On the Value of Therapeutic Interventions Targeting the Complement System in Acute Myocardial Infarction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

By Map44 Pathway Activation in a Manner Inhibitable Pattern
Co-Complexes of MASP-1 and MASP-2 Associated with the Soluble Pattern-Recognition Molecules Drive Lectin Pathway Activation in a Manner Inhibitable This information is current as by MAp44 of September 28, 2021. Søren E. Degn, Lisbeth Jensen, Tomasz Olszowski, Jens C. Jensenius and Steffen Thiel J Immunol 2013; 191:1334-1345; Prepublished online 19 June 2013; Downloaded from doi: 10.4049/jimmunol.1300780 http://www.jimmunol.org/content/191/3/1334 http://www.jimmunol.org/ Supplementary http://www.jimmunol.org/content/suppl/2013/06/19/jimmunol.130078 Material 0.DC1 References This article cites 43 articles, 23 of which you can access for free at: http://www.jimmunol.org/content/191/3/1334.full#ref-list-1 Why The JI? Submit online. by guest on September 28, 2021 • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2013 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Co-Complexes of MASP-1 and MASP-2 Associated with the Soluble Pattern-Recognition Molecules Drive Lectin Pathway Activation in a Manner Inhibitable by MAp44 Søren E. -

Ncounter Human Inflammation V2 Panel Gene List
nCounter Human Inflammation V2 Panel Gene List Official Symbol Accession Alias / Prev Symbol GO Annotation* Official Full Name Intrinsic To Plasma Membrane,Intrinsic To Membrane,Membrane Part,Membrane,Integral To Membrane,Integral To Plasma Membrane,Plasma Membrane Part,Plasma Membrane,Signal Transduction,Cell Surface Receptor Linked Signal Transduction Go 0007166,Defense Response,Inflammatory Response,Response To Stress,Response To External AGER NM_001136.3 RAGE Stimulus,Response To W advanced glycosylation end product-specific receptor Cytoplasmic Part,Membrane,Cytoplasm,Cytosol,Plasma Membrane,Regulation Of Biological Quality,Positive Regulation Of Cell Proliferation,Cell Development,Negative Regulation Of Apoptosis,Programmed Cell Death,Regulation Of Growth,Carboxylic Acid Metabolic ALOX12 NM_000697.1 12-LOX, 12S-LOX, LOG12 Process,Fatty Acid Oxidation,Negative Regulation Of Cellular Process,Regulation Of Cell arachidonate 12-lipoxygenase Defense Response,Inflammatory Response,Response To Stress,Response To External ALOX15 NM_001140.3 15-LOX-1, 15LOX-1 Stimulus,Response To Wounding,Oxidoreductase Activity arachidonate 15-lipoxygenase ALOX5 NM_000698.2 5-LO, 5-LOX, 5LPG, LOG5 Oxidoreductase Activity arachidonate 5-lipoxygenase Extracellular Region,Extracellular Region Part,Extracellular Space,Cell Cell Signaling,Cell AREG NM_001657.2 AR, CRDGF, SDGF Proliferation Go 0008283,Receptor Binding,Growth Factor Activity amphiregulin Cytoplasm,Carboxylic Acid Metabolic Process,Glutamine Family Amino Acid Metabolic Process,Amino Acid Metabolic -

