte Regional Ambulance Service (709) 532-4911/4912 Central Region Bay L'Argent Bay L'Argent Ambulance Service (709) 461-2105 Eastern Region Bell Island Tremblett's Ambulance Service (709) 488-9211 Eastern Region Bonavista/Catalina Fewer's Ambulance Service (709) 468-2244 Eastern Region Botwood Freake's Ambulance Service Ltd. (709) 257-3777 Central Region Boyd's Cove Mercer's Ambulance Service (709) 656-4511 Central Region Brigus Broughton's Ambulance Service (709) 528-4521 Eastern Region Buchans A.M. Guy Memorial Hospital (709) 672-2111 Central Region Burgeo Reliable Ambulance Service (709) 886-3350 Western Region Burin Collins Ambulance Service (709) 891-1212 Eastern Region Carbonear Carbonear General Hospital (709) 945-5555 Eastern Region Carmanville Mercer's Ambulance Service (709) 534-2522 Central Region Clarenville Fewer's Ambulance Service (709) 466-3468 Eastern Region Clarke's Beach Moore's Ambulance Service (709) 786-5300 Eastern Region Codroy Valley MacKenzie Ambulance Service (709) 695-2405 Western Region Corner Brook Reliable Ambulance Service (709) 634-2235 Western Region Corner Brook Western Memorial Regional Hospital (709) 637-5524 Western Region Cow Head Cow Head Ambulance Committee (709) 243-2520 Western Region Daniel's Harbour Daniel's Harbour Ambulance Service (709) 898-2111 Western Region De Grau Cape St. George Ambulance Service (709) 644-2222 Western Region Deer Lake Deer Lake Ambulance -

Executive Notes, May 8, 2015 from the NLTA
Newfoundland and Labrador Teachers’ Association EXECUTIVE NOTES May 8, 2015 our NLTA Provincial Executive met in St. John’s rebuild and recover from the earthquake devastation. Yon May 8, 2015. Executive Notes is a summary of • The NLTA will provide $500 to the NL Federation of discussions and decisions that occurred at these meetings. School Councils to assist with their AGM. For further information contact any member of Provincial • The NLTA will sponsor St. John’s Pride to the level of Executive or the NLTA staff person as indicated. $1,000 (silver sponsorship) pending a review of the promotional material for St. John’s Pride 2015. President’s Report Since the February meeting of Provincial Executive the For further information contact James Dinn, President President has attended numerous functions and visited or Don Ash, Executive Director. schools in St. John’s, Paradise, Conne River, Milltown, Ad Hoc Committee on Substitute Teachers English Harbour West, Harbour Breton, Lewisporte, • The NLTA will lobby the districts and the Department of Campbellton and Norris Arm. He presented NLTA’s pre- Education and Early Childhood Development to increase budget consultation brief to the Minister of Finance, met substitute teachers’ access to professional development with NLESD Trustees, met with the Minister of Finance sessions. regarding pension discussions, and with the Minister of • The NLTA will consider offering professional Education and Early Childhood Development regarding development sessions specifically for substitutes, as teacher allocation cuts. He attended the 2015 International well as consider the most viable way to offer these Summit on the Teaching Profession, the substitute teacher sessions to as many substitute teachers as possible. -

