Septic Arthritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Is It Orthopaedic Or Neurologic? Sorting out Lameness, Paresis and Dogs That Won’T Get Up
IS IT ORTHOPAEDIC OR NEUROLOGIC? SORTING OUT LAMENESS, PARESIS AND DOGS THAT WON’T GET UP Christopher L. Mariani, DVM, PhD, DACVIM (Neurology) Associate Professor of Neurology & Neurosurgery College of Veterinary Medicine North Carolina State University Lameness, difficulty walking, and reluctance or inability to rise are common presentations for patients presented to small animal practitioners. Disorders of the central and peripheral nervous systems, spine, long bones, joints, tendons, or musculature can all result in these clinical signs. Identifying the organ system and anatomic structures responsible are critical to recommending subsequent diagnostic testing, therapy, and possibly referral to the appropriate specialist. The most critical steps in this evaluation are careful observation of the animal’s gait, and thorough neurologic and orthopedic examinations. CLINICAL EVALUATION Gait Examination Gait examination is arguably the most important part of the evaluation of patients with difficulty ambulating, but is often not performed by veterinary practitioners. The patient should be evaluated while walking towards and away from the examiner, and should also be observed from the side. If the animal is unable to stand or bear weight, adequate support of the limbs in question should be provided while assessing the ability of the animal to voluntarily advance its limbs, bear weight, and move in a coordinated manner. Several abnormalities may be detected with the gait examination. These include: Ataxia: incoordination characterized by a failure to walk or move the limbs in a straight line, crossing of the limbs over the body midline, and possibly stumbling and falling. Ataxia indicates neurologic dysfunction, and may be caused by involvement of several areas of the nervous system. -

Introduction
Whether you enjoy horses as they roam INTRODUCTION around the yard, depend on them for getting From the Ground Up your work done, or engage in competitive Grab hold of most any equine publication and you enthusiasts have wri�en and spoken about proper sports, keeping up with the latest in health can witness the excitement building around research horse and hoof care, much of their advice has been of the equine hoof. We have marveled at its simplistic dismissed until more recently. Discussions of sound advancements will help you enjoy them for design and intricate functions for decades, yet this hoof management practices are once again coming more productive years. latest, fresh information renews our respect and to the forefront in the equine sports industry because enthusiasm for keeping those hooves healthy. Such lameness issues are so common and devastating to so facts surrounding hoof health and disease give us many top performance horses in the world. Careful an accurate perspective on what it takes to raise and study, observation and research is allowing us to have maintain healthy horses; the hooves are a window to horses that run faster, travel farther, jump higher, the horse’s state of health. We are steadily improving ride safer and live longer. Sharing this valuable in our horsemanship and making decisions which information with you is an honor and a privilege and keep our valuable partners from harm, allowing is part of an ongoing dedication to help horses stay or us to enjoy them for more years than we thought become healthier. -

A Review of Selected Neurological Diseases Affecting Horses
MILNE LECTURE Neurology Is Not a Euphemism for Necropsy: A Review of Selected Neurological Diseases Affecting Horses Stephen M. Reed, DVM, Diplomate ACVIM Author’s address: Rood and Riddle Equine Hospital, PO Box 12070, Lexington, KY 40580; e-mail: [email protected]. © 2008 AAEP. 1. Introduction An increased level of understanding about the Disorders of the nervous system are serious and causes and management of equine neurological dis- often debilitating problems affecting horses. Refer- eases during the past 30 yr has resulted in consid- ence to equine neurological diseases can be found as erably less fear on the part of owners and early as 1860 when Dr. E. Mayhew described a con- veterinarians when faced with the statement that dition of partial paralysis in The Illustrated Horse “your horse is ataxic.” This increased awareness Doctor. Dr. Mayhew wrote that “with few excep- and knowledge about causes of ataxia in horses has tions a permanent neurologic gait deficit renders a made it routine for most equine veterinarians to in- horse unsuitable for use.” Although this is still at clude some level of neurological testing as part of their least partially correct today, there would be little physical examination. One need not look too hard to need to go further with today’s lecture if not for the identify articles on the role of the neurological exami- fact that much progress has been made in our un- nation as a part of the purchase, lameness, and even derstanding of how to better diagnose and treat exercise evaluation in horses. There are even articles neurological disorders affecting horses. -

