India's Bhilwara COVID-19 Containment Policy Response
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Basic Details School Name Kendriya Vidyalaya Kota Road Bhilwara Rajasthan School Code 03549 Address Kendriya Vidyalaya,Kota Road
BASIC DETAILS 03549--KENDRIYA VIDYALAYA KOTA ROAD BHILWARA RAJASTHAN Dated : 02/02/2019 SCHOOL NAME KENDRIYA VIDYALAYA KOTA SCHOOL CODE 03549 ROAD BHILWARA RAJASTHAN ADDRESS KENDRIYA VIDYALAYA,KOTA AFFILIATION CODE 1700045 ROAD BHILWARA,RAJASTHAN PRINCIPAL MR ROOP SINGH DHANKARIYA PRINCIPAL'S CONTACT 9414070788 NUMBER PRINCIPAL'S EMAIL ID [email protected] PRINCIPAL'S RETIREMENT 31/03/2024 DATE SCHOOL'S CONTACT NUMBER 1482-256500 SCHOOL'S EMAIL ID [email protected] SCHOOL'S WEBSITE kvbhilwara.com SCHOOL'S FAX NUMBER 0 LANDMARK NEAR SCHOOL AHINSA CIRCLE, TILAK NAGAR YEAR OF ESTABLISHMENT 1994 AFFILIATION VALIDITY 1996 TO 2019 AFFILIATION STATUS REGULAR NAME OF THE KVS REGISTRATION DATE 15/12/1965 TRUST/SOCIETY/COMPANY SCHOOL NAME KENDRIYA VIDYALAYA KOTA SCHOOL CODE 03549 ROAD BHILWARA RAJASTHAN REGISTERED WITH SOCIETY REGISTRATION under society registration act 1860 REGISTRATION VALIDITY PERMANENT NUMBER REGISTRATION NOC ISSUING AUTHORITY cbse NOC ISSUING DATE 26/08/1996 NO OBJECTION CERTIFICATE VIEW NON PROPRIETY VIEW CHARACTER AFFIDAVIT/NON PROFIT COMPANY AFFIDAVIT FACULTY DETAILS 03549--KENDRIYA VIDYALAYA KOTA ROAD BHILWARA RAJASTHAN Dated : 02/02/2019 TOTAL NUMBER OF TEACHERS (ALL CLASSES) 23 NUMBER OF PGTs 9 NUMBER OF TGTs 7 NUMBER OF PRTs 7 NUMBER OF PETs 1 OTHER NON-TEACHING STAFF 7 TOTAL NUMBER OF TEACHERS (ALL CLASSES) 23 NUMBER OF PGTs 9 NUMBER OF MANDATORY TRAINING QUALIFIED 5 NUMBER OF TRAININGS ATTENDED BY FACULTY SINCE 8 TEACHERS LAST YEAR STUDENT DETAILS 03549--KENDRIYA VIDYALAYA KOTA ROAD BHILWARA RAJASTHAN Dated : 02/02/2019 CLASS TOTAL NUMBER OF SECTIONS TOTAL NUMBER OF INTAKE TOTAL NUMBER OF STUDENTS 1 1 51 51 2 1 49 49 3 1 54 54 4 1 51 51 5 1 55 55 6 1 53 53 7 1 57 57 CLASS TOTAL NUMBER OF SECTIONS TOTAL NUMBER OF INTAKE TOTAL NUMBER OF STUDENTS 8 1 55 55 9 1 59 59 10 1 37 37 11 2 76 76 12 2 54 54 ACADEMIC DETAILS 03549--KENDRIYA VIDYALAYA KOTA ROAD BHILWARA RAJASTHAN Dated : 02/02/2019 SUBJECTS OFFERED FOR CLASS 10 SUBJECTS OFFERED FOR CLASS 12 002---HINDI COURSE-A 065---INFORMATICS PRAC. -

Rajasthan NAMP ARCGIS
Status of NAMP Station (Rajasthan) Based on Air Quality Index Year 2010 ± Sriganganager Hanumangarh Churu Bikaner Jhunjhunu 219 373 *# Alwar(! Sikar 274 273 372 297 *# *# 409 *# Jaisalmer *# (! Bharatpur Nagaur 408 376 410 411 *# Dausa *# *# *#Jaipur 296 Jodhpur 298 412 *# (! 413 *# Dholpur *# Karauli Ajmer Sawai Madhopur Tonk Barmer Pali Bhilwara Bundi *#326 Jalor Kota# Rajsamand Chittorgarh * 325 17 Baran Sirohi *#321 *# 294 320Udaipurjk jk Jhalawar Station City Location code Area 372 Regional Office,RSPCB Residential Dungarpur Alwar 373 M/s Gourav Solvex Ltd Industrial Banswara 219 RIICO Pump House MIA Industrial 274 Regional Office, Jodhpur Industrial 273 Sojati Gate Residential 376 Mahamandir Police Thana Residential Jodhpur 411 Housing Board Residential 413 DIC Office Industrial AQI Based Pollution Categories 412 Shastri Nagar Residential 321 Regional Office MIA, Udaipur Industrial Udaipur 320 Ambamata, Udaipur (Chandpur Sattllite Hospital) Residential *# Moderate 294 Town Hall, Udaipur Residential 17 Regional Office, Kota Industrial Poor Kota 325 M/s Samcore Glass Ltd Industrial (! 326 Municipal Corporation Building, Kota Residential Satisfactory 298 RSPCB Office, Jhalana Doongari Residential jk 410 RIICO Office MIA, Jaipur Industrial 296 PHD Office, Ajmeri Gate Residential Jaipur 408 Office of the District Educational Officer, Chandpole Residential 409 Regional Office North, RSPCB,6/244 Vidyadhar Nagar Residential 297 VKIA, Jaipur (Road no.-6) Industrial Status of NAMP Station (Rajasthan) Based on Air Quality Index Year 2011 ± -
