Endometrial Sampling Devices for Early Diagnosis of Endometrial Lesions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Water Resource Carrying Capacity Based on Water Demand Prediction in Chang-Ji Economic Circle
water Article Water Resource Carrying Capacity Based on Water Demand Prediction in Chang-Ji Economic Circle Ge Wang 1,2,3,4, Changlai Xiao 1,2,3,4, Zhiwei Qi 1,2,3,4, Xiujuan Liang 1,2,3,4,*, Fanao Meng 1,2,3,4 and Ying Sun 1,2,3,4 1 Key Laboratory of Groundwater Resources and Environment, Jilin University, Ministry of Education, No 2519, Jiefang Road, Changchun 130021, China; [email protected] (G.W.); [email protected] (C.X.); [email protected] (Z.Q.); [email protected] (F.M.); [email protected] (Y.S.) 2 Jilin Provincial Key Laboratory of Water Resources and Environment, Jilin University, Changchun 130021, China 3 National-Local Joint Engineering Laboratory of In-Situ Conversion, Drilling and Exploitation Technology for Oil Shale, Changchun 130021, China 4 College of New Energy and Environment, Jilin University, No 2519, Jiefang Road, Changchun 130021, China * Correspondence: [email protected] Abstract: In view of the large spatial difference in water resources, the water shortage and deteriora- tion of water quality in the Chang-Ji Economic Circle located in northeast China, the water resource carrying capacity (WRCC) from the perspective of time and space is evaluated. We combine the gray correlation analysis and multiple linear regression models to quantitatively predict water supply and demand in different planning years, which provide the basis for quantitative analysis of the WRCC. The selection of research indicators also considers the interaction of social economy, water resources, and water environment. Combined with the fuzzy comprehensive evaluation method, the gray corre- lation analysis and multiple linear regression models to quantitatively and qualitatively evaluate the WRCC under different social development plans. -

2.15 Jilin Province Jilin Province Jixin Group Co. Ltd., Affiliated to the Jilin Provincial Prison Administration Bureau, Has 22
2.15 Jilin Province Jilin Province Jixin Group Co. Ltd., affiliated to the Jilin Provincial Prison Administration Bureau, has 22 prison enterprises Legal representative of the prison company: Feng Gang, Chairman of Jilin Jixin Group Co., Ltd. His official positions in the prison system: Party Committee Member of Jilin Provincial Justice Department, Party Committee Secretary and Director of Jilin Provincial Prison Administration Bureau1 According to the “Notice on Issuing ‘Jilin Province People’s Government Institutional Reform Program’ from the General Office of the CCP Central Committee and the General Office of the State Council” (Ting Zi [2008] No. 25), the Jilin Provincial Prison Administration Bureau (Deputy-department level) was set up as a management agency under the Provincial Justice Department.2 Business areas: The company manages state-owned operating assets of the enterprises within province’s prison system; production, processing and sale of electromechanical equipment (excluding cars), chemical products, apparels, cement, construction materials; production and sale of agricultural and sideline products; labor processing No. Company Name of the Legal Person Legal Registered Business Scope Company Notes on the Prison Name Prison, to which and representative Capital Address the Company Shareholder(s) / Title Belongs 1 Jilin Jixin Jilin Provincial State-owned Feng Gang 70.67 The company manages state-owned 1000 Xinfa According to the “Notice on Issuing Group Co., Prison Asset Chairman of Jilin million operating assets of the -

