Multi-Sectoral Rapid Assessment Report Rapport D'évaluation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bulletin Sap N°377
PRESIDENCE DE LA REPUBLIQUE REPUBLIQUE DU MALI ------------***------------ ------------***------------ COMMISSARIAT A LA SECURITE ALIMENTAIRE Un Peuple-Un But-Une Foi ------------***------------ SYSTEME D’ALERTE PRECOCE (S.A.P) BP. 2660, Bamako-Mali Tel :(223) 20 80 10 28 ; Adresse email : [email protected] /[email protected] Adresse Site Web : www.sapmali.com BULLETIN SAP N°377 Mars 2019 Présentation du Système d’Alerte Précoce (S.A.P) du MALI PRESENTATION DU SAP Le SAP est un système de collecte permanente d’informations sur la situation alimentaire. Sa mission consiste essentiellement à fournir à l’ensemble du système de sécurité alimentaire du pays les informations nécessaires à une affectation optimale du stock national de sécurité dans le cadre d'opérations d'aides alimentaires ciblées ou à une utilisation efficiente des fonds de sécurité alimentaire dans des actions d’atténuation d’insécurité alimentaire. Son objectif est de déterminer suffisamment à l'avance les populations les plus vulnérables risquant de connaître des difficultés alimentaires et/ou nutritionnelles, de dire les raisons du risque, de dire à partir de quand, pour combien de temps, avec quelle intensité et quelles sont les actions d’atténuation possibles. Les informations sont recueillies auprès des services administratifs, techniques, de la société civile et des élus locaux depuis les communes vers les chefs-lieux de cercles, les chefs-lieux de Régions et enfin Bamako. Au niveau de chaque chef-lieu de Région, l'équipe régionale SAP chargée du recueil des informations est appuyée par la Direction Régionale de la Planification, de la Statistique, de l’Informatique, de l’Aménagement du Territoire et de la Population. -

M700kv1905mlia1l-Mliadm22305
! ! ! ! ! RÉGION DE MOPTI - MALI ! Map No: MLIADM22305 ! ! 5°0'W 4°0'W ! ! 3°0'W 2°0'W 1°0'W Kondi ! 7 Kirchamba L a c F a t i Diré ! ! Tienkour M O P T I ! Lac Oro Haib Tonka ! ! Tombouctou Tindirma ! ! Saréyamou ! ! Daka T O M B O U C T O U Adiora Sonima L ! M A U R I T A N I E ! a Salakoira Kidal c Banikane N N ' T ' 0 a Kidal 0 ° g P ° 6 6 a 1 1 d j i ! Tombouctou 7 P Mony Gao Gao Niafunké ! P ! ! Gologo ! Boli ! Soumpi Koulikouro ! Bambara-Maoude Kayes ! Saraferé P Gossi ! ! ! ! Kayes Diou Ségou ! Koumaïra Bouramagan Kel Zangoye P d a Koulikoro Segou Ta n P c ! Dianka-Daga a ! Rouna ^ ! L ! Dianké Douguel ! Bamako ! ougoundo Leré ! Lac A ! Biro Sikasso Kormou ! Goue ! Sikasso P ! N'Gorkou N'Gouma ! ! ! Horewendou Bia !Sah ! Inadiatafane Koundjoum Simassi ! ! Zoumoultane-N'Gouma ! ! Baraou Kel Tadack M'Bentie ! Kora ! Tiel-Baro ! N'Daba ! ! Ambiri-Habe Bouta ! ! Djo!ndo ! Aoure Faou D O U E N