The Serine Protease Domain of MASP-3: Enzymatic Properties and Crystal Structure in Complex with Ecotin
The serine protease domain of MASP-3: enzymatic properties and crystal structure in complex with ecotin. Christine Gaboriaud, Rajesh Kumar Gupta, Lydie Martin, Monique Lacroix, Laurence Serre, Florence Teillet, Gérard J Arlaud, Véronique Rossi, Nicole Thielens To cite this version: Christine Gaboriaud, Rajesh Kumar Gupta, Lydie Martin, Monique Lacroix, Laurence Serre, et al.. The serine protease domain of MASP-3: enzymatic properties and crystal structure in complex with ecotin.. PLoS ONE, Public Library of Science, 2013, 8 (7), pp.e67962. 10.1371/journal.pone.0067962. inserm-00868926 HAL Id: inserm-00868926 https://www.hal.inserm.fr/inserm-00868926 Submitted on 2 Oct 2013 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. The Serine Protease Domain of MASP-3: Enzymatic Properties and Crystal Structure in Complex with Ecotin Christine Gaboriaud1,2,3*, Rajesh Kumar Gupta1,2,3¤a, Lydie Martin1,2,3, Monique Lacroix1,2,3, Laurence Serre3,1¤b, Florence Teillet1,2,3,Ge´rard J. Arlaud1,2,3,Ve´ronique Rossi1,2,3, Nicole M. Thielens1,2,3 1 Institut de Biologie Structurale (IBS), Direction des Sciences du Vivant, Commissariat a` l’Energie Atomique et aux Energies Alternatives, Grenoble, France, 2 IBS, Centre National de la Recherche Scientifique, Grenoble, France, 3 IBS, Universite´ Grenoble Alpes, Grenoble, France Abstract Mannan-binding lectin (MBL), ficolins and collectin-11 are known to associate with three homologous modular proteases, the MBL-Associated Serine Proteases (MASPs). -

Human Map44 HK359
Human MAp44 HK359 Edition 05-13 ELISA KIT PRODUCT INFORMATION & MANUAL Read carefully prior to starting procedures! For use in laboratory research only Not for clinical or diagnostic use Note that this user protocol is not lot-specific and is representative for the current specifications of this product. Please consult the vial label and the Certificate of Analysis for information on specific lots. Also note that shipping conditions may differ from storage conditions. For research use only. Not for use in or on humans or animals or for diagnostics. It is the responsibility of the user to comply with all local/state and federal rules in the use of this product. Hycult Biotech is not responsible for any patent infringements that might result from the use or derivation of this product. TABLE OF CONTENTS Page 1. Intended use ..................................................................................................................2 2. Introduction ....................................................................................................................2 3. Kit features ....................................................................................................................2 4. Protocol overview ..........................................................................................................3 5. Kit components and storage instructions .......................................................................4 Materials required but not provided 4 6. Warnings and precautions .............................................................................................5 -
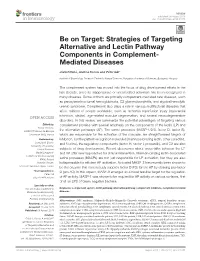
Strategies of Targeting Alternative and Lectin Pathway Components in Complement- Mediated Diseases
REVIEW published: 08 August 2018 doi: 10.3389/fimmu.2018.01851 Be on Target: Strategies of Targeting Alternative and Lectin Pathway Components in Complement- Mediated Diseases József Dobó, Andrea Kocsis and Péter Gál* Institute of Enzymology, Research Centre for Natural Sciences, Hungarian Academy of Sciences, Budapest, Hungary The complement system has moved into the focus of drug development efforts in the last decade, since its inappropriate or uncontrolled activation has been recognized in many diseases. Some of them are primarily complement-mediated rare diseases, such as paroxysmal nocturnal hemoglobinuria, C3 glomerulonephritis, and atypical hemolytic uremic syndrome. Complement also plays a role in various multifactorial diseases that affect millions of people worldwide, such as ischemia reperfusion injury (myocardial infarction, stroke), age-related macular degeneration, and several neurodegenerative disorders. In this review, we summarize the potential advantages of targeting various Edited by: complement proteins with special emphasis on the components of the lectin (LP) and Nicole Thielens, UMR5075 Institut de Biologie the alternative pathways (AP). The serine proteases (MASP-1/2/3, factor D, factor B), Structurale (IBS), France which are responsible for the activation of the cascade, are straightforward targets of Reviewed by: inhibition, but the pattern recognition molecules (mannose-binding lectin, other collectins, Cordula M. Stover, and ficolins), the regulatory components (factor H, factor I, properdin), and C3 are also University of Leicester, United Kingdom subjects of drug development. Recent discoveries about cross-talks between the LP Maciej Cedzynski, and AP offer new approaches for clinical intervention. Mannan-binding lectin-associated Institute for Medical Biology (PAN), Poland serine proteases (MASPs) are not just responsible for LP activation, but they are also Christian Drouet, indispensable for efficient AP activation. -
Role of Complement in Diabetes
This is a repository copy of Role of complement in diabetes. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/151783/ Version: Accepted Version Article: Ajjan, RA and Schroeder, V (2019) Role of complement in diabetes. Molecular Immunology, 114. pp. 270-277. ISSN 0161-5890 https://doi.org/10.1016/j.molimm.2019.07.031 (c) 2019, Elsevier Ltd. This manuscript version is made available under the CC-BY-NC-ND 4.0 license https://creativecommons.org/licenses/by-nc-nd/4.0/ Reuse This article is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs (CC BY-NC-ND) licence. This licence only allows you to download this work and share it with others as long as you credit the authors, but you can’t change the article in any way or use it commercially. More information and the full terms of the licence here: https://creativecommons.org/licenses/ Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Molecular Immunology, Special Issue EMCHD 2019 Review Article Role of Complement in Diabetes Ramzi A. Ajjan a, Verena Schroeder b* a Leeds Institute for Cardiovascular and Metabolic Medicine, School of Medicine, University of Leeds, Leeds, United Kingdom b Experimental Haemostasis Group, Department for BioMedical Research (DBMR), University of Bern, Bern, Switzerland * Corresponding author: Verena Schroeder Experimental Haemostasis Group Department for BioMedical Research (DBMR) University of Bern Murtenstrasse 40 3008 Bern Switzerland Tel.: +41 31 632 9618 E-mail: [email protected] 1 Abstract Accumulating evidence suggests a role for the complement system in the pathogenesis of diabetes and the vascular complications that characterise this condition. -