The Standardization of Procedures in Village Committee Elections
The Standardization of Villager Committee Election Procedures Survey Analysis of the 5th Round of Villager Committee Elections in 40 Villages from Five Counties in Jilin Province Sun Long and Tong Zhihui I. Survey Background, Purpose, and Methodology Chinese villager committee elections have entered a phase of legalization and standardization, as indicated by the formal promulgation of the Organic Law on Villager Committees in 1998. Jilin Province is the birthplace of the haixuan method of villager committee elections. Haixuan, or “sea election,” means that candidates are not predetermined by higher- level government offices or leaders but nominated by villagers having the right to vote. Final candidates are then determined according to the number of nominations each individual receives. (Wang Zhoutian, 1995) As early as 1986, a portion of Lishu County, Jilin Province began using the haixuan method. By the 4th round of village committee elections in 1997, 86.8% of all villages in Jilin Province had moved to the haixuan method. (Jilin Province People’s Congress Internal Affairs and Justice Committee, et al., 2001) In November 2000, the Standing Committee of the People’s Congress in Jilin Province ratified the Jilin Province Measures for the Election of Villager Committees , standardizing many procedures in villager committee elections. Under the guidance of these Measures, the 5th round of villager committee elections in Jilin Province were held between November 2000 and March 2001. To determine how well the election procedures had been implemented in the villager committee elections, in July 2001 the Ministry of Civil Affairs (MCA) Department of Basic- Level Governance and Community Construction conducted a survey of 790 cadres and villagers in 40 villages randomly selected from five counties in Jilin Province. -

Characteristics of Spatial Connection Based on Intercity Passenger Traffic Flow in Harbin- Changchun Urban Agglomeration, China Research Paper
Guo, R.; Wu, T.; Wu, X.C. Characteristics of Spatial Connection Based on Intercity Passenger Traffic Flow in Harbin- Changchun Urban Agglomeration, China Research Paper Characteristics of Spatial Connection Based on Intercity Passenger Traffic Flow in Harbin-Changchun Urban Agglomeration, China Rong Guo, School of Architecture,Harbin Institute of Technology,Key Laboratory of Cold Region Urban and Rural Human Settlement Environment Science and Technology,Ministry of Industry and Information Technology,Harbin 150006,China Tong Wu, School of Architecture,Harbin Institute of Technology,Key Laboratory of Cold Region Urban and Rural Human Settlement Environment Science and Technology,Ministry of Industry and Information Technology,Harbin 150006,China Xiaochen Wu, School of Architecture,Harbin Institute of Technology,Key Laboratory of Cold Region Urban and Rural Human Settlement Environment Science and Technology,Ministry of Industry and Information Technology,Harbin 150006,China Abstract With the continuous improvement of transportation facilities and information networks, the obstruction of distance in geographic space has gradually weakened, and the hotspots of urban geography research have gradually changed from the previous city hierarchy to the characteristics of urban connections and networks. As the main carrier and manifestation of elements, mobility such as people and material, traffic flow is of great significance for understanding the characteristics of spatial connection. In this paper, Harbin-Changchun agglomeration proposed by China's New Urbanization Plan (2014-2020) is taken as a research object. With the data of intercity passenger traffic flow including highway and railway passenger trips between 73 county-level spatial units in the research area, a traffic flow model is constructed to measure the intensity of spatial connection. -