T Z A ! ! ! ! Hanguirde ! Gathi-Loumo ! Oualo Kersani ! Tambeni ! Deri Yogoro ! Handane ! Modioko Dari ! Herao ! Korientzé ! Kanfa Beria G A O Fraction Sormon Youwarou ! Ourou! hama ! ! ! ! ! Guidio-Saré Tiecourare ! Tondibango Kadigui ! Bore-Maures ! Tanal ! Diona Boumbanke Y O U W A R O U ! ! ! ! Kiri Bilanto ! ! Nampala ! Banguita ! bo Sendegué Degue -Dé Hombori Seydou Daka ! o Gamni! d ! la Fraction Sanango a Kikara Na! ki ! ! Ga!na W ! ! Kelma c Go!ui a Te!ye Kadi!oure L ! Kerengo Diambara-Mouda ! Gorol-N! okara Bangou ! ! ! Dogo Gnimignama Sare Kouye ! Gafiti ! ! ! Boré Bossosso ! Ouro-Mamou ! Koby Tioguel ! Kobou Kamarama Da!llah Pringa! -
R E GION S C E R C L E COMMUNES No. Total De La Population En 2015
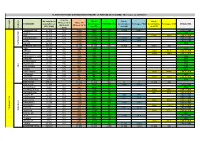
PLANIFICATION DES DISTRIBUTIONS PENDANT LA PERIODE DE SOUDURE - Mise à jour au 26/05/2015 - % du CH No. total de la Nb de Nb de Nb de Phases 3 à 5 Cibles CH COMMUNES population en bénéficiaires TONNAGE CSA bénéficiaires Tonnages PAM bénéficiaires Tonnages CICR MODALITES (Avril-Aout (Phases 3 à 5) 2015 (SAP) du CSA du PAM du CICR CERCLE REGIONS 2015) TOMBOUCTOU 67 032 12% 8 044 8 044 217 10 055 699,8 CSA + PAM ALAFIA 15 844 12% 1 901 1 901 51 CSA BER 23 273 12% 2 793 2 793 76 6 982 387,5 CSA + CICR BOUREM-INALY 14 239 12% 1 709 1 709 46 2 438 169,7 CSA + PAM LAFIA 9 514 12% 1 142 1 142 31 1 427 99,3 CSA + PAM SALAM 26 335 12% 3 160 3 160 85 CSA TOMBOUCTOU TOMBOUCTOU TOTAL 156 237 18 748 18 749 506 13 920 969 6 982 388 DIRE 24 954 10% 2 495 2 495 67 CSA ARHAM 3 459 10% 346 346 9 1 660 92,1 CSA + CICR BINGA 6 276 10% 628 628 17 2 699 149,8 CSA + CICR BOUREM SIDI AMAR 10 497 10% 1 050 1 050 28 CSA DANGHA 15 835 10% 1 584 1 584 43 CSA GARBAKOIRA 6 934 10% 693 693 19 CSA HAIBONGO 17 494 10% 1 749 1 749 47 CSA DIRE KIRCHAMBA 5 055 10% 506 506 14 CSA KONDI 3 744 10% 374 374 10 CSA SAREYAMOU 20 794 10% 2 079 2 079 56 9 149 507,8 CSA + CICR TIENKOUR 8 009 10% 801 801 22 CSA TINDIRMA 7 948 10% 795 795 21 2 782 154,4 CSA + CICR TINGUEREGUIF 3 560 10% 356 356 10 CSA DIRE TOTAL 134 559 13 456 13 456 363 0 0 16 290 904 GOUNDAM 15 444 15% 2 317 9 002 243 3 907 271,9 CSA + PAM ALZOUNOUB 5 493 15% 824 3 202 87 CSA BINTAGOUNGOU 10 200 15% 1 530 5 946 161 4 080 226,4 CSA + CICR ADARMALANE 1 172 15% 176 683 18 469 26,0 CSA + CICR DOUEKIRE 22 203 15% 3 330 -

Annuaire Statistique 2015 Du Secteur Développement Rural
