Badenoch & Strathspey Redesign Recommendation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Contract Between Scottish Ministers
CONTRACT BETWEEN SCOTTISH MINISTERS AND GEOAMEY PECS LTD FOR THE SCOTTISH COURT CUSTODY AND PRISONER ESCORT SERVICE (SCCPES) REFERENCE: 01500 MARCH 2018 Official No part of this document may be disclosed orally or in writing, including by reproduction, to any third party without the prior written consent of SPS. This document, its associated appendices and any attachments remain the property of SPS and will be returned upon request. 1 | P a g e 01500 Scottish Court Custody and Prisoner Escort Service (SCCPES) FORM OF CONTRACT CONTRACT No. 01500 This Contract is entered in to between: The Scottish Ministers, referred to in the Scotland Act 1998, represented by the Scottish Prison Service at the: Scottish Prison Service Calton House 5 Redheughs Rigg Edinburgh EH12 9HW (hereinafter called the “Purchaser”) OF THE FIRST PART And GEOAmey PECS Ltd (07556404) The Sherard Building, Edmund Halley Road Oxford OX4 4DQ (hereinafter called the “Service Provider”) OF THE SECOND PART The Purchaser hereby appoints the Service Provider and the Service Provider hereby agrees to provide for the Purchaser, the Services (as hereinafter defined) on the Conditions of Contract set out in this Contract. The Purchaser agrees to pay to the Service Provider the relevant sums specified in Schedule C and due in terms of the Contract, in consideration of the due and proper performance by the Service Provider of its obligations under the Contract. The Service Provider agrees to look only to the Purchaser for the due performance of the Contract and the Purchaser will be entitled to enforce this Contract on behalf of the Scottish Ministers. -
Caithness and Sutherland Proposed Local Development Plan Committee Version November, 2015
Caithness and Sutherland Proposed Local Development Plan Committee Version November, 2015 Proposed CaSPlan The Highland Council Foreword Foreword Foreword to be added after PDI committee meeting The Highland Council Proposed CaSPlan About this Proposed Plan About this Proposed Plan The Caithness and Sutherland Local Development Plan (CaSPlan) is the second of three new area local development plans that, along with the Highland-wide Local Development Plan (HwLDP) and Supplementary Guidance, will form the Highland Council’s Development Plan that guides future development in Highland. The Plan covers the area shown on the Strategy Map on page 3). CaSPlan focuses on where development should and should not occur in the Caithness and Sutherland area over the next 10-20 years. Along the north coast the Pilot Marine Spatial Plan for the Pentland Firth and Orkney Waters will also influence what happens in the area. This Proposed Plan is the third stage in the plan preparation process. It has been approved by the Council as its settled view on where and how growth should be delivered in Caithness and Sutherland. However, it is a consultation document which means you can tell us what you think about it. It will be of particular interest to people who live, work or invest in the Caithness and Sutherland area. In preparing this Proposed Plan, the Highland Council have held various consultations. These included the development of a North Highland Onshore Vision to support growth of the marine renewables sector, Charrettes in Wick and Thurso to prepare whole-town visions and a Call for Sites and Ideas, all followed by a Main Issues Report and Additional Sites and Issues consultation. -

4.11 Chief Executive and Directors Report
NHS Highland Board 24 July 2018 Item 4.11 CHIEF EXECUTIVE AND DIRECTORS REPORT – EMERGING ISSUES AND UPDATES Report by Elaine Mead, Chief Executive The Board is asked to: • Note the updates provided in the report. Chief Officer Argyll and Bute Health and Social Care Partnership It is with much regret to report that Christina West has resigned from the post of Chief Officer for Argyll and Bute Health and Social Care Partnership with a leaving date of 30th September 2018. Integration of health and social care has been one of the most significant changes in the public sector for decades. Under Christina’s Leadership she leaves Argyll