Species Composition and Dynamics of Aphids and Parasitoid Wasps in Maize Fields in Northeastern China
bioRxiv preprint doi: https://doi.org/10.1101/2020.10.19.345215; this version posted October 19, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Species composition and dynamics of aphids and parasitoid wasps in maize fields in Northeastern China Ying Zhang1, Min-chi Zhao1, Jia Cheng1, Shuo Liu1, Hai-bin Yuan1 * 1 Jilin Agricultural University, Department of Plant Protection, Changchun,130118, China. *Corresponding author; [email protected] Abstract Maize, Zea mays L., is the most abundant field crop in China. Aphids are the most economically damaging pest on maize, particularly in the cotton agri-ecosystems of Jilin Province, northern China. Parasitic wasps are important natural enemies of aphids, but limited information exists about their species composition, richness and seasonal dynamics in northern China. In this study, the population dynamics of maize aphids and parasitoid wasps were assessed in relation to each other during the summer seasons of two consecutive years, 2018 and 2019. We selected maize fields in the Changchun, Songyuan, Huinan and Gongzhuling areas of Jilin Province. Four species of aphids were recorded from these maize fields: Rhopalosiphum padi (L), Rhopalosiphum maidis (Fitch), Aphis gossypii Glover and Macrosiphum miscanthi (Takahashi). The dominant species in each of the four areas were R. maids (Filch) and R. padi in Changchun, R .padi in Songyuan, A. gossypii and R. padi in Huinan, and A.gossypii and R. -
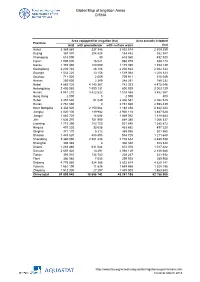
Global Map of Irrigation Areas CHINA
Global Map of Irrigation Areas CHINA Area equipped for irrigation (ha) Area actually irrigated Province total with groundwater with surface water (ha) Anhui 3 369 860 337 346 3 032 514 2 309 259 Beijing 367 870 204 428 163 442 352 387 Chongqing 618 090 30 618 060 432 520 Fujian 1 005 000 16 021 988 979 938 174 Gansu 1 355 480 180 090 1 175 390 1 153 139 Guangdong 2 230 740 28 106 2 202 634 2 042 344 Guangxi 1 532 220 13 156 1 519 064 1 208 323 Guizhou 711 920 2 009 709 911 515 049 Hainan 250 600 2 349 248 251 189 232 Hebei 4 885 720 4 143 367 742 353 4 475 046 Heilongjiang 2 400 060 1 599 131 800 929 2 003 129 Henan 4 941 210 3 422 622 1 518 588 3 862 567 Hong Kong 2 000 0 2 000 800 Hubei 2 457 630 51 049 2 406 581 2 082 525 Hunan 2 761 660 0 2 761 660 2 598 439 Inner Mongolia 3 332 520 2 150 064 1 182 456 2 842 223 Jiangsu 4 020 100 119 982 3 900 118 3 487 628 Jiangxi 1 883 720 14 688 1 869 032 1 818 684 Jilin 1 636 370 751 990 884 380 1 066 337 Liaoning 1 715 390 783 750 931 640 1 385 872 Ningxia 497 220 33 538 463 682 497 220 Qinghai 371 170 5 212 365 958 301 560 Shaanxi 1 443 620 488 895 954 725 1 211 648 Shandong 5 360 090 2 581 448 2 778 642 4 485 538 Shanghai 308 340 0 308 340 308 340 Shanxi 1 283 460 611 084 672 376 1 017 422 Sichuan 2 607 420 13 291 2 594 129 2 140 680 Tianjin 393 010 134 743 258 267 321 932 Tibet 306 980 7 055 299 925 289 908 Xinjiang 4 776 980 924 366 3 852 614 4 629 141 Yunnan 1 561 190 11 635 1 549 555 1 328 186 Zhejiang 1 512 300 27 297 1 485 003 1 463 653 China total 61 899 940 18 658 742 43 241 198 52 -
External Monitoring Report of Resettlement for ADB Financed
Social Monitoring Report Project Number: 40665 October 2011 PRC: Songhua River Basin Water Pollution Control and Management Project (Jilin Component) Prepared by the Project Management Office of Jilin Provincial Government with the assistance of Northeast Project Management Co. Ltd. For: Jilin Provincial Government Dehui City Tianyi Water Co. Ltd.; Gongzhuling City Urban State-Owned Assets Operations Co. Ltd. Fusong County Lantianbishui Infrastructure Development Co. Ltd.; Fuyu County Wastewater Treatment Co. Ltd.; Jingyu County Yutong Municipal Engineering Co. Ltd.; Liuhe County Bishui Wastewater Treatment Co. Ltd.; Tonghua County Water Supply Co.; Yushu Tianyi Water Co. Ltd.; Da’an City Xingcheng Urban Infrastructure Development and Construction Co. Ltd. Huadian City Infrastructure Development Construction Investment Co. Ltd.; Huinan County Chaoyang Township Huashu Domestic SolidWaste Treatment Service Co. Ltd.; Jiaohe City Jiemei Solid Waste Co.; Jingyu County Huanyu Domestic Solid Waste Management Co. Ltd,; Liuhe County Luyuan Domestic Solid Waste Management and Service Co. Ltd.; Meihekou City Jiecheng Domestic Solid Waste Collection, Transportation and Treatment Co. Ltd.; Tongyu County Hecheng Domestic Solid Waste Sanitary Landfill; Changbaishan Development and Construction Group Co. Ltd. This report has been submitted to ADB by the Project Management Office of Hefei Municipal Government and is made publicly available in accordance with ADB’s public communications policy (2005). It does not necessarily reflect the views of ADB. ADB -