Social, Economic and Cultural Overview of Western Newfoundland and Southern Labrador
Social, Economic and Cultural Overview of Western Newfoundland and Southern Labrador ii Oceans, Habitat and Species at Risk Publication Series, Newfoundland and Labrador Region No. 0008 March 2009 Revised April 2010 Social, Economic and Cultural Overview of Western Newfoundland and Southern Labrador Prepared by 1 Intervale Associates Inc. Prepared for Oceans Division, Oceans, Habitat and Species at Risk Branch Fisheries and Oceans Canada Newfoundland and Labrador Region2 Published by Fisheries and Oceans Canada, Newfoundland and Labrador Region P.O. Box 5667 St. John’s, NL A1C 5X1 1 P.O. Box 172, Doyles, NL, A0N 1J0 2 1 Regent Square, Corner Brook, NL, A2H 7K6 i ©Her Majesty the Queen in Right of Canada, 2011 Cat. No. Fs22-6/8-2011E-PDF ISSN1919-2193 ISBN 978-1-100-18435-7 DFO/2011-1740 Correct citation for this publication: Fisheries and Oceans Canada. 2011. Social, Economic and Cultural Overview of Western Newfoundland and Southern Labrador. OHSAR Pub. Ser. Rep. NL Region, No.0008: xx + 173p. ii iii Acknowledgements Many people assisted with the development of this report by providing information, unpublished data, working documents, and publications covering the range of subjects addressed in this report. We thank the staff members of federal and provincial government departments, municipalities, Regional Economic Development Corporations, Rural Secretariat, nongovernmental organizations, band offices, professional associations, steering committees, businesses, and volunteer groups who helped in this way. We thank Conrad Mullins, Coordinator for Oceans and Coastal Management at Fisheries and Oceans Canada in Corner Brook, who coordinated this project, developed the format, reviewed all sections, and ensured content relevancy for meeting GOSLIM objectives. -

Appendix D: Nunatsiavut Regional Impact Assessment
Nunatsiavut Regional Impact Document ITK National Position Document on Canada-Wide Strategy for Management of Municipal Wastewater Effluent Draft January 29, 2008 Sikumiut Sikumiut Environmental Avatilgijingita Management Ltd. Kamajingit 1.0 Introduction and Overview Sikumiut Environmental Management Ltd. (Sikumiut) was retained by ITK to coordinate a review by the Nunatsiavut communities of the proposed Regulatory Framework for Wastewater Treatment. In compiling this response, information was collected through contact with the five Labrador Inuit communities which comprise Nunatsiavut, the portion of Labrador which was the subject of a recently settled Land Claims Agreement. Other sources of information included the Community Accounts website as well as the Municipal Plans for each community. The communities comprising Nunatsiavut (Figure 1) are all located on the North Coast of Labrador adjacent to salt water. There are no road connections. Each community is accessible by air, with twin otter aircraft providing regular service from Happy Valley- Goose Bay to gravel airstrips adjacent to each community. During open water season (July - October) a marine coastal service provides less expensive transport of passengers and goods. Snowmobile trails connect Rigolet, Makkovik and Postville with Upper Lake Melville and the town of Happy Valley-Goose Bay. The total population of the North Coast is approximately 2 500, ranging between approximately 200 (Rigolet and Postville) and 1,000 (Nain). The communities are dominantly (90 – 95%) Inuit. The economies of the communities are based on renewable resources generally (fishing, hunting, wood harvesting) however mining and quarrying have become important contributors in recent years. Tourism is at a modest level, but is expected to grow, especially for Nain with respect to the Torngat Mountains National Park Reserve. -