MINISTERE DE L’AGRICULTURE REPUBLIQUE DU MALI ----------------- Un Peuple - Un But – Une Foi SECRETARIAT GENERAL ----------------- ----------------- CELLULE DE PLANIFICATION ET DE STATISTIQUE / SECTEUR DEVELOPPEMENT RURAL Annuaire Statistique 2015 du Secteur Développement Rural Juin 2016 1 LISTE DES TABLEAUX Tableau 1 : Répartition de la population par région selon le genre en 2015 ............................................................ 10 Tableau 2 : Population agricole par région selon le genre en 2015 ........................................................................ 10 Tableau 3 : Répartition de la Population agricole selon la situation de résidence par région en 2015 .............. 10 Tableau 4 : Répartition de la population agricole par tranche d'âge et par sexe en 2015 ................................. 11 Tableau 5 : Répartition de la population agricole par tranche d'âge et par Région en 2015 ...................................... 11 Tableau 6 : Population agricole par tranche d'âge et selon la situation de résidence en 2015 ............. 12 Tableau 7 : Pluviométrie décadaire enregistrée par station et par mois en 2015 ..................................................... 15 Tableau 8 : Pluviométrie décadaire enregistrée par station et par mois en 2015 (suite) ................................... 16 Tableau 9 : Pluviométrie enregistrée par mois 2015 ........................................................................................ 17 Tableau 10 : Pluviométrie enregistrée par station en 2015 et sa comparaison à -

0 16 32 48 64 8 Km
LOCALISATIONREGIONS REALISATIONS DE TOMBOUCTOU RELAC I & ET II / TOMBOUCTOUTAOUDENIT LOCALISATION REALISATION PROJETS RELAC I ET II Projet MLI/803 Relance de l’Economie locale et Appui aux Collectivités dans le Nord du Mali Avec la participation financière de l’UE ¯ REPUBLIQUE DU MALI SALAM C.TOMBOUCTOU BER TICHIFT DOUAYA INASTEL ELB ESBAT LYNCHA BER AIN RAHMA TINAKAWAT TAWAL C.BOUREM AGOUNI C.GOUNDAM ZARHO JIDID LIKRAKAR GABERI ATILA NIBKIT JAMAA TINTÉLOUT RHAROUS ERINTEDJEFT BER WAIKOUNGOU NANA BOUREM INALY DANGOUMA ALAFIA ALGABASTANE KEL ESSOUK TOBORAK NIKBKIT KAIDAM KEL ESSOUK ABOUA BENGUEL RHAROUS TOMBOUCTOU RHAROUS CAP ARAOUNE BOUGOUNI TINDIAMBANE TEHERDJE MINKIRI MILALA CT TOUEDNI IKOUMADEN DOUDARE BÉRÉGOUNGOU EMENEFAD HAMZAKOMA MORA TEDEYNI KEL INACHARIADJANDJINA KOIRA KABARA TERDIT NIBKITE KAIDAM ADIASSOU ARNASSEYEBELLESAO ZEINA DOUEKIRE NIBKIT KORIOME BOUREM INALY BORI KEL IKIKANE TIMBOUSE KELTIROU HOUNDOUBOMO TAGLIF INKARAN KAGA TOYA HEWA TILIMEDESS I INDALA ILOA KOULOUTAN II KELTAMOULEIT BT KEL ANTASSAR DJEGUELILA TASSAKANE IDJITANE ISSAFEYE DONGHOI TAKOUMBAOUT EDJAME ADINA KOIRA AGLAL DOUEKIRE KESSOU BIBI LAFIA NIAMBOURGOU HAMZAKONA ZINZIN 3 BOYA BABAGA AMTAGARE KATOUWA WANA KEL HARODJENE 2 FOUYA GOUNDAM DOUKOURIA KESSOU KOREY INTEDEINI EBAGAOU KEYNAEBAGAOU BERRI BORA CAMP PEUL GOYA SUD GARI KEL HAOUSSA IDJILAD KEL ERKIL ARHAM KOROMIA HARAM DIENO KEL ADRAR ARHAM KIRCHAMBA DOUKOURIA BAGADADJI GOUREIGA MORIKOIRA TANGASSANE DEBE DIAWATOU FOUTARD FADJIBAYENDE KIRCHAMBA DIAWATOU DOUTA KOUNDAR INATABANE CHÉRIF YONE KEL DJILBAROU -

Régions De SEGOU Et MOPTI République Du Mali P! !