and Bute’s Health and Social Care Partnership in a positive position to move forward, with plans in place to redesign services not least to meet the demographic challenges. Christina takes with her our grateful thanks, for her hard work, determination and commitment to developing health and social care services for the people of Argyll and Bute. She embraced the Highland Quality Approach and has been an invaluable member of NHS Highland’s Senior Leadership team. The recruitment process is underway to secure a new Chief Officer. Dr Grays Temporary Service Model for Women and Children’s services A new temporary service model for Women and Children’s services at Dr Gray’s Hospital is to be put in place to allow maternity and paediatric service to continue in Elgin. The change comes after NHS Education for Scotland said initial indications were that only two trainee doctors had elected to work at Dr Gray’s at the next intake in August – six less than the number required. -

Parliamentary Questions on Covid-19 and Answers by the Scottish Government
PARLIAMENTARY QUESTIONS ON COVID-19 AND ANSWERS BY THE SCOTTISH GOVERNMENT Thursday 2 July 2020 Written questions lodged on 2 July can be found on page 12 of this document. ANSWERS TO PARLIAMENTARY QUESTIONS (Received on 2 July) Government Initiated Question George Adam (Paisley) (Scottish National Party): To ask the Scottish Government when it will publish an update on Scotland’s approach to physical distancing. S5W-30404 John Swinney: The Scottish Government has today published COVID-19: Scotland’s route map through and out of the crisis – Update on approach to physical distancing in light of advice from the Scottish Government COVID-19 Advisory Group which provides an update on the approach to physical distancing in Scotland as we move through Phase 2 and Phase 3 of the Route Map. This approach continues to be informed by evidence and has been updated in light of advice from the Scottish Government COVID-19 Advisory Group which has also been published today. The publication also updates on the final stage of Phase 2 of Scotland’s Route Map. Continued progress in suppressing the virus, as measured by the latest data, means that we are able to confirm the indicative dates for the remainder of Phase 2, concerning relaxation of the 5-mile guidance on travel for leisure purposes, the re- opening of self-contained, self-catering accommodation and the re-opening of outdoor hospitality. Changes to allow children and young-people more opportunity to meet up are also set out. Ministerial portfolio: Economy, Fair Work and Culture Iain Gray (East Lothian) (Scottish Labour): To ask the Scottish Government whether restrictions have been placed on the Individual Training Account scheme for 2020-21 because of the COVID-19 pandemic and, if so, in what sectors. -

Migdale Hospital a Case Study
Migdale Hospital A Case Study 1 Migdale Hospital Overview The replacement of the Migdale Hospital in Bonar Bridge is a good example of a rural community hospital and sets a helpful precedent for community facilities in remote locations. The product of 15 years work, the project involved considerable consultation with community groups, local councillors, staff, patients, and patient representatives before being constructed and completed in June 2011. The new facility replaces an older hospital building, originally designed as a Victorian ‘Poorhouse’ to support and provide housing for the dependent or needy. A decision was made to sell the original hospital which had become unfit for purpose. This was in part due to restrictions caused by the narrow corridors, 4 and 5 bed wards, inadequate sanitary facilities and split-level Front elevation of Migdale hospital, accommodation, all of which affected the use by long-stay elderly patients. overlooking the Kyle of Sutherland Retention would require a total refurbishment which was deemed unviable. Image credit: John Paul Photography It was considered that a new hospital could more easily provide better integrated care and single-bed rooms, in line with Scottish Government Health and Social Care Directorate (SGHSCD) policy. The new Migdale hospital is a 22-bed community health unit serving the north and west areas of NHS Highland. The hospital has two wards: an Older Adult Mental Health Assessment Unit (Strathy) and a GP Acute Unit (Kyelsku). A number of outpatient services are also provided including Physiotherapy, Occupational Therapy, Audiology, Rehabilitation Classes, and Memory Clinics. Built on a steeply sloping site in Bonar Bridge, the hospital lies close to the main travel routes between Inverness and the North and West of Scotland. -