Board Minutes December 7, 2019
OFFICE OF THE DIRECTOR Chair: Goronwy Price C.E.O./Director of Education: Anthony Stack Newfoundland and Labrador English School Board Minutes December 7, 2019 1. OPENING The Newfoundland and Labrador English School Board (NLESB) meeting took place on Saturday, December 7, 2019 at the District Conference Centre at 40 Strawberry Marsh Road, St. John’s, NL. The meeting was called to order by the Chair of the Board, Goronwy Price, at 3:02 PM. Members present: Mr. Goronwy Price, Chair Mr. Hayward Blake, Vice-Chair Mr. Wayne Lee Mr. Winston Carter Mr. Lester Simmons Ms. Pamela Gill Mr. Thomas Kendell Mr. Keith Culleton Mr. Scott Burden Mr. Kevin Ryan Mr. Eric Ayers (Skype) Mr. John George Mr. Raymond Bennett Mr. Steve Tessier Regrets: Ms. Jennifer Aspell Mr. Peter Whittle Also in attendance: Mr. Anthony Stack, CEO/Director of Education Mr. Ed Walsh, Associate Director of Education (Programs and Human Resources) Mr. Terry Hall, CFO/Assistant Director of Education (Corporate Services) Ms. Georgina Lake, Assistant Director of Education (Student Services) Ms. Heather May, Director of Strategic Planning, Policy and Communications Ms. Susan Tobin, Manager of Policy Mr. Doug Pippy, Director of Educational Programs Mr. Andrew Hickey, Assistant Director of Education, (Programs) Central Region Mr. John Way, NLESD Mr. Ian Wallace, Parliamentarian Ms. Elaine Cross, Executive Assistant 2. ADOPTION OF AGENDA MOTION: It was moved by Thomas Kendell and seconded by Raymond Bennett that the agenda be adopted as presented. (Carried) 3. MINUTES OF PREVIOUS MEETING 3.1 October 26, 2019 Minutes adopted (Wayne Lee/John George) Carried 3.2 October 26, 2019 AGM Minutes adopted (Steve Tessier/Winston Carter) Carried 3.3 November 7, 2019 Minutes adopted (Pamela Gill/John George) Carried 4. -
Labrador Inuit Constitution
THE LABRADOR INUIT CONSTITUTION 1 TABLE OF CONTENTS CHAPTER 1 .................................................................................................................................................. 7 FOUNDING PROVISIONS ...................................................................................................................... 7 Part 1.1 The Labrador Inuit Constitution ........................................................................................... 7 Part 1.2 Amendment of the Labrador Inuit Constitution and Effective Date .................................... 10 Part 1.3 Nunatsiavut, the Nunatsiavut Government and the Institutions of Labrador Inuit Self- Government ....................................................................................................................... 13 Part 1.4 Labrador Inuit Rights of Participation in the Nunatsiavut Government .............................. 13 Part 1.5 Capital of Nunatsiavut ....................................................................................................... 14 Part 1.6 Languages ......................................................................................................................... 15 Part 1.7 Nunatsiavut Flag ............................................................................................................... 16 Part 1.8 Nunatsiavut Anthem .......................................................................................................... 16 CHAPTER 2 ............................................................................................................................................... -

Lgbtq Resources
Equity and Inclusive Education Resource Kit for Newfoundland and Labrador, Grades 7 -12 LGBTQ RESOURCES LGBTQ NewfouNdLaNd aNd LaBrador For a continually updated web directory of regional and national resources, see MyGSA.ca/Resources LGBTQ and LGBTQ-Friendly Organizations, Programmes, & Resources in Newfoundland and Labrador Provincial Resources: Making Queerness Visible Workshop 6 Camp Eclipse 7 Supportive Counseling and Peer Support (Planned Parenthood Newfoundland & Labrador Sexual Health Centre) 8 Wapanaki Two-Spirit Alliance, Atlantic Region 9 Piecing Together a Caring Community: A Resource Book on Dismantling Homophobia by Ann Shortall - selected sections available in PDF format at www.MyGSA.ca 10 Violence Prevention Labrador 10 Northern Committee Against Violence 10 Western Regional Coalition to End Violence 10 Southwestern Coalition to End Violence 11 Central West Committee Against Violence Inc. 11 The Roads to End Violence 11 Eastern Region Committee Against Violence 11 Burin Peninsula Voice Against Violence 12 Communities Against Violence 12 Coalition Against Violence 12 Resources in St. John’s: Aids Committee of Newfoundland and Labrador (ACNL) 13 Frontrunners (Running Group) 13 LBGT MUN (Memorial University) 14 LGBT Youth Group (Planned Parenthood & Newfoundland and Labrador Sexual Health Centre) 14 PFLAG Canada (St. John’s Chapter) 15 Spectrum (Queer Choir) 15 Resources in Corner Brook: Corner Brook Pride 16 Resources in Grand Falls-Windsor: LGBTQ Group in Central NL, Grand Falls-Windsor 16 Resources in Labrador: Safe Alliance, -