Régions de SEGOU et MOPTI République du Mali P! ! Tin Aicha Minkiri Essakane TOMBOUCTOUC! Madiakoye o Carte de la ville de Ségou M'Bouna Bintagoungou Bourem-Inaly Adarmalane Toya ! Aglal Razelma Kel Tachaharte Hangabera Douekiré ! Hel Check Hamed Garbakoira Gargando Dangha Kanèye Kel Mahla P! Doukouria Tinguéréguif Gari Goundam Arham Kondi Kirchamba o Bourem Sidi Amar ! Lerneb ! Tienkour Chichane Ouest ! ! DiréP Berabiché Haib ! ! Peulguelgobe Daka Ali Tonka Tindirma Saréyamou Adiora Daka Salakoira Sonima Banikane ! ! Daka Fifo Tondidarou Ouro ! ! Foulanes NiafounkoéP! Tingoura ! Soumpi Bambara-Maoude Kel Hassia Saraferé Gossi ! Koumaïra ! Kanioumé Dianké ! Leré Ikawalatenes Kormou © OpenStreetMap (and) contributors, CC-BY-SA N'Gorkou N'Gouma Inadiatafane Sah ! ! Iforgas Mohamed MAURITANIE Diabata Ambiri-Habe ! Akotaf Oska Gathi-Loumo ! ! Agawelene ! ! ! ! Nourani Oullad Mellouk Guirel Boua Moussoulé ! Mame-Yadass ! Korientzé Samanko ! Fraction Lalladji P! Guidio-Saré Youwarou ! Diona ! N'Daki Tanal Gueneibé Nampala Hombori ! ! Sendegué Zoumané Banguita Kikara o ! ! Diaweli Dogo Kérengo ! P! ! Sabary Boré Nokara ! Deberé Dallah Boulel Boni Kérena Dialloubé Pétaka ! ! Rekerkaye DouentzaP! o Boumboum ! Borko Semmi Konna Togueré-Coumbé ! Dogani-Beré Dagabory ! Dianwely-Maoundé ! ! Boudjiguiré Tongo-Tongo ! Djoundjileré ! Akor ! Dioura Diamabacourou Dionki Boundou-Herou Mabrouck Kebé ! Kargue Dogofryba K12 Sokora Deh Sokolo Damada Berdosso Sampara Kendé ! Diabaly Kendié Mondoro-Habe Kobou Sougui Manaco Deguéré Guiré ! ! Kadial ! Diondori -

Geo-Epidemiology of Malaria at the Health Area Level, Dire Health District, Mali, 2013–2017
International Journal of Environmental Research and Public Health Article Geo-Epidemiology of Malaria at the Health Area Level, Dire Health District, Mali, 2013–2017 Mady Cissoko 1,2,3,* , Issaka Sagara 1,2, Moussa H. Sankaré 3, Sokhna Dieng 2, Abdoulaye Guindo 1,4, Zoumana Doumbia 3, Balam Allasseini 3, Diahara Traore 5, Seydou Fomba 5, Marc Karim Bendiane 2, Jordi Landier 2, Nadine Dessay 6 and Jean Gaudart 1,7 1 Malaria Research and Training Center—Ogobara K. Doumbo (MRTC-OKD), FMOS-FAPH, Mali-NIAID-ICER, Université des Sciences, des Techniques et des Technologies de Bamako, Bamako 1805, Mali; [email protected] (I.S.); [email protected] (A.G.); [email protected] (J.G.) 2 Aix Marseille Université (AMU), Institut national de la santé et de la recherche médicale (INSERM), Institut de Recherche pour le Développement (IRD), 13005 Marseille, France; [email protected] (S.D.); [email protected] (M.K.B.); [email protected] (J.L.) 3 Direction Régionale de la Santé de Tombouctou, Tombouctou 59, Mali; [email protected] (M.H.S.); [email protected] (Z.D.); [email protected] (B.A.) 4 Mère et Enfant face aux Infections Tropicales (MERIT), IRD, Université Paris 5, 75006 Paris, France 5 Programme National de la Lutte contre le Paludisme (PNLP Mali), Bamako 233, Mali; [email protected] (D.T.); [email protected] (S.F.) 6 ESPACE-DEV, UMR228 IRD/UM/UR/UG/UA, Institut de Recherche pour le Développement (IRD), 34093 Montpellier, France; [email protected] 7 Aix Marseille Université, APHM, INSERM, IRD, SESSTIM, Hop -

Peacebuilding Fund
Highlights #15 | April 2016 CRZPC: enlarged session with donors and Monthly Bulletin some iNGOs Trust Fund: new equipment for the MOC HQ in Gao Role of the S&R Section Peacebuilding Fund: UNDP & UNIDO support income generating activities In support to the Deputy Special Representative Through this monthly bulletin, we provide regular Timbuktu: support to the Préfecture and of the Secretary-General (DSRSG), Resident updates on stabilization & recovery developments women associations (QIPs) Coordinator (RC) and Humanitarian Coordinator (HC) and activities in the north of Mali. The intended Mopti: gardening in Sévaré