EQUINE LAMENESS Dr Annemarie Farrington a Lame Horse Is Defined
EQUINE LAMENESS Dr Annemarie Farrington A lame horse is defined as having an abnormal gait or an incapability of normal locomotion. The commonest causes of lameness in horses include infection (e.g., subsolar abscess), trauma, congenital conditions (e.g., contracted tendons), and acquired abnormalities (e.g., osteochondritis dissecans). Factors unrelated to the musculoskeletal system such as metabolic, circulatory, and nervous system abnormalities (e.g., wobbler syndrome) can also cause a horse to become lame. Lameness resulting from musculoskeletal abnormalities is the leading cause of poor performance in athletic horses and thus the ability to diagnose and treat lameness is an important technique in veterinary medicine. The timely and accurate evaluation of lameness requires a detailed knowledge of the horse’s anatomy, biomechanics, conformation, breed characteristics and an ability to assess a variety of gaits – ie walk, trot, canter.. More lameness is seen in the forelimbs than the hindlimbs and almost 95% of forelimb lameness occurs from the knee down. When the hind limb is involved, however, many more problems are seen in the upper part of the limb, especially in the hock or stifle.. However accurate lameness diagnosis may not always be as straightforward as it seems so a methodical approach must be employed. It is always important to start a lameness examination with a complete history of the lameness, a general physical examination of the horse to rule out other, potentially more serious diseases, and a thorough conformation assessment. The horse’s gait or movement must then be evaluated initially while walking but then trotting both in a straight line and in a circle. -

Recent Advances in Equine Osteoarthritis Annette M Mccoy, DVM, MS, Phd, DACVS; University of Illinois College of Veterinary Medicine
Recent Advances in Equine Osteoarthritis Annette M McCoy, DVM, MS, PhD, DACVS; University of Illinois College of Veterinary Medicine Introduction It is widely recognized that osteoarthritis (OA) is the most common cause of chronic lameness in horses and that it places a significant burden on the equine industry due to the cost of treatment and loss of use of affected animals. Depending on the disease definition and target population, the reported prevalence of OA varies. It was reported at 13.9% in a cross-sectional survey of horses in the UK, but at 97% (defined by loss of range of motion) in a group of horses over 30 years of age. Among Thoroughbred racehorses that died within 60 days of racing, 33% had at least one full-thickness cartilage lesion in the metacarpophalangeal joint, and the severity of cartilage lesions strongly correlated with a musculoskeletal injury leading to death. The majority of the horses in this study were less than 3 years of age, emphasizing the importance of OA in young equine athletes. Unfortunately, a major challenge in managing OA is that by the time clinical signs occur (i.e. lameness), irreversible cartilage damage has already occurred. Although novel treatment modalities are being tested that show promise for modulation of the course of disease, such as viral vector delivery of genes that produce anti-inflammatory products, there are no generally accepted treatments that can be used to reliably reverse its effects once a clinical diagnosis has been made. Thus, there is much research effort being put both into the development of improved diagnostic markers and the development of new treatments for this devastating disease. -