Student and Youth Services Agreement.Xlsx
2015-16 Student and Youth Services Agreement Approvals Organization Location Project Approved Amount BOTWOOD BOYS AND GIRLS CLUB Botwood Youth Cordinator$ 40,100 CBDC TRINITY CONCEPTION CORPORATION Carbonear Community Youth Coordinator$ 87,500 COLLEGE OF THE NORTH ATLANTIC St. John's Small Enterprise Co-Operative Placement Assistance$ 229,714 COLLEGE OF THE NORTH ATLANTIC St. John's Student Works and Service Program (SWASP)$ 90,155 COLLEGE OF THE NORTH ATLANTIC St. John's Partnership in Academic Career Education Employment Program $ 57,232 (PACEE) COMMUNITY YOUTH NETWORK CORNER BROOK & AREA Corner Brook Impact $ 5,071 CONSERVATION CORPS NEWFOUNDLAND AND St. John's Green Team$ 579,600 LABRADOR FOR THE LOVE OF LEARNING, INC St. John's Watering the Seeds$ 115,000 HARBOUR BRETON COMMUNITY YOUTH Harbour Breton Youth Entreprensurial Skills$ 35,000 HARBOUR BRETON COMMUNITY YOUTH Harbour Breton Youth Outreach Coordinator$ 52,500 HARBOUR GRACE COMMUNITY YOUTH Harbour Grace Changing Lanes$ 60,301 KANGIDLUASUK STUDENT PROGRAM INC Nain Student Program$ 7,000 MARINE INSTITUTE St. John's Youth Opportinities Coop Program$ 100,000 MARINE INSTITUTE St. John's Wage Subsidies for MESD$ 11,186 MEMORIAL UNIVERSITY OF NL St. John's Small Enterprise Co-Operative Placement Assistance$ 522,993 MEMORIAL UNIVERSITY OF NL St. John's Graduate Transition to Employment (GTEP)$ 200,000 MEMORIAL UNIVERSITY OF NL St. John's Student Works and Service Program (SWASP)$ 331,680 MEMORIAL UNIVERSITY OF NL St. John's Partnership in Academic Career Education Employment Program $ 67,732 (PACEE) NEWFOUNDLAND AND LABRADOR ASSOC OF Mount Pearl Youth Ventures$ 82,000 COMMUNITY BUSINESS DEVELOPMENT CORPORATIONS SKILLS CANADA-NEWFOUNDLAND AND LABRADOR St. -

Office Allowances - Office Accommodations 01-Apr-20 to 30-Sep-20
House of Assembly Newfoundland and Labrador Member Accountability and Disclosure Report Office Allowances - Office Accommodations 01-Apr-20 to 30-Sep-20 LOVELESS, ELVIS, MHA Page: 1 of 1 Summary of Transactions Processed to Date for Fiscal 2020/21 Expenditure Limit (Net of HST): $7,800.00 Transactions Processed as of: 30-Sep-20 Expenditures Processed to Date (Net of HST): $5,850.00 Funds Available (Net of HST): $1,950.00 Percent of Funds Expended to Date: 75.0% Date Source Document # Vendor Name Expenditure Details Amount 01-Apr-20 HOA006183 ROY DRAKE Lease payment for the Constituency Office for the District of Fortune Bay - Cape 975.00 La Hune located in Harbour Breton. 01-May-20 HOA006216 ROY DRAKE Lease payment for the Constituency Office for the District of Fortune Bay - Cape 975.00 La Hune located in Harbour Breton. 01-Jun-20 HOA006252 ROY DRAKE Lease payment for the Constituency Office for the District of Fortune Bay - Cape 975.00 La Hune located in Harbour Breton. 01-Jul-20 HOA006295 ROY DRAKE Lease payment for the Constituency Office for the District of Fortune Bay - Cape 975.00 La Hune located in Harbour Breton. 01-Aug-20 HOA006334 ROY DRAKE Lease payment for the Constituency Office for the District of Fortune Bay - Cape 975.00 La Hune located in Harbour Breton. 01-Sep-20 HOA006370 ROY DRAKE Lease payment for the Constituency Office for the District of Fortune Bay - Cape 975.00 La Hune located in Harbour Breton. Period Activity: 5,850.00 Opening Balance: 0.00 Ending Balance: 5,850.00 ---- End of Report ---- House of Assembly -