MASP-1 and MASP-2 Do Not Activate Pro-FD in Resting Human
MASP-1 and MASP-2 do not activate pro-FD in resting human blood, while MASP-3 is a potential activator: kinetic analysis involving specific MASP-1 and MASP-2 inhibitors Gábor Oroszlán *, Elod Kortvely †, Dávid Szakács ‡, Andrea Kocsis *, Sascha Dammeier §, Anne Zeck ¶, Marius Ueffing †,§, Péter Závodszky *, Gábor Pál ‡ , Péter Gál *2, József Dobó *2 * Institute of Enzymology, Research Centre for Natural Sciences, Hungarian Academy of Sciences, Magyar tudósok krt. 2, H-1117, Budapest, Hungary † Institute for Ophthalmic Research, University of Tübingen, Röntgenweg 11, 72076 Tübingen, Germany ‡ Department of Biochemistry, Eötvös Loránd University, 1/C Pázmány Péter street, H-1117, Budapest, Hungary § Institute for Ophthalmic Research, Medical Proteome Center, University of Tübingen, Nägelestrasse 5, 72074 Tübingen, Germany ¶ Natural and Medical Sciences Institute at the University of Tübingen, Department of Bioanalytics, Markwiesenstrasse 55, 72770 Reutlingen, Germany 2 Address correspondence and reprint request to J. Dobó, and/or P. Gál, Institute of Enzymology, Research Centre for Natural Sciences, Hungarian Academy of Sciences, Magyar tudósok krt. 2, H- 1117, Budapest, Hungary, e-mail: [email protected] (J.D.), or [email protected] (P.G.), phone: +36-1-3826768, fax: +36-1-3826295 Running title: Kinetics of pro-FD activation Keywords (not in the title): lectin pathway; innate immunity; mannan-binding lectin; MBL- associated serine protease; thrombin; trypsin 1 Abstract It had been thought that complement factor D (FD) is activated at the site of synthesis and only FD lacking a propeptide is present in blood. The serum of MASP-1/3(-/-) mice contains pro-FD and has markedly reduced alternative pathway activity. -