prison (QIP video) in her responsibilities to lead the United Nations’ audience is the section’s main partners including Bamako: “MINUSMA in front of youths” contribution to Mali’s reconstruction efforts, the MINUSMA military and civilian components, UNCT awareness-raising day Stabilization & Recovery section (S&R) promotes and international partners. More QIPs launched in northern regions synergies between MINUSMA, the UN Country Team and other international partners. For more information: Gabriel Gelin, Information Specialist (S&R Main Figures section) - [email protected] QIPs 2015-2016: 58 projects with 15 completed and 43 under implementation over a total budget Donor Coordination and Partnerships of 4 million USD (167 projects since 2013) Peacebuilding Fund (PBF): 5 projects started On 8th of April, donors and some epidemics, (3) support to medicine provision in 2015 over 18 months for a total budget of 1. international NGOs met for the and (4) strengthening of the health information 10,932,168 USD monthly enlarged session of the Commission system. Partners in presence recommended that Trust Fund (TF): 13 projects completed/nearing Réhabilitation des Zones Post-Conflit (CRZPC). -

Et Dangha (Cercle De Diré)
Coopération Allemande (GTZ/KfW) Programme Mali-Nord Mission de prospection dans les communes de Lafia et Alafia (cercle de Tombouctou), Haribomo (cercle de Gourma Rharous) et Dangha (cercle de Diré) réunion à Temeout le 22 février 2009 présenté par Yehia Ag Mohamed Ali Bamako, mars 2009 1 1. Introduction Une mission du Programme Mali-Nord (GTZ/KfW) s’est rendue dans les communes de Lafia (cercle de Tombouctou) et de Dangha (cercle de Diré) du 21 au 22 février 2009, La mission est composée de : - Nock Ag Attia (comité consultatif), - Yehia Ag Mohamed Ali, - Dr. Henner Papendieck, - Salaha Baby (chef d’antenne de Diré), - Boubacar Maïga (chef d’antenne de Rharous), - Aliou Maouloud (aménagiste). 2. Objectifs de la mission Cette mission complète la prospection commencée lors de la mission du 13 au 16 janvier 2009. Elle est destinée à évaluer le potentiel aménageable des zones visitées et à prendre contact avec les élus et notables locaux en vue d’identifier des personnes ressources crédibles pouvant garantir la réussite d’un éventuel programme d’aménagement de PIV et mares. 3. Déroulement de la mission Le 21 février la mission a emprunté la pinasse à partir de Koriomé pour longer le fleuve en direction de Kaga. Elle s’est arrêtée à Ewet (en face de Tombouctou) où elle a rencontré les notables de la fraction Kel Ahadsatafane. Là, les populations ont manifesté leur intérêt pour l’aménagement de 3 PIV de 40 hectares chacun, soit 120 hectares, PIV aménagés par différentes organisations : FENU, AFAR, UNICEF, etc. Le potentiel aménageable est apparemment suffisant. -

Mali, Third Quarter 2018: Update on Incidents According to the Armed
MALI, THIRD QUARTER 2018: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) - Updated 2nd edition compiled by ACCORD, 20 December 2018 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; incid- ent data: ACLED, 15 December 2018; coastlines and inland waters: Smith and Wessel, 1 May 2015 MALI, THIRD QUARTER 2018: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) - UPDATED 2ND EDITION COMPILED BY ACCORD, 20 DECEMBER 2018 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Violence against civilians 63 37 208 Conflict incidents by category 2 Strategic developments 37 0 0 Development of conflict incidents from September 2016 to September Battles 36 25 159 2018 2 Remote violence 29 10 35 Methodology 3 Riots/protests 26 0 0 Total 191 72 402 Conflict incidents per province 4 This table is based on data from ACLED (datasets used: ACLED, 15 December 2018). Localization of conflict incidents 4 Development of conflict incidents from September 2016 to Disclaimer 5 September 2018 This graph is based on data from ACLED (datasets used: ACLED, 15 December 2018). 2 MALI, THIRD QUARTER 2018: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) - UPDATED 2ND EDITION COMPILED BY ACCORD, 20 DECEMBER 2018 Methodology Geographic map data is primarily based on GADM, complemented with other sources if necessary. -