17 Tuesday, April 16Th, 2013 the House Met at 1:30 O'clock in The
17 Tuesday, April 16th, 2013 The House met at 1:30 o’clock in the afternoon pursuant to adjournment. The Honourable the Government House Leader (Mr. King) raised a point of privilege concerning the alleged use of social media by a Member of the House of Assembly. The Speaker (Mr. Wiseman) suspended the proceedings at 1:46 o’clock in the afternoon to consider the point of privilege. The Speaker resumed the Chair at 4:23 o’clock in the afternoon and ruled that there was no point of privilege but that there had been a contempt. The Speaker requested three times that the Member for St. John’s Centre (Ms. Rogers) apologize. The Member declined. The Speaker named the Member for St. John’s Centre (Ms. Rogers) and requested that the Sergeant-at-Arms escort Ms. Rogers from the Chamber. The Member for Lewisporte (Mr. Verge) made a Statement to recognize the volunteer firefighters in his District. The Member for Humber Valley (Mr. Ball) made a Statement to commend Mr. Clarence White who has received the Newfoundland and Labrador Teachers’ Association Special Recognition Award. The Member for St. Barbe (Mr. Bennett) made a Statement to pay tribute to the late Howard Joseph Lavers. The Member for Kilbride (Mr. Dinn) made a Statement to recognize the St. Kevin’s Junior High School Girls’ Cross Country Running Team, winners of the regional championships in Placentia in October. The Member for Terra Nova (Mr. Collins) made a Statement to recognize Mr. David Saunders, advocate for the arts and the preservation of the Province’s heritage. -

Relocation Redux: Labrador Inuit Population Movements and Inequalities in the Land Claims Era
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Sociology Department, Faculty Publications Sociology, Department of 12-2016 Relocation Redux: Labrador Inuit Population Movements and Inequalities in the Land Claims Era Kirk Dombrowski University of Nebraska - Lincoln, [email protected] Patrick Habecker University of Nebraska-Lincoln, [email protected] G. Robin Gauthier University of Nebraska-Lincoln, [email protected] Bilal Khan University of Nebraska - Lincoln, [email protected] Joshua Moses Haverford College, [email protected] Follow this and additional works at: https://digitalcommons.unl.edu/sociologyfacpub Part of the Family, Life Course, and Society Commons, Indigenous Studies Commons, Social and Cultural Anthropology Commons, and the Social Psychology and Interaction Commons Dombrowski, Kirk; Habecker, Patrick; Gauthier, G. Robin; Khan, Bilal; and Moses, Joshua, "Relocation Redux: Labrador Inuit Population Movements and Inequalities in the Land Claims Era" (2016). Sociology Department, Faculty Publications. 715. https://digitalcommons.unl.edu/sociologyfacpub/715 This Article is brought to you for free and open access by the Sociology, Department of at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in Sociology Department, Faculty Publications by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. Current Anthropology Volume 57, Number 6, December 2016 785 Relocation Redux Labrador Inuit Population Movements and Inequalities in the -
Labrador Mining and Power: How Much and Where From?
Labrador mining and power: how much and where from? Department of Natural Resources November 2012 Key Factors • $10-15 billion of investment in Labrador mining projects may be realized over the next decade but this is dependent in part on the availability and cost of power. • If these projects proceed they will bring major economic benefits to the province, through employment and taxation revenue (both direct and indirect), as well as provide opportunities for service industries. • Estimation of future power needs for planned mining developments is challenging, particularly as many projects have not advanced to the stage where firm requests for power have been made. • Based on projects already in construction or near sanction, existing generating capacity in Labrador may be exhausted by 2015-17. • Muskrat Falls could be an important source of power for mining developments post-2017, and sanctioning of the project may assist mining companies in making positive investment decisions. Availability of power will encourage investment in the province rather than in competing jurisdictions. • Muskrat Falls could provide power for future mining developments (or export markets if mining developments are slow to proceed) as well as providing sufficient power for the Island of Newfoundland. The Isolated Island option, with refurbishment or replacement of the Holyrood Generating Station or any other isolated alternative, will not supply the power needed for Labrador mining developments. • In the longer term, mining developments may absorb all residual power from the Muskrat Falls development. Further power may be needed. LABRADOR MINING AND POWER: HOW MUCH AND WHERE FROM? 1 Introduction The provincial minerals sector in 2012 is forecast to operate at record levels, with mineral shipments and mineral industry employment at all-time highs.