CELLULITIS by Drs Georgina Johnston and Allison Stewart
CELLULITIS by Drs Georgina Johnston and Allison Stewart Dr Georgina Johnston BVetMed BSc (Hons1) MRCVS Georgina is an experienced equine vet and is currently completing speciality training in Equine Sports Medicine and Rehabilitation at the University of Queensland Equine Specialist Hospital. Her clinical interests include lameness investigation, diagnostic imaging, cardiology and exercise testing. Georgina is also an FEI vet. What is cellulitis? Cellulitis can be a frustrating and challenging condition to treat. It is caused by a bacterial infection of the soft tissues under the skin. In horses, it is most commonly found in one of the hind legs but can occur anywhere in the body. Cellulitis is typically first noticed as sudden swelling that is hot and painful to the touch. As the infection worsens, the horse may develop a fever or become lame to the point of not wanting to bear weight on the affected leg. Swelling can spread from the initial site of infection to affect the entire leg. The infection spreads throughout the tissue causing massive swelling. The lymphatics (fine vessels that return tissue fluid or “lymph” back to the circulatory system) are overwhelmed or compressed by the swollen tissue and this results in additional swelling from oedema (non-infected tissue fluid). Cellulitis is very painful, while oedema is non-painful and can be diagnosed by making an impression of a finger in the swollen tissue without any pain response from the horse. It can however be difficult to distinguish exactly which parts of the swollen limb are due to the primary cellulitis and which parts are due to the secondary oedema. -

Pottoka´S Behaviour and Training
POTTOKA´S BEHAVIOUR AND TRAINING The horse’s long evolution as a prey animal has selected a series of behaviours, including social behaviour, that are surprisingly uniform despite great differences in race, climate and geographical conditions. Ethology is the study of animal behaviour under natural conditions, that is, wild, not domestic, animals. Until very recently it was thought that the only true wild horse was Przewalski’s, the Asiatic wild horse (Equus przewalskii). Unfortunately most examples live in zoos, although a herd has been re-introduced to natural conditions in Mongolia where its behaviour is being studied. Wild Equus caballus, the modern horse, was thought to be extinct. Almost all “wild” horses are in fact feral, that is, descendents of escaped domestic horses. During domestication, certain characteristics useful to man are selected: docility, ease of training, strength or speed, the capacity to accept often rather rough handling without protest, the acceptance of unnatural living conditions, or any other whim that takes our fancy, like shape of head or coat colour. It should be noted that ease of training does not necessarily mean intelligence, for our training methods are often confused and anthropomorphic. North American mustangs and island ponies, South American criollos living wild, Australian and New Zealand brumbies, Namibian desert horses, Japanese misaki horses and others, including the famous Tour du Valat herd of Camargue ponies, are all feral horses whose behaviour has been studied. Recently, however, it has been found that the Portuguese Sorraia, which now lives in domestic conditions, is in fact a true wild horse dating from the Palaeolithic. -

Lameness in Horses Prompt Recognition and Treatment of Lameness Is Imperative to Minimize Losses
Fact Sheet Sponsored by: Lameness in Horses Prompt recognition and treatment of lameness is imperative to minimize losses Overview flexion tests (bending individual joints for Lameness, traditionally defined as any an extented amout of time and then watch- abnormal gait, is a common event in the ing the horse trot off) to determine which equine industry, contributing to untold areas are painful, and if a decreased range economic and horse losses annually.1,2 To- of motion exists. day, veterinarians also accept that even be- In the United States veterinarians typi- havior changes, not just gait changes, can cally classify the degree of lameness by cause lameness in horses due to pain in the grade using the American Association of neck, withers, shoulders, back, loin, hips, Equine Practitioner’s (AAEP) lameness legs, or feet.2 grading system:2 Grade 0 is defined as no detectable lame- Causes of Lameness ness under any circumstances. A number of conditions can result in Grade 1 is defined as lameness that is diffi- lameness. These include trauma, congeni- cult to observe and is inconsistently appar- tal conditions (e.g., contracted tendons), ent regardless of the circumstances (e.g., acquired abnormalities (e.g., osteochon- in hand or under saddle, hard surface, in- dritis dissecans), and infection (e.g., septic/ cline, or circling). infectious arthritis). Essentially, any body Grade 2 lameness is difficult to detect at a ON part that has nerve endings can serve as a S walk or trot in a straight line, but is consis- source of pain, and horses with poor confor- A LAR tently apparent under particular circum- IC mation are more likely to suffer problems ER stances (e.g., under saddle, hard surface, with tendons, ligaments, and joints than During a lameness examination, a veterinarian incline). -