THEIR OWN COUNTRY :A Profile of Labour Migration from Rajasthan
THEIR OWN COUNTRY A PROFILE OF LABOUR MIGRATION FROM RAJASTHAN This report is a collaborative effort of 10 civil society organisations of Rajasthan who are committed to solving the challenges facing the state's seasonal migrant workers through providing them services and advocating for their rights. This work is financially supported by the Tata Trust migratnt support programme of the Sir Dorabji Tata Trust and Allied Trusts. Review and comments Photography Jyoti Patil Design and Graphics Mihika Mirchandani All communication concerning this publication may be addressed to Amrita Sharma Program Coordinator Centre for Migration and Labour Solutions, Aajeevika Bureau 2, Paneri Upvan, Street no. 3, Bedla road Udaipur 313004, Ph no. 0294 2454092 [email protected], [email protected] Website: www.aajeevika.org This document has been prepared with a generous financial support from Sir Dorabji Tata Trust and Allied Trusts In Appreciation and Hope It is with pride and pleasure that I dedicate this report to the immensely important, yet un-served, task of providing fair treatment, protection and opportunity to migrant workers from the state of Rajasthan. The entrepreneurial might of Rajasthani origin is celebrated everywhere. However, much less thought and attention is given to the state's largest current day “export” - its vast human capital that makes the economy move in India's urban, industrial and agrarian spaces. The purpose of this report is to bring back into focus the need to value this human capital through services, policies and regulation rather than leaving its drift to the imperfect devices of market forces. Policies for labour welfare in Rajasthan and indeed everywhere else in our country are wedged delicately between equity obligations and the imperatives of a globalised market place. -

Census Atlas, Part IX-B, Vol-XIV, Rajasthan
PRG. 173 B (N) (Ordy.) 1,000 CENSUS OF INDIA 1961 VOLUME XIV RAJASTHAN PART IX-B CENSUS ATLAS C. S. GUPTA OF THE INDIAN ADMINISTRATIVE SERVICE Superintendent of Census Op~rations, RajalJhan 1969 FOREWORD FEW PEOPLE REALIZE, much less appreciate, that apart from the Survey of India and the Geological Survey, the Census of India had' been perhaps the largest single producer of maps of the Indian subcontinent. Intimate collaboration between geographer and demographer began quite early in the modern era, almost two centuries before the first experiments in a permanent decennial Census were made in the 1850's. For example, the population estimates of Fort St. George, Madras, made in 1639 and 1648, and of Masulipatnam and Bombay by Dr. John Fryer, around 1672-73 were supported by cartographic documents of no mean order, Tbe first detailed modern maps, the results of Major James Rennell's stupendous Survey of 1767-74, were published in 1778-1780 and Henry Taylor Colebrooke, almost our first systematic demographer, was quick to make good use of them by making estimates of population in the East India Company's Possessions in the 1780's. Upjohn's map of Calcutta City, drawn in 1792.93, reprinted in the Census Report of Calcutta for 195 I, gives an idea of the standards of cartographic excellence reached at that period. In the first decade of the nineteenth century, Francis Buchanan Hamilton improved upon Colebrooke's method in which he was undoubtedly helped by the improved maps prepared for the areas he surve ed. It is possible that the Great Revenue Survey, begun in the middle of the last century, offered the best guarantee of the success of decennial population censuses proposed shortly before the Mutiny of 1857. -