Appeal Citation List External
The Highland and Western Isles Valuation Joint Board Citation List Valuation Appeal Committee Hearing Date of Hearing : 05 November 2019 Citations Issued : 23 July 2019 Seq Appeal Reference Description & Situation No Number 1 263201 01/05/406034/9 Hospital, Timbury Unit, Hospital Road, Wick, Caithness, KW1 5NQ 2 263200 01/05/703006/0 Hospital, Caithness General Hospital, Rosebank, Wick, Caithness, KW1 5LF 3 284334 01/05/756091/8 Retail Warehouse, Unit 1, South Road Retail Park, Wick, KW1 5NU 4 281318 01/12/037710/0 Premises (Miscellaneous), Thrumster, Wick, Caithness, KW1 5TR 5 277814 01/14/069800/3 Hotel, Portland Arms, Lybster, Caithness, KW3 6BS 6 263286 01/15/011230/4 Hospital, Dunbar Hospital, Ormlie Road, Thurso, Caithness, KW14 7XE 7 281311 01/16/032500/2 Garage (Commercial), Old Church, Harland Gardens, Castletown, Thurso, Caithness, KW14 8UD 8 263184 02/05/008305/1 Hospital, New Migdale Hospital, Cherry Grove, Bonar Bridge, Ardgay, Sutherland, IV24 3ER 9 263189 02/08/002700/1 Hospital, Lawson Memorial, Golspie, Sutherland, KW10 6SR 10 260760 02/09/009101/0 Hotel, The Nip Inn, New Buildings, Main Street, Lairg, Sutherland, IV27 4DB 11 290055 02/12/024400/5 Self Cat Unit, Hope Lodge, Hope, Altnaharra, Lairg, Sutherland, IV27 4UJ 12 259201 02/14/000550/9 Hydro Elec Works, Kintradwell Burn, Kintradwell, Brora, Sutherland, KW9 6LU 13 269064 03/02/001400/4 Hydro Elec Works, Ledgowan Hydro Scheme, Ledgowan, Achnasheen, Ross-shire, IV22 2EN 14 268843 03/02/002650/4 Hydro Elec Works, Loch Rosque Hydro Scheme, Achnasheen, Ross-shire, IV22 -
Item 4: Caithness and Sutherland Local Development Plan
THE HIGHLAND COUNCIL Agenda 4. Item CAITHNESS AND SUTHERLAND AREA COMMITTEE Report CS/12/ No 15 26 MAY 2015 CAITHNESS AND SUTHERLAND LOCAL DEVELOPMENT PLAN Report by Director of Development and Infrastructure Summary This report presents a summary of matters raised in responses to the Main Issues Report (MIR) consultation for the Caithness and Sutherland Local Development Plan (CaSPlan), which ran from 30 October 2014 to 6 February 2015. It also presents a summary of matters raised in responses to the Additional Sites and Issues consultation that was undertaken from 13 March 2015 to 24 April 2015. Officers have been giving initial consideration to the matters raised and the report includes recommendations for the Council’s interim position on these for Area Committee’s consideration. The Area Committee is asked to agree the Council’s interim position to guide the preparation of the Proposed Plan, to be referred to the PDI Committee for consideration later in 2015 alongside ongoing environmental assessment and other actions to be undertaken. 1. Background 1.1 Following Area Committee’s approval of the Main Issues Report for the Caithness and Sutherland Local Development Plan at its meeting on 23 September 2014, the MIR and an accompanying Environmental Report were published on 30 October 2014 for public consultation. The consultation ran for a total of 14 weeks; the original deadline of 29 January 2015 was extended to 6 February 2015 due to the postponement and rescheduling of the Brora workshop. 1.2 The MIR was not intended as a draft version of the plan; it was a discussion document that set out initial ideas and options for what the plan needs to achieve for people and places in the area and the Council’s initial preferences for where new development might be located. -

Shinty Yearbook