Navicular Syndrome in Equine Patients: Anatomy, Causes, and Diagnosis*
3 CE CREDITS CE Article In collaboration with the American College of Veterinary Surgeons Navicular Syndrome in Equine Patients: Anatomy, Causes, and Diagnosis* R. Wayne Waguespack, DVM, MS, DACVS R. Reid Hanson, DVM, DACVS, DACVECC Auburn University Abstract: Navicular syndrome is a chronic and often progressive disease affecting the navicular bone and bursa, deep digital flexor tendon (DDFT), and associated soft tissue structures composing the navicular apparatus. This syndrome has long been considered one of the most common causes of forelimb lameness in horses. Diagnosis of navicular syndrome is based on history, physical examina- tion, lameness examination, and peripheral and/or intraarticular diagnostic anesthesia. Several imaging techniques (e.g., radiography, ultrasonography, nuclear scintigraphy, thermography, computed tomography [CT], magnetic resonance imaging [MRI]) are used to identify pathologic alterations associated with navicular syndrome. Radiographic changes of the navicular bone are not pathognomonic for navicular syndrome. Additionally, not all horses with clinical signs of navicular syndrome have radiographic changes associated with the navicular bone. Therefore, newer imaging modalities, including CT and especially MRI, can play an important role in identifying lesions that were not observed on radiographs. Navicular bursoscopy may be necessary if the clinical findings suggest that lameness originates from the navicular region of the foot and if other imaging modalities are nondiagnostic. With new diagnostic imaging tech- niques, clinicians are learning that anatomic structures other than the navicular bursa, navicular bone, and DDFT may play an important role in navicular syndrome. avicular syndrome is chronic and often progressive, Anatomy of the Equine Digit affecting the navicular bone and bursa as well as the The navicular bone is boat shaped and lies at the palmar associated deep digital flexor tendon (DDFT) and aspect of the distal interphalangeal joint (DIPJ; FIGURE 1). -