Geography of Rajasthan
GEOGRAPHY OF RAJASTHAN RIVERS OF RAJASTHAN All aspects relating to Rivers of Rajasthan have been simplified and summarized by the Delhi Law Academy in 21 pages. This sample contains the first 3 pages… Delhi Law Academy – India’s Finest Coaching RAJASTHAN ADMINISTRATIVE SERVICE www.delhilawacademy.com All materials, copyrights and trademarks are rights of their respective owners Banas River & its Tributaries • Banas river originates in the Khamnor Hills of the Aravalli Range, near Kumbhalgarh in Rajsamand. • It is a tributary of the Chambal River and is approximately 512 kilometres in length. • It is also known as 'Van Ki Asha' (Hope of forest). • There is another river in Rajasthan with name of Banas, which flows in western direction and is also called as West Banas River. Origin Khamnor Hills, near Kumbhalgarh in Raisamand. Length 512 Kms Discharge Chambal near Rameshwar in Sawai Madhopur District States & Major Cities Nathdwara, Jahazpur and Tonk. Right Bank Tributaries Berach, Menali Left Bank Tributaries Kothari, Khari, Dai, Morel and Kalisil Major Dams Bisalpur Banas River in Indian mythology • Lord Parshuram, an avatar (incarnation) of Lord Vishnu, is linked strongly with Banas. Parshuram had killed his mother, Renukaji, on the order of his father. He went to several places seeking salvation. He saw that a calf, who had turned black on killing a man, turned white again after taking a dip in river Banas. Parshuram did the same and was relieved of the sin. The place is now called Matrikundya and falls in Bhilwara district. It is also known as the ‘Haridwar of Rajasthan’. • Jargaji, an important pilgrimage, is located around 10 km from the origin point. -

Nagaur District Survey Report
NAGAUR DISTRICT SURVEY REPORT 1 CONTENTS PAGE(S) 1. INTRODUCTION 2 2. OVERVIEW OF MINING ACTIVITY IN THE DISTRICT 8 3. THE LIST OF MINING LEASES IN THE DISTRICT 39 4. DETAILS OF ROYALTY OR REVENUE RECEIVED IN LAST 147 THREE YEARS 5. DETAILS OF PRODUCTION OF SAND OR BAJARI OR 150 MINOR MINERALS IN LAST THREE YEARS 6. PROCESS OF DEPOSITION OF SEDIMENTS IN THE RIVERS OF 152 THE DISTRICT 7. GENERAL PROFILE OF THE DISTRICT 152 8. LAND UTILIZATION PATTERN IN THE DISTRICT 161 9. PHYSIOGRAHY OF THE DISTRICT 163 10. RAINFALL 165 11. GEOLOGY AND MINERAL WEALTH 166 2 [ Nagaur District Survey Report CHAPTER 1: Introduction Nagaur district falls almost in the central part of Rajasthan covering an area of 17,718 sq.km. The district is bounded by the latitudes 26°02'12" to 27°37'39" and longitudes 73°05'20" to 75°24'. The NH-65 which connects district H.Q. with Jodhpur and NH-89 connecting it with Ajmer and Bikaner are passing through the district. It is also connected with Jaipur, Jodhpur and Bikaner through broad gauge railway line. It is oval in shape. The district forms a part of great Thar desert and a large part of it is covered by wind blown sand. The district boundary is shared by seven districts of Rajasthan viz.-Jaipur, Ajmer, Pali, Jodhpur, Bikaner, Churu and Sikar. It falls in Ajmer division and administratively divided into four sub divisional offices viz. Didwana, Nagaur, Merta, and Parbatsar. Nagaur, Merta, Jayal, Ladnun, Didwana, Nawa, Makrana, Degana, Parbatsar and Khimsar are the ten tehsil head quaters of the district. -

Geology of Rajpura-Dariba Group of Rocks