Gao, Kidal, Tombouctou | 27 Décembre 2012
ANALYSE DES DONNEES SECONDAIRES Nord Mali: Gao, Kidal, Tombouctou | 27 décembre 2012 FACTEURS DE LA CRISE PROFIL HUMANITAIRE Quoi: Conflit armé au nord Mali Chiffres Globaux (Nord et Sud) Quand: De mi-janvier 2012 à nos jours Population Déplacements Sécurité Alimentaire Acteurs principaux: Les forces gouvernementales, les milices pro-gouvernementales, les groupes armés: Mouvement national de libération de l’Azawad – MNLA; Ansar Dine; Al Qaïda au Maghreb Islamique (AQIM); MUJUAO Mali A risque d’insécurité Facteurs aggravants: Total des PDIs au Mali: 14.53 millions* alimentaire Insécurité continue: Les tensions, les liens avec le crime organisé et les intérêts 198,558*** divergents conduisent à la fragmentation et aux conflits entre les groupes armés (Voir 2 millions** page 3 – protection) Réfugiés maliens Personnes ayant un besoin Insécurité alimentaire (voir page 2 – sécurité alimentaire) et les niveaux élevés de dans la région**** immédiat d’assistance malnutrition (page 5 – nutrition) 145,599 alimentaire Ralentissement de l’activité économique Accès limité et/ou manque d’accès aux services sociaux de base. 747,000 Processus politique: Impasse après le coup d’état contre l’ancien Président Amadou Chiffres pour le Nord Toumani Toure entrainant une instabilité politique. Population Déplacements Sécurité Alimentaire Analyse préliminaire des facteurs essentiels du besoin humanitaire: La crise alimentaire et nutritionnelle prolongée, affectant les 3 régions Nord sous contrôle des groupes armés, aura probablement moins d’impact immédiat sur les conditions de Nord PDIs au Nord Mali santé de la population globale, que l’insécurité, la perturbation des services publics et du A risque d’insécurité 921,393** 76,386*** alimentaire commerce et la fuite du personnel de santé et des administrations, aggravés par (Tombouctou, Gao, Kidal) l’application d’une interprétation stricte de la sharia et l’accès restreint de l’assistance 1 million** humanitaire. -

Pnr 2015 Plan Distribution De
Tableau de Compilation des interventions Semences Vivrières mise à jour du 03 juin 2015 Total semences (t) Total semences (t) No. total de la Total ménages Total Semences (t) Total ménages Total semences (t) COMMUNES population en Save The Save The CERCLE CICR CICR FAO REGIONS 2015 (SAP) FAO Children Children TOMBOUCTOU 67 032 ALAFIA 15 844 BER 23 273 1 164 23,28 BOUREM-INALY 14 239 1 168 23,36 LAFIA 9 514 854 17,08 TOMBOUCTOU SALAM 26 335 TOMBOUCTOU TOTAL 156 237 DIRE 24 954 688 20,3 ARHAM 3 459 277 5,54 BINGA 6 276 450 9 BOUREM SIDI AMAR 10 497 DANGHA 15 835 437 13 GARBAKOIRA 6 934 HAIBONGO 17 494 482 3,1 DIRE KIRCHAMBA 5 055 KONDI 3 744 SAREYAMOU 20 794 1 510 30,2 574 3,3 TIENKOUR 8 009 TINDIRMA 7 948 397 7,94 TINGUEREGUIF 3 560 DIRE TOTAL 134 559 GOUNDAM 15 444 ALZOUNOUB 5 493 BINTAGOUNGOU 10 200 680 6,8 ADARMALANE 1 172 78 0,78 DOUEKIRE 22 203 DOUKOURIA 3 393 ESSAKANE 13 937 929 9,29 GARGANDO 10 457 ISSA BERY 5 063 338 3,38 TOMBOUCTOU KANEYE 2 861 GOUNDAM M'BOUNA 4 701 313 3,13 RAZ-EL-MA 5 397 TELE 7 271 TILEMSI 9 070 TIN AICHA 3 653 244 2,44 TONKA 65 372 190 4,2 GOUNDAM TOTAL 185 687 RHAROUS 32 255 1496 18,7 GOURMA-RHAROUS TOMBOUCTOU BAMBARA MAOUDE 20 228 1 011 10,11 933 4,6 BANIKANE 11 594 GOSSI 29 529 1 476 14,76 HANZAKOMA 11 146 517 6,5 HARIBOMO 9 045 603 7,84 419 12,2 INADIATAFANE 4 365 OUINERDEN 7 486 GOURMA-RHAROUS SERERE 10 594 491 9,6 TOTAL G.