Spatial-Temporal Change of Land Use and Its Impact on Water Quality of East-Liao River Basin from 2000 to 2020
water Article Spatial-Temporal Change of Land Use and Its Impact on Water Quality of East-Liao River Basin from 2000 to 2020 Mingxi Zhang 1,2,3, Guangzhi Rong 1,2,3, Aru Han 1,2,3, Dao Riao 1,2,3, Xingpeng Liu 1,2,3,*, Jiquan Zhang 1,2,3 and Zhijun Tong 1,2,3 1 School of Environment, Northeast Normal University, Changchun 130024, China; [email protected] (M.Z.); [email protected] (G.R.); [email protected] (A.H.); [email protected] (D.R.); [email protected] (J.Z.); [email protected] (Z.T.) 2 Department of Environment, Institute of Natural Disaster Research Northeast Normal University, Changchun 130024, China 3 Key Laboratory for Vegetation Ecology, Ministry of Education, Changchun 130024, China * Correspondence: [email protected]; Tel.: +86-139-4406-7540 Abstract: Land use change is an important driving force factor affecting the river water environment and directly affecting water quality. To analyze the impact of land use change on water quality change, this study first analyzed the land use change index of the study area. Then, the study area was divided into three subzones based on surface runoff. The relationship between the characteristics of land use change and the water quality grade was obtained by grey correlation analysis. The results showed that the land use types changed significantly in the study area since 2000, and water body and forest land were the two land types with the most significant changes. The transfer rate is cultivated field > forest land > construction land > grassland > unused land > water body. -

Minimum Wage Standards in China August 11, 2020
Minimum Wage Standards in China August 11, 2020 Contents Heilongjiang ................................................................................................................................................. 3 Jilin ............................................................................................................................................................... 3 Liaoning ........................................................................................................................................................ 4 Inner Mongolia Autonomous Region ........................................................................................................... 7 Beijing......................................................................................................................................................... 10 Hebei ........................................................................................................................................................... 11 Henan .......................................................................................................................................................... 13 Shandong .................................................................................................................................................... 14 Shanxi ......................................................................................................................................................... 16 Shaanxi ...................................................................................................................................................... -

Jilin Province, China, January 2021
China CDC Weekly Outbreak Reports COVID-19 Super Spreading Event Amongst Elderly Individuals — Jilin Province, China, January 2021 Laishun Yao1,&; Mingyu Luo2,&; Tiewu Jia3,&; Xingang Zhang1; Zhulin Hou1; Feng Gao1; Xin Wang1; Xiaogang Wu1; Weihua Cheng4; Guoqian Li4; Jing Lu4; Bing Zhao3; Tao Li3; Enfu Chen2; Dapeng Yin3,#; Biao Huang1,# locked down to help stop virus transmission starting Summary from January 20. What is already known on this topic? Clusters of COVID-19 cases often happened in small INVESTIGATION AND RESULTS settings (e.g., families, offices, school, or workplaces) that facilitate person-to-person virus transmission, Through January 31, 2021, there have been about especially from a common exposure. 140 cases associated with the same case (called Mr. L in What is added by this report? this report), showing Mr. L to be a super spreader. On January 10 and 11, 2021, an individual gave three Mr. L, a 44-year-old male, is a product promotion product promotional lectures in Tonghua City, Jilin lecturer who travels often. From December 23, 2020 Province, that ultimately led to a 74-case cluster of to January 3, 2021, Mr. L traveled by train and plane COVID-19. Our investigation determined the in Shandong, Shanxi, Henan, and Heilongjiang outbreak to be an import-related COVID-19 provinces; from January 3 to 6, Mr. L traveled by train superspreading cluster event in which elderly, retired inside Heilongjiang Province; and on January 7, he people were exposed to the infected individual during traveled through Jilin Province by train to Changchun his promotional lectures, which were delivered in a City. -