International Journal of Research and Innovations in Earth Science Volume 2, Issue 3, ISSN (Online) : 2394-1375 Geology of Rajpura-Dariba Group of Rocks P. K. Yadav Email: [email protected] Abstract – Stratigraphic position of Rajpura-Dariba Group collection of new data and in totality adopting a holistic of rocks has been worked out by different workers and integrated approach to find new sites for exploration. varied status has been given by them. These different views Study area lies around village Sindesar Khurd which is have been discussed in the present paper, Considering accessible by road from Dariba mines and Rail Magra; a lithology, airborne and ground geophysics and Tehsil headquarter. The area consists of a physiographic geochronological data in the present paper an attempt has been made to compare these different views on the ridge composed of series of hills looking like a chain of stratigraphy. On the basis of presence of basal conglomerate, train bogies. volcanics and variation in the environment of deposition a Stratigraphically the sequence in the Rajpura-Dariba new threefold classification has been proposed. Stratigraphic Group of rocks was considered by Gupta (1934) to belong status of host lithology has been identified for use as tool for to Aravalli “system.” Later Raja Rao et al. (1971) of prognostication of base metals in the Rajpura-Dariba Grou[ Geological Survey of India recognized the cover sequence of rocks. to be Pre-Aravalli meta-sediments on the basis of differences with the Aravalli‟s in lithology and grade of Keywords – Lithological Setup, Host Lithology, metamorphism. In the major stratigraphic revision, Prognostication, Stratigraphy, Structure. -

Village Bhateri, Tehsil Bassi, District Jaipur, Rajasthan List of Industries
List of industries to whom permission being accorded in 2008-09 S. No. Name Address Purpose of application Location Requirement Remarks (cu.m/day) 250 Khetan Business 23-A/1, Residency GW Clearance in respect of Village Rabcha & Oden, 58 through 1 Approval vide Corporation Pvt. Ltd Road, Udaipur-313001 their Dhanlaxmi, Vijaylaxmi Khamnor Block, Rajasmand existing letter no 21- (Rajasthan) & mahalaxmi Soapstone & District, Rajasthan openwell 4(125)/WR/CG Dolomite mines WA/07 dated 19- 5-2008 251 Singhalsons (Mines) 9A, II Floor, GW Clearance in respect of Village Girota, Sikrai Tehsil, 5 through Approval vide Chameliwala Market, their silica sand washing Dausa District, Rajasthan existing 1 t/w letter no. 21- M.I. Road, Jaipur- plant 4(188)/WR/CG 302001 (Rajasthan) WA/07 dated 19- 5-2008 252 IOL Chemicals & Trident Complex, Mansa GW Clearance in respect of Mansa Raod, Village 940 through 2 Approval vide Pharmaceuticals Ltd., Road, Village Fatehgarh Organic Chemicals & bulk Fatehgarh Channa, Barnala, t/ws tapping letter no. 21- Channa, Barnala- manufacturing drugs Punjab aquifers below 4(118)/WR/CG 148101, Punjab 150 m depth WA/07 dated 13- 5-2008 253 See below 254 See below 255 Ansal Properties & 115, Ansal Bhawan, 16 GW Clearance in respect of Village Kambopura, Tehsil 4000 trough 4 Approval vide Infrastructure Limited KG Marg, New Delhi housing colony at Sushant Karnal, District Karnal, t/ws tapping letter no. 21- City, Karnal Haryana aquifers below 4(88)/NWR/CG 150 m depth WA/07 dated 16- 5-2008 256 Narang Constructions & 409-411, N.N. Mall, GW Clearance in respect of Village Badkhalsa, Block 460 through 2 Approval vide Financiers Pvt. -
Status of Beds at Level 3 MCH Centers Total S.N
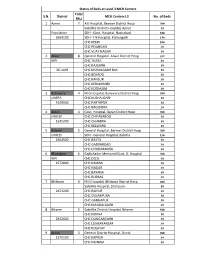