YEARBOOK REVIEW OF TWENTY NINETEEN SHINTY YEARBOOK | Review of 2019 Page 1 Page 2 SHINTY YEARBOOK | Review of 2019 PRESIDENT’S REPORT Once again, as President of the Camanachd Association, it is my place as the newly elected pleasure to commend the latest edition of the Shinty Year Book to Lib Dem M.P. for North-East your attention. Each year, this publication serves as an important Fife. We will not lose touch record of everything that has occurred in our ancient sport over the with Wendy and thank her past twelve months- and this year in particular there is much to be for her offer of continued positive about in the world of Shinty. support when needed. Our C.A. staff, under the guidance of our CEO, Derek Keir, are fully It is also with regret that committed to providing the best service possible. Under Derek I inform you that two old there is a real team spirit about the office. It is an extremely busy friends of the Association, place where complex issues have to be dealt with on a daily basis. our Chieftain Jock Turner The addition in 2018 of Deborah MacPherson and Aarron Duncan- and our Vice- Chieftain Alex MacLeod in 2019 to our team has made a massive impact. Their skills, MacNaughton have decided when added to the experience and dedication of the others, make it a to step aside. We deeply very competent unit. My gratitude extends to all the Board members, appreciate their time and support and thank them sincerely for their the volunteers on all of our subcommittees and of course all our contributions to our sport. -

Appendix 10: Badenoch & Strathspey Redesign Clinical Service Model
Appendix 10: Badenoch & Strathspey Redesign Clinical Service Model Introduction This document sets out the high-level clinical specification to underpin the future model for health and social care services across Badenoch & Strathspey. The service model was agreed as part of the major service change process including a three month public consultation. Some of the detail reflects feed-back received during the Options Appraisal process and public consultation. There have also been a series of clinical workshop and meetings to discuss the model and the component parts of the service and this specification reflects those discussions. Locality profiles have been studied and a bed modelling exercise completed. The specification is broken down into a number of sections with management and professional leads identified. Within each section there is a brief description of what will be provided and any further work required prior to submission of Outline Business Case Outline of services 1. Health Centres 2. Hospital inpatient beds 3. Enhanced Community Services and delivery of integrated care 3.1 Dementia 3.2 Care at Home 3.3 Equipment/Aids and Adaptations and Handyperson 3.4 Other Community Services 4. Tele-care and assisted technologies 5. Day Service – (Aviemore) 6. Care Homes 6.1 Step Up – Step Down / Flexible Use Beds 7. End of Life Care 8. Outpatient Services 9. Daycase Services 10. X-Ray Services 11. Out of Hours Service 12. Minor Injury Services 13. Scottish Ambulance Service (SAS) 14. Physiotherapy 15. Other AHP Services 16. Care and Learning (formerly known as Children’s Services) 17. Dentistry 18. Commissioning arrangements and contracts 19. -

Delivering Practical Partnerships to Tackle Fuel Poverty and Improve Energy Efficiency Teresa Bray Chief Executive Warm Recovery – the Plan
Inspiring change for people and the environment Delivering practical partnerships to tackle fuel poverty and improve energy efficiency Teresa Bray Chief Executive Warm Recovery – The Plan • Edinburgh and Lothian Health Foundation • 2 Year project supporting patients on discharge from hospital – 2014/16 • Respiratory nurses and discharge staff at Royal Infirmary Edinburgh and Western General • Senior level buy in during development Warm Recovery – Delivery • Minimal Senior support at delivery stage • Busy delivery staff at Discharge Hubs • Requirement for NHS Lothian email address for referrals • Successes through Astley Ainsley and Family Nurse partnership • Local Opportunities for Older People wider Third Sector Support at home • Learnings Home Energy Scotland support • Impartial advice and support supported by the Scottish Government, managed by the Energy Saving Trust and delivered across Scotland • Referrals to Warmer Homes Scotland for heating and insulation • Links in to other organisations NHS Highland Community Hospitals • Regular presence at Raigmore • Following Home Energy Scotland outreach work, Lorraine Coe, NHS Highland Sutherland District Lawson Memorial Hospital Manager driving force. • Referrals at discharge. • Extends reach to very vulnerable households • Data protection challenging Migdale Hospital Outcomes • 45 referrals • 16 home visits • 7 Warmer Homes Scotland referrals • 16 onward referrals and signposting • Currently being rolled out to community health teams in Suhterland, wider roll out being considered • Regular -