Horse Breeds - Volume 3
Horse Breeds - Volume 3 A Wikipedia Compilation by Michael A. Linton Contents Articles Latvian horse 1 Lipizzan 3 Lithuanian Heavy Draught 11 Lokai 12 Losino horse 13 Lusitano 14 Malopolski 19 Mallorquín 21 Mangalarga 23 Mangalarga Marchador 24 Maremmano 28 Marismeño 30 Marwari horse 31 Mecklenburger 35 Međimurje horse 39 Menorquín horse 41 Mérens horse 43 Messara horse 51 Miniature horse 52 Misaki horse 57 Missouri Fox Trotter 59 Monchino 62 Mongolian horse 63 Monterufolino 65 Morab 66 Morgan horse 70 Moyle horse 76 Murakoz horse 77 Murgese 78 Mustang horse 80 Namib Desert Horse 86 Nangchen horse 91 National Show Horse 92 Nez Perce Horse 94 Nivernais horse 96 Nokota horse 97 Nonius horse 101 Nordlandshest/Lyngshest 104 Noriker horse 106 Norman Cob 109 Coldblood trotter 114 North Swedish Horse 116 Novokirghiz 118 Oberlander horse 119 Oldenburg horse 120 Orlov Trotter 125 Ostfriesen and Alt-Oldenburger 129 Pampa horse 134 Paso Fino 135 Pentro horse 140 Percheron 141 Persano horse 148 Peruvian Paso 149 Pintabian 154 Pleven horse 156 Poitevin horse 157 Posavac horse 164 Pryor Mountain Mustang 166 Przewalski's horse 175 Purosangue Orientale 183 Qatgani 185 Quarab 186 Racking horse 188 Retuerta horse 189 Rhenish-German Cold-Blood 190 Rhinelander horse 191 Riwoche horse 192 Rocky Mountain Horse 195 Romanian Sporthorse 197 Russian Don 199 Russian Heavy Draft 201 Russian Trotter 203 References Article Sources and Contributors 204 Image Sources, Licenses and Contributors 208 Article Licenses License 212 Latvian horse 1 Latvian horse Latvian Alternative names Latvian Harness Horse Latvian Carriage Latvian Coach Latvian Draft Latvian Riding Horse Country of origin Latvia Horse (Equus ferus caballus) The Latvian horse comes from Latvia and is split into three types: the common harness horse, a lighter riding horse and a heavier draft type. -
An Approach to Diagnosing Lameness in Equine Patients
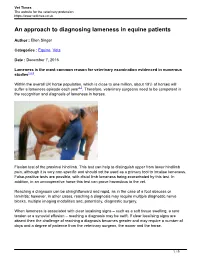
Vet Times The website for the veterinary profession https://www.vettimes.co.uk An approach to diagnosing lameness in equine patients Author : Ellen Singer Categories : Equine, Vets Date : December 7, 2015 Lameness is the most common reason for veterinary examination evidenced in numerous studies1,2,3. Within the overall UK horse population, which is close to one million, about 19% of horses will suffer a lameness episode each year4,5. Therefore, veterinary surgeons need to be competent in the recognition and diagnosis of lameness in horses. Flexion test of the proximal hindlimb. This test can help to distinguish upper from lower hindlimb pain, although it is very non-specific and should not be used as a primary tool to localise lameness. False-positive tests are possible, with distal limb lameness being exacerbated by this test. In addition, in an uncooperative horse this test can prove hazardous to the vet. Reaching a diagnosis can be straightforward and rapid, as in the case of a foot abscess or laminitis; however, in other cases, reaching a diagnosis may require multiple diagnostic nerve blocks, multiple imaging modalities and, potentially, diagnostic surgery. When lameness is associated with clear localising signs – such as a soft tissue swelling, a sore tendon or a synovial effusion – reaching a diagnosis may be swift. If clear localising signs are absent then the challenge of reaching a diagnosis becomes greater and may require a number of days and a degree of patience from the veterinary surgeon, the owner and the horse. 1 / 9 The overall challenge in lameness evaluation is to reach one specific diagnosis so clear advice can be provided to the owner regarding treatment and prognosis. -

MAGNETIC RESONANCE IMAGING the More Motion Artefact Is Agnetic Resonance How MRI Works by Sarah E Powell When Is an MRI Scan Name: Sarah E
ROSSDALES EQUINE HOSPITAL & DIAGNOSTIC CENTRE Cotton End Road, Exning, Newmarket, Suffolk CB8 7NN Vet Vetwatch www.rossdales.com Profile MAGNETIC RESONANCE IMAGING the more motion artefact is agnetic resonance How MRI works By Sarah E Powell When is an MRI scan Name: Sarah E. Powell imaging (MRI) When the area (i.e. tissue) we are appropriate? present on the images, preventing Qualifications: MA VetMB describes the interested in is placed into a strong MRI scans are reserved for cases detection of certain injuries. MRCVS M Not all horses make suitable Year of Qualification: 2002 method of imaging the horse magnetic field and a short pulse of where lameness has been localised of the foot in detail, both of which Main interests: My main area is by stimulating the molecules in radio waves is applied, the tissues to a specific region by nerve and patients for standing MRI equine orthopaedic disease with are frequently implicated in foot the tissue to ‘resonate’ when a ‘resonate’ and a weak ‘signal’ joint blocks and a definitive procedures. Some horses will not an emphasis on diagnostic lameness. This is particularly true imaging. I have a special interest magnetic field is applied to echoes back from the tissue. The diagnosis has not been possible tolerate the procedure well, or are of what is commonly called too small to be comfortably in computed tomographic and them. echo varies depending on the type using other imaging techniques. magnetic resonance imaging and ‘Navicular Syndrome’ (NS). A The most common application is of tissue present in the anatomic In almost all cases an X-ray and/or positioned within the magnet.