Targeting of Liver Mannan-Binding Lectin
Targeting of Liver Mannan-Binding Lectin−Associated Serine Protease-3 with RNA Interference Ameliorates Disease in a Mouse Model of Rheumatoid Arthritis Downloaded from Nirmal K. Banda, Dhruv Desai, Robert I. Scheinman, Rasmus Pihl, Hideharu Sekine, Teizo Fujita, Vibha Sharma, Annette G. Hansen, Peter Garred, Steffen Thiel, Anna Borodovsky and V. Michael Holers http://www.immunohorizons.org/ ImmunoHorizons 2018, 2 (8) 274-295 http://www.immunohorizons.org/ doi: https://doi.org/10.4049/immunohorizons.1800053 http://www.immunohorizons.org/content/2/8/274 This information is current as of September 25, 2021. Supplementary http://www.immunohorizons.org/content/suppl/2018/09/14/2.8.274.DCSupp Material lemental by guest on September 25, 2021 References This article cites 60 articles, 25 of which you can access for free at: by guest on September 25, 2021 http://www.immunohorizons.org/content/2/8/274.full#ref-list-1 Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://www.immunohorizons.org/alerts ImmunoHorizons is an open access journal published by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 All rights reserved. ISSN 2573-7732. RESEARCH ARTICLE Innate Immunity Targeting of Liver Mannan-Binding Lectin–Associated Serine Protease-3 with RNA Interference Ameliorates Disease in a Mouse Model of Rheumatoid Arthritis Nirmal K. Banda,*,1 Dhruv Desai,† Robert I. Scheinman,‡ Rasmus Pihl,§ Hideharu Sekine,{ Teizo Fujita,{ Vibha Sharma,|| Downloaded from Annette -

Essential Role for the Lectin Pathway in Collagen Antibody–Induced
Essential Role for the Lectin Pathway in Collagen Antibody−Induced Arthritis Revealed through Use of Adenovirus Programming Complement Inhibitor MAp44 This information is current as Expression of September 26, 2021. Nirmal K. Banda, Gaurav Mehta, Troels R. Kjaer, Minoru Takahashi, Jerome Schaack, Thomas E. Morrison, Steffen Thiel, William P. Arend and V. Michael Holers J Immunol 2014; 193:2455-2468; Prepublished online 28 Downloaded from July 2014; doi: 10.4049/jimmunol.1400752 http://www.jimmunol.org/content/193/5/2455 http://www.jimmunol.org/ Supplementary http://www.jimmunol.org/content/suppl/2014/07/26/jimmunol.140075 Material 2.DCSupplemental References This article cites 62 articles, 30 of which you can access for free at: http://www.jimmunol.org/content/193/5/2455.full#ref-list-1 by guest on September 26, 2021 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2014 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Essential Role for the Lectin Pathway in Collagen Antibody– Induced Arthritis Revealed through Use of Adenovirus Programming Complement Inhibitor MAp44 Expression Nirmal K. -
The Evolution of the Immune System: Conservation and Diversification
Title The Evolution of the Immune System Conservation and Diversification Page left intentionally blank The Evolution of the Immune System Conservation and Diversification Davide Malagoli Department of Life Sciences Biology Building, University of Modena and Reggio Emilia, Modena, Italy AMSTERDAM • BOSTON • HEIDELBERG • LONDON NEW YORK • OXFORD • PARIS • SAN DIEGO SAN FRANCISCO • SINGAPORE • SYDNEY • TOKYO Academic Press is an imprint of Elsevier Academic Press is an imprint of Elsevier 125 London Wall, London EC2Y 5AS, United Kingdom 525 B Street, Suite 1800, San Diego, CA 92101-4495, United States 50 Hampshire Street, 5th Floor, Cambridge, MA 02139, United States The Boulevard, Langford Lane, Kidlington, Oxford OX5 1GB, UK Copyright © 2016 Elsevier Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek per- mission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions. This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein). Notices Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary. Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds, or experiments described herein. -