Status of Beds at Level 3 MCH Centers Total S.N. District MCH Centers L3 No. of Beds FRU 1 Ajmer 7 A K Hospital, Beawer District Hosp 300 Satellite District Hospital, Ajmer 30 Population SDH - Govt. Hospital, Nasirabad 100 2664100 SDH- Y N Hospital, Kishangarh 150 CHC KEKRI 100 CHC PISANGAN 30 CHC VIJAY NAGAR 30 2 Alwar 8 General Hospital, Alwar District Hosp 332 NIPI CHC TIJARA 30 CHC RAJGARH 50 36 LAKH CHC KISHANGARH BAS 50 CHC BEHROD 50 CHC BANSUR 30 CHC KERLIMANDI 30 CHC KOTKASIM 30 3 Banswara 4 M G Hospital, Banswara District Hosp 300 UNFPA CHC KUSHALGARH 50 1629900 CHC PARTAPUR 30 CHC BAGIDORA 30 4 Baran 4 Govt. Hospital, Baran District Hosp 300 UNICEF CHC CHIPABAROD 30 1245200 CHC CHHABRA 50 CHC KELWARA 30 5 Barmer 5 General Hospital, Barmer District Hosp 200 UNICEF SDH - General Hospital, Balotra 150 2404500 CHC BAYTU 30 CHC GADRAROAD 30 CHC DHORIMANNA 30 6 Bharatpur 6 RajBahadur Memorial Govt. D. Hospital 300 NIPI CHC DEEG 50 2572800 CHC KAMAN 30 CHC NAGAR 30 CHC BAYANA 50 CHC RUPBAS 30 7 Bhilwara 6 M G Hospital, Bhilwara District Hosp 400 Satellite Hospital, Shahpura 50 2453200 CHC RAIPUR 30 CHC GULABPURA 50 CHC GANGAPUR 50 CHC MANDALGARH 50 8 Bikaner 5 Satellite District Hospital, Bikaner 100 CHC NOKHA 50 2322600 CHC DUNGARGARH 30 CHC LUNKARANSAR 30 CHC KOLAYAT 30 9 Bundi 3 General District Hospital, Bundi 300 1170100 CHC KAPREN 30 CHC NAINWA 50 Total S.N. District MCH Centers L3 No. of Beds FRU 10 Chittorgarh 5 District Hospital, Chittorgarh 300 1629900 CHC BEGUN 50 CHC KAPASAN 50 CHC BADISADRI 50 CHC NIMBAHERA 100 11 Churu 5 D B Hospital, Churu District Hospital 225 2059300 SDH - S R J Hospital, Ratangarh 100 SDH - S B Hospital, Sujangarh 100 CHC RAJGARH 50 CHC SARDARSHAHAR 75 12 Dausa 3 District Hospital, Dausa 150 NIPI CHC LALSOT 30 1606100 CHC MAHUWA 30 13 Dholpur 4 Sadar District Hospital, Dholpur 300 1196300 CHC RAJAKHERA 30 CHC BARI 50 CHC BASERI 30 14 Dungarpur 4 General District Hospital, Dungarpur 300 UNICEF SDH - Govt. -

List of Foreign Exchange Authorised Branches in India
LIST OF FOREIGN EXCHANGE AUTHORISED BRANCHES IN INDIA SWIFT CODE ADDRESS BARBINBBTSY SPECIALISED INTEGRATED TREASURY BRANCH .Baroda Sun Towers 4th & th floor C 34 Gblock Bandra Kurla Complex Bandra East Mumbai 400051 Tel no 022 66363600 general 022 66363636 & 67592705 Fax 022 67592830 67592670 Tel : 022-67592759 /60 mob 9833832772 E mail [email protected] BARBINBBBMO MUMBAI MAIN OFFICE 10/12, Mumbai Samachar Marg, Fort, Mumbai-400 001. Tel :(DGM) 022-22048649 (Forex) 22825201 (General) 22048641 Fax : 22040494 E-mail : [email protected] BARBINBBPAT PATNA MAIN BRANCH Frazer Road, Patna 800 001. Tel : 0612 2225284/2222105/2225837) Fax :0612 2225284 E-mail : [email protected] BARBINBBJAM JAMSHEDPUR MAIN BRANCHBank of Baroda Building,.Main Road, Bistrupur Jamshedpur 831 001 Tel : 0657 424723/423770) Fax :0657 422319 E-mail : [email protected] BARBINBBBHU BHUBANESHWAR BRANCH 91/92, 1st Floor, Bapuji Nagar, Bhubaneshwar – 751 509 Khurda District Tel :0674-2532214 | 2530018 Fax : 530018 E-mail : [email protected] BARBINBBCMS CAMAC STREET BRANCH 3-B, Camac Street, Kolkata-700 016. Tel : 033 22467190 (Mgr) 22293414 (Forex) 033 22291720, 5181 (General) Fax : 033 22264576 E-mail : [email protected] BARBINBBIBB INTERNATIONAL BUSINESS BRANCH 4, India Exchange Place 1st Floor, Kolkata-700 001. Tel : 033 22422694, 22426703 (AGM) / 22434777 (CM) 033 22106721, 22422697 (Forex) Fax No.22424387 E-Mail [email protected] BARBINBBMAT CHANDAVARKAR ROAD BRANCH 309, Matunga (Central Railway) Chandavarkar Road, Mumbai-400 019. Tel : 022-24142374 (Mgr), 24100456 (Forex) 24141699, 24142399 (General) E mail [email protected] BARBINBBGHE GHATKOPAR (EAST) BRANCH A – Chetan Bldg., Rajawadi Road, Ghatkopar (East), Mumbai – 400 077 Tel : 022-25106379, 25107731,25025653(Mgr) Fax : 25135232 E-mail : [email protected] BARBINBBTHW THANE (WEST) BRANCH Annapurna Bhavan, Gokhale Road, Naupada, Thane (West) - 400 602. -