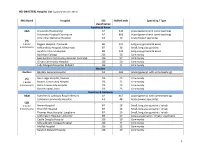
MASTER) Hospital List (Updated October 2015
HEI (MASTER) Hospital List (updated October 2015) NHS Board Hospital ISD Staffed beds Speciality / Type classification Ayrshire & Arran A&A University Hospital Ayr A2 343 Acute (general with some teaching) University Hospital Crosshouse A2 666 Acute (general with some teaching) Arran War Memorial Hospital A3 19 Acute (mixed speciality) (9) 3 acute Biggart Hospital, Prestwick B6 121 Long stay geriatric & acute 6 community Kirklandside Hospital, Kilmarnock B7 36 Small, long stay geriatric Ayrshire Central Hospital B8 142 Long stay geriatric & acute Davidson Cottage J26 26 Community East Ayrshire Community Hospital, Cumnock J26 57 Community Girvan Community Hospital J26 20 Community Lady Margaret Hospital, Millport J26 9 Community Borders Borders Borders General Hospital A2 265 Acute (general, with some teaching) (5) Hay Lodge Hospital, Peebles J26 23 Community 1 acute Hawick Community Hospital J26 22 Community 4 community Kelso Community Hospital J26 23 Community Knoll Hospital, Duns J26 23 Community Dumfries & Galloway D&G Dumfries & Galloway Royal Infirmary A2 367 Acute (general, with some teaching) Galloway Community Hospital A3 48 Acute (mixed speciality) (10) 2 acute Annan Hospital B7 18 Small, long stay geriatric / rehab 8 community Thornhill Hospital B7 13 Small, long stay geriatric / rehab Thomas Hope Hospital, Langholm B7 10 Small, long stay geriatric / rehab Lochmaben Hospital, Lockerbie B9 17 Long stay geriatric / rehab / psychiatry Castle Douglas Hospital J26 19 Community Kirkcudbright Cottage Hospital J26 9 Community Moffat Hospital J26 12 Community Newton Stewart Hospital J26 19 Community 1 HEI (MASTER) Hospital List (updated October 2015) Fife Fife Victoria Hospital, Kirkcaldy A2 621 Acute (general with some teaching) (7) Queen Margaret Hospital, Dunfermline A3 196 Acute (mixed speciality) 2 acute 5 community Cameron Hospital, Leven B7 95 Small, long stay geriatric Adamson Hospital, Cupar J26 19 Community Glenrothes Hospital J26 74 Community Randolph Wemyss Memorial Hospital J26 16 Community St. -

North and West Operational Unit Occupational Therapy & Physiotherapy Leadership and Management Structure – January 2015
North and West Operational Unit Occupational Therapy & Physiotherapy Leadership and Management structure – January 2015 Within North and West Unit we have leads for both Occupational Therapy and Physiotherapy who have area wide governance roles for these professions and they link into the Highland wide governance networks for their profession. All Allied Health Professional staff are professionally led by those listed in the tables below and operationally managed via an integrated team structure within districts which sit under an area and Unit level management structure to the Director of Operations. Our only Mental Health Occupational Therapist is operationally managed in the Mental Health Integrated Team but professionally reports to the Lead Occupational Therapist within their area. Name Profession Post Base Dawn Mohun OT North Area Professional Migdale Hospital Lead Cherry Grove Bonar Bridge IV24 3ER Kerry Watson OT West Area Professional Kyle Health Centre, Lead Station Road Kyle of Lochalsh IV40 8AE Liz Morrison Physio Acting West Area Fort Willian Health Centre Professional Lead Fort William Lochaber PH33 7AQ Shona Paterson Physio North Area Professional Lawson Memorial Hospital Lead Golspie Sutherland KW10 6SS South and Mid Unit Management Structure Within South & Mid we have Unit Leads for both Occupational Therapy and Physiotherapy who have unit wide governance roles for these professions and they link into the Highland wide governance networks for their profession. Community Physiotherapy and Occupational Therapy sits within