Role of MASP-3 in the Physiological Activation of Factor D of the Alternative Complement Pathway
Cutting Edge: Role of MASP-3 in the Physiological Activation of Factor D of the Alternative Complement Pathway This information is current as Manabu Hayashi, Takeshi Machida, Yumi Ishida, Yusuke of September 27, 2021. Ogata, Tomoko Omori, Mika Takasumi, Yuichi Endo, Toshiyuki Suzuki, Masayuki Sekimata, Yoshimi Homma, Masahito Ikawa, Hiromasa Ohira, Teizo Fujita and Hideharu Sekine J Immunol published online 9 August 2019 Downloaded from http://www.jimmunol.org/content/early/2019/08/09/jimmun ol.1900605 Supplementary http://www.jimmunol.org/content/suppl/2019/08/09/jimmunol.190060 http://www.jimmunol.org/ Material 5.DCSupplemental Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists by guest on September 27, 2021 • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2019 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Published August 9, 2019, doi:10.4049/jimmunol.1900605 Cutting Edge: Role of MASP-3 in the Physiological Activation of Factor D of the Alternative Complement Pathway Manabu Hayashi,*,† Takeshi Machida,* Yumi Ishida,* Yusuke Ogata,* Tomoko Omori,* Mika Takasumi,*,† Yuichi Endo,* Toshiyuki Suzuki,‡ ‡ x { † Masayuki Sekimata,‖ Yoshimi Homma, Masahito Ikawa, Hiromasa Ohira, Teizo Fujita, and Hideharu Sekine* The complement system, a part of the innate immune PRMs of the LP form a complex with MBL-associated serine system, can be activated via three different pathways. -

MASP-1 of the Complement System Promotes Clotting Via Prothrombin
This accepted author manuscript is copyrighted and published by Elsevier. It is posted here by agreement between Elsevier and MTA. The definitive version of the text was subsequently published in 2015 Mol. Immunol. 65, 398–405. doi:10.1016/j.molimm.2015.02.014. Available under license CC-BY-NC-ND. MASP-1 of the complement system promotes clotting via prothrombin activation Lorenz Jenny a,b , József Dobó c, Péter Gál c, Verena Schroeder a,b a University Clinic of Haematology, Haemostasis Research Laboratory, University Hospital Bern, 3010 Bern, Switzerland b Department of Clinical Research, University of Bern, Bern, Switzerland; c Institute of Enzymology, Research Centre for Natural Sciences, Hungarian Academy of Sciences, Magyar tudósok krt 2, H-1113 Budapest, Hungary Corresponding author: Verena Schroeder, PhD University Clinic of Haematology Haemostasis Research Laboratory University Hospital Inselspital 3010 Bern, Switzerland Tel. +41 31 632 9618, Fax +41 31 632 1882 E-mail [email protected] 1 Abbreviations CAPS, N-cyclohexyl-3-aminopropanesulfonic acid; CFT, clot formation time; CT, clotting time; FXa, activated factor X; FXIII, factor XIII; MAp, MBL-associated protein; MASP, mannan-binding lectin- associated serine protease; MBL, mannose binding lectin; MCF, maximum clot firmness; MES, 2- (N-Morpholino)- ethanesulfonic acid; PAR4, protease activated receptor 4; PPP, platelet-poor plasma; PT-DP, Prothrombin-depleted plasma; PVDF, polyvinylidene difluoride; rMASP-1cf, MASP-1 catalytic fragment; SGMI, Schistocerca gregaria protease inhibitor (SGPI)-based MASP- inhibitor; WB, whole blood. Abstract Mannan-binding lectin-associated serine protease-1 (MASP-1), a protein of the complement lectin pathway, resembles thrombin in terms of structural features and substrate specificity, and it has been shown to activate coagulation factors.