Final Population Figures, Series-18, Rajasthan
PAPER 1 OF 1982 CENSUS OF INDIA 1981 SERIES 18 RAJASTHAN fINAL POPULATION FIGU~ES (TOTAL POPULATION, SCHEDULED CASTE POPULATION AND .sCHEDULED TRIBE POPULATION) I. C. SRIVASTAVA ·1)f the Indian Administrative Service Director of Census Operations Rajasthan INTRODUCfION The final figures of total population, scheduled caste and scheduled tribe population of Rajasthan Stat~ are now ready for release at State/District/Town and Tehsil levels. This Primary Census Abs tract, as it is called, as against the provisional figures contained in our three publications viz. Paper I, fFacts & Figures' and Supplement to Paper-I has been prepared through manual tabulation by over 1400 census officials including Tabulators, Checkers and Supervisors whose constant and sustained efforts spread over twelve months enabled the Directorate to complete the work as per the schedule prescribed at the national level. As it will take a few months more to publish the final population figures at the viJ1age as well as ward levels in towns in the form of District Census Handbooks, it is hoped, this paper will meet the most essential and immediate demands of various Government departments, autonomous bodies, Cor porations, Universities and rtsearch institutions in relation to salient popUlation statistics of the State. In respect of 11 cities with One lac or more population, it has also been possible to present ~the data by municipal wards as shown in Annexure. With compliments from Director of Census Operations, Rajasthan CONTENTS INTRODUCTION (iii) Total Population, Scheduled Caste and Scheduled Tribt' Population by Districts, 1981 Total Schedu1ed Caste and Scheduled Tribe Population. ( vi) 1. Ganganagar District 1 2. -

List of Rajasthan Pradesh Congress Seva Dal Office Bearers-2017
List of Rajasthan Pradesh Congress Seva Dal Office bearers-2017 Chief Organiser 1 Shri Rakesh Pareek Shri Rakesh Pareek Chief Organiser Chief Organiser Rajasthan Pradesh Congress Seva Dal Rajasthan Pradesh Congress Seva Dal B-613 Sawai Jaisingh Highway, Vill/PO-Sarvad Ganeshganj Banipark Ajmer Jaipur Rajasthan Rajasthan Tel-09414419400 Mahila Organiser 1 Smt. Kalpana Bhatnagar Mahila Organiser Rajasthan Pradesh Congress Seva Dal 46, Navrang Nagar Beawar, Dist- Ajmer Rajasthan Tel: 09001864018 Additional Chief OrganisersP 1 Shri Hajari Lal Nagar 2 Shri Ram Kishan Sharma Additional Chief Organiser Additional Chief Organiser Rajasthan Pradesh Congress Seva Dal Rajasthan Pradesh Congress Seva Dal C 4/272 Vidyadhar Nagar Ghanshyam Ji Ka Mandir Jaipur (Rajasthan) Gangapol Bahar, Badanpura Tel:- 09214046342, 09414446342 Jaipur 09829783637 Rajasthan Tel:- 09314504631 3 Shri Hulas Chand Bhutara 4 Shri Manjoor Ahmed Additional Chief Organiser Additional Chief Organiser Rajasthan Pradesh Congress Seva Dal Rajasthan Pradesh Congress Seva Dal C-53, Panchshel Colony 4354, Mohalla Kayamkhani Purani Chungi Topkhano Ka Rasta Ajmer Road Chandpol Bazar Jaipur--302019 Jaipur Rajasthan Rajasthan Tel: 01531-220642, 09414147159 Tel: 09314603489, 08890473767 09079004827 5 Shri Bhawani Mal Ajmera 6 Shri Ram Bharosi Saini Additional Chief Organiser Additional Chief Organiser Rajasthan Pradesh Congress Seva Dal Rajasthan Pradesh Congress Seva Dal Rahul Electricals, V/Post- Chantali Ganesh Shopping Teh- Wair Complex, Opp.R No-2, Dist- Bharatpur VKI Chonu Rd. Rajasthan