State-Run Industrial Enterprises in Fengtian, 1920-1931
State Building, Capitalism, and Development: State-Run Industrial Enterprises in Fengtian, 1920-1931 A DISSERTATION SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY OF MINNESOTA BY Yu Jiang IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY Liping Wang, Ann Waltner October 2010 © Yu Jiang, 2010 Acknowledgements I am grateful that Department of History at University of Minnesota took a risk with me, somebody with no background in history. I also thank the department for providing a one-semester fellowship for my dissertation research. I am deeply indebted to Minnesota Population Center for hosting me in its IT team for many years – it allowed me, a former software engineer, to keep abreast of the latest developments in computer technology while indulging in historical studies. Thanks are especially due to Steve Ruggles (MPC director) and Pete Clark (IT director) for giving me this great opportunity. The source materials for this dissertation mostly come from Liaoning Provincial Archives, Liaoning Provincial Library, and Meihekou Archives. I thank these institutions for their help. Liaoning Shekeyuan offered both warm reception and administrative help right after I arrived in Shenyang. My archival research in Shenyang also benefited greatly from Chris Isett’s help. Su Chen from East Asian Library at University of Minnesota has been helpful numerous times in locating important documents. My committee members, Mark Anderson, Ted Farmer, M.J. Maynes, Ann Waltner, and Liping Wang provided valuable comments on the draft. M.J. and Ann’s thoughtful comments on a paper based on my dissertation helped improve my work. -

Democartic People's Republic of Korea Atlas
PGDS in DOS Democratic People's Rep. of Korea Atlas Map Population and Geographic Data Section As of July 2005 Division of Operational Support Email : [email protected] ! !!!!!!!! ) )))))))) )))))))) ! ! Nongan ! !!!!!!!! Shulan ))) Pogranichnyy ))))))))))))))))) ! !!!!!!!! Ningan r ! !!!!!!!! Jiutai o w ! !!!!!!!! . ! ! Dongjingcheng C P 3 A _ m e D _ p e ! !!!!!!!! R ! ! Changchung _ ! !!!!!!!! Jilin a ! ! e r ! !!!!!!!! o ! ! Jiaohe K ! !!!!!!!! Datun ! !!!!!!!! Xinan ! !!!!!!!! ! !!!!!!!! Gongzhuling ! !!!!!!!! Dunhua ! !!!!!!!! Yitong ! !!!!!!!! Yantongshan ! !!!!!!!! Bamiancheng ! !!!!!!!! ! !!!!!!!! ! ! Huadian ! !!!!!!!! Tumen) )))))))))))))))) ! !!!!!!!! Panshi ))) ! !!!!!!!! Liaoyuan ! !!!!!!!! Yanji ! !!!!!!!! Hunchun ! !!!!!!!! ! !!!!!!!! ! ! Chongsong ! ! Laochengzhen ! !!!!!!!! ))))))))))))))))) I Dong ) )))))))) )))))))) CHINACHINACHINACHINACHINACHINACHINACHINACHINACHINACHINACHINACHINACHINA ! !!!!!!!! Kaishantun ))) Kraskino ! !!!!!!!! Dongfeng ! !!!!!!!! ))))))))))))))))) Hailong ! !!!!!!!! Laocheng ))))))))))))))))) Sechon-dong ! !!!!!!!! Helong ! !!!!!!!! Kaiyuan ! !!!!!!!! Meihekou ! !!!!!!!! Kyongchung ) )))))))) )))))))) ! !!!!!!!! ))) Yuson! ! ! !!!!!!!! Qingyu ! !!!!!!!! Shanchengzhen ! !!!!!!!! Unggi ! !!!!!!!! Lihue ))))))))))))))))) Najin ))))))))))))))))) Musan ))))))))))))))))) Komusan Dong ))))))))))))))))) ! !!!!!!!! Hunjiang !! Fushun ) )))))))) )))))))) Lingjiang ))) ! !!!!!!!! ! ! ) )))))))))))))))) ! !!!!!!!! Tong Hua ))) Nanam RUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIAN