Coronary Artery Bypass Graft Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
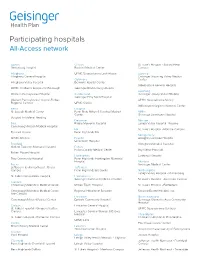
Participating Hospitals All-Access Network
Participating hospitals All-Access network Adams Clinton St. Luke’s Hospital - Sacred Heart Gettysburg Hospital Bucktail Medical Center Campus Allegheny UPMC Susquehanna Lock Haven Luzerne Allegheny General Hospital Geisinger Wyoming Valley Medical Columbia Center Allegheny Valley Hospital Berwick Hospital Center Wilkes-Barre General Hospital UPMC Children’s Hospital of Pittsburgh Geisinger Bloomsburg Hospital Lycoming Western Pennsylvania Hospital Cumberland Geisinger Jersey Shore Hospital Geisinger Holy Spirit Hospital Western Pennsylvania Hospital-Forbes UPMC Susquehanna Muncy Regional Campus UPMC Carlisle Williamsport Regional Medical Center Berks Dauphin St. Joseph Medical Center Penn State Milton S Hershey Medical Mifflin Center Geisinger Lewistown Hospital Surgical Institute of Reading Delaware Monroe Blair Riddle Memorial Hospital Lehigh Valley Hospital - Pocono Conemaugh Nason Medical Hospital Elk St. Luke’s Hospital - Monroe Campus Tyrone Hospital Penn Highlands Elk Montgomery UPMC Altoona Fayette Abington Lansdale Hospital Uniontown Hospital Bradford Abington Memorial Hospital Guthrie Towanda Memorial Hospital Fulton Fulton County Medical Center Bryn Mawr Hospital Robert Packer Hospital Huntingdon Lankenau Hospital Troy Community Hospital Penn Highlands Huntingdon Memorial Hospital Montour Bucks Geisinger Medical Center Jefferson Health Northeast - Bucks Jefferson Campus Penn Highlands Brookville Northampton Lehigh Valley Hospital - Muhlenberg St. Luke's Quakertown Hospital Lackawanna Geisinger Community Medical Center St. Luke’s Hospital - Anderson Campus Cambria Conemaugh Memorial Medical Center Moses Taylor Hospital St. Luke’s Hospital - Bethlehem Conemaugh Memorial Medical Center - Regional Hospital of Scranton Steward Easton Hospital, Inc. Lee Campus Lancaster Northumberland Conemaugh Miners Medical Center Ephrata Community Hospital Geisinger Shamokin Area Community Hospital Carbon Lancaster General Hospital St. Luke’s Hospital - Gnaden Huetten UPMC Susquehanna Sunbury Campus Lancaster General Women & Babies Hospital Philadelphia St. -

Designated Acute Care Hospital Stroke Centers 180424
Acute Stroke -ready; Comprehensive stroke COUNTY FACILITY NAME CITY ZIP Center or Primary Stroke Center? MONTGOMERY Abington Memorial Hospital Comprehensive stroke Center Abington 19001 ALLEGHENY Allegheny General Hospital Comprehensive Stroke Center Pittsburgh 15212 CUMBERLAND Carlisle Regional Medical Center Primary Stroke Center Carlisle 17015 FRANKLIN Chambersburg Hospital Primary Stroke Center Chambersburg 17201 CHESTER Chester County Hospital – Chester County Primary Stroke Center West Chester 19380 CAMBRIA Conemaugh Memorial Medical Center Primary Stroke Center Johnstown 15905 BLAIR Conemaugh Nason Medical Center Acute Stroke -ready Roaring Spring 16673 BUCKS Doylestown Hospital Primary Stroke Center Doylestown 18901 MONTGOMERY Einstein Medical Center Montgomery Primary Stroke Center East Norriton 19403 LANCASTER Ephrata Community Hospital Primary Stroke Center Ephrata 17522 WESTMORELAND Excela Health Frick Hospital Primary Stroke Center Westmoreland 15666 WESTMORELAND Excela Health Latrobe Hospital Primary Stroke Center Latrobe 15650 WESTMORELAND Excela Health Westmoreland Hospital Primary Stroke Center Greensburg 15601 LACKAWANNA Geisinger Community Medical Center – Scranton - Lackawanna County Primary Stroke Center Scranton 18510 MONTOUR Geisinger Medical Center – Montour County Primary Stroke Center Danville 17822 LUZERNE Geisinger Wyoming Valley Medical Center, Wilkes-Barre – Luzerne County Primary Stroke Center Wilkes Barre 18711 ADAMS Gettysburg Hospital Primary Stroke Center Gettysburg 17325 CARBON Gnadden Huetten Memorial -

Allergy/Immunology Long Island Jewish Medical Center Thomas
Einstein Medical Center Internal Medicine Residency Fellowship Appointments 1999-present (Updated 12-12-2019, some advanced fellowships included) Allergy/Immunology Long Island Jewish Medical Center Thomas Jefferson University University of Pennsylvania Cardiology Einstein Medical Center (29) Allegheny General Hospital Baylor College of Medicine (5) Baystate Medical Center Cedars Sinai Medical Center Cleveland Clinic, Florida Creighton University Danbury Hospital Drexel University/ Hahnemann Hospital Emory University (8) Geisinger Medical Center (3) Jersey Shore University Medical Center Lankenau Medical Center (2) Lehigh Valley Hospital (2) Loma Linda University Hospital (4) Michigan State University Ochsner Clinic Foundation St. Luke's Hospital, Bethlehem St Vincent’s Hospital, Worcester, MA Tufts Medical Center UMDNJ Robert Wood Johnson, Camden UMDNJ-SOM University of Arkansas University of Buffalo University of California at Davis University of Cincinnati University of Florida University of Illinois at Chicago (2) University of Kentucky University of Miami Jackson Memorial University of Minnesota University of Pittsburgh University of Texas, Galveston University of Texas, Houston (2) Virginia Commonwealth University Critical Care University of Pittsburgh Medical Center University of Tennessee Endocrinology Einstein Medical Center (3) Baylor College of Medicine (2) Case Western University Cedars Sinai Medical Center Cooper University Hospital Johns Hopkins University Mt Sinai Medical Center, NY St Luke’s Roosevelt Stony Brook University -

Coverage You Can Count on We’Ll Help You Every Step of the Way
GEISINGER HEALTH PLAN Coverage you can count on We’ll help you every step of the way. Call us 800-918-5154 to speak to our dedicated team of trained advisors. Open Enrollment Period: Nov. 1, 2020, through Jan. 15, 2021 Hours: Monday–Friday, 8 a.m. to 7 p.m.; Saturday, 10 a.m. to 2 p.m. Jan. 16, 2021, through Oct. 31, 2021 Hours: Monday–Friday, 8 a.m. to 5 p.m. Due to COVID-19 restrictions, Geisinger Community Place will be closed until further notice. Open enrollment begins Nov. 1. Are you ready? For plan year 2021, Pennsylvania is transitioning from HealthCare.gov to its own state-based health insurance marketplace, Pennie™, where you will enroll in or make changes to your 2021 coverage. The 2021 Open Enrollment Period (OEP) begins Nov. 1, 2020, and lasts until Jan. 15, 2021. • Nov. 1–Dec. 15, 2020 enrollment: Coverage becomes effective Jan. 1, 2021 Pennie will be live at the • Dec. 16, 2020–Jan. 15, 2021 enrollment: Coverage becomes effective Feb. 1, 2021 beginning of the 2021 OEP. Visit pennie.com or call Are you in our service area? 844-844-8040 to find Geisinger Health Plan's service area includes the following counties: information and assistance • Adams • Cumberland • Luzerne • Somerset on your health insurance. • Berks • Dauphin • Lycoming • Snyder • Blair • Elk • Mifflin • Sullivan • Bradford • Fulton • Monroe • Susquehanna • Cambria • Huntingdon • Montour • Tioga • Cameron • Jefferson • Northumberland • Union • Carbon • Juniata • Northampton • Wayne • Centre • Lackawanna • Perry • Wyoming • Clearfield • Lancaster • Pike • York • Clinton • Lebanon • Potter • Columbia • Lehigh • Schuylkill County restrictions for Premier network plans and Geisinger Extra plans can be found on pages 6 and 7 respectively. -

Acute-Care-Hospitals-Alphabetic.Pdf
Acute Care Hospitals Facility Name Facility # Facility Name Facility # Abington Health Center - Warminster 1410-09 Barnabas Health Jersey City Medical Center 2312-70 Campus(Warminster Hospital) Barnes-Kasson Hospital 1241-58 Abington Health-Lansdale Hospital 1432-46 Barnesville Hospital - Barnesville 1012-72 Abington Memorial Hospital 1001-46 Bath VA Medical Center 1062-71 Acuity Specialty Hospital of New Jersey (LTAC) 2310-70 (within Atlanticare Reg. Med.Ctr. Atlantic City Bayhealth Hospital, Sussex Campus 1012-68 Campu Bayshore Community Hospital 1039-70 AHN Harmar Neighborhood Hospital 1465-02 Beebe Medical Center - Lewes, DE 1003-68 AHN Hempfield Neighborhood Hospital 1130-65 Bellevue Hospital Center- New York, NY 1012-71 AHN McCandless Neighborhood Hospital 1464-02 Belmont Community Hospital (The Bellaire City 1002-72 AHN Neighborhood Hospital - Brentwood 1463-02 Hospital) Akron General Medical Center 1033-72 Belmont Hospital Bel Air 1026-72 Albany Medical Center Hospital - Albany, NY 1043-71 Benedictine Hospital 1001-71 Aliquippa Community Hospital (UPMC Beaver 1002-04 Berwick Hospital Center 1013-19 Valley Hospital) Beth Israel Hospital - Newark 1035-70 Allegheny General Hospital 1184-02 Beth Israel Med Ctr-Petrie Division (Manhattan) 1057-71 Allegheny Valley Hospital (Alle-Kiski Medical 1124-02 Center) Bloomsburg Hospital 1016-19 Anne Arundel Medical Center 1035-69 Bluefield Regional Medical Center 1029-73 Ardern Hill Hospital - Goshen 1017-71 Blythedale Children's Hospital 1063-71 Aria Health - Bucks County (formerly Delaware -

PA Ehealth Partnership P3N ADT Operations Facilities in Production
PA eHealth Partnership P3N ADT Operations Facilities in Production Exchange ER Name Type of Facility Subtype - ED, Inpatient, etc. Consent Model Address HSX Mainline Health Bryn Mawr Hospital hospital ED Opt Out 130 South Bryn Mawr Avenue, Bryn Mawr, PA 19010 HSX Mainline Health Lankenau Hospital hospital ED Opt Out 100 Lancaster Avenue, Wynnewood, PA 19096 HSX Mainline Health Paoli Hospital hospital ED Opt Out 255 W. Lancaster Avenue, Paoli, PA 19301 HSX Mainline Health Riddle Hospital hospital ED Opt Out 1068 West Baltimore Pike, Media, PA 19063 HSX Temple University Hospital hospital ED Opt Out 3401 N.Broad Street,Philadelphia, PA 19140 HSX Temple Jeanes Hospital hospital ED Opt Out 7600 Central Avenue, Philadelphia,PA 19111 HSX Crozer-Chester Medical Center hospital ED Opt out 1 Medical Center Blvd, Chester, PA 19013 HSX Crozer Delaware County Memorial Hospital hospital ED Opt out 501 N Lansdowne Ave, Drexel Hill, PA 19026 HSX Crozer Springfield Hospital hospital ED Opt out 190 W Sproul Rd, Springfield, PA 19064 HSX Crozer Taylor Hospital hospital ED Opt out 175 E Chester Pike, Ridley Park, PA 19078 HSX Doylestown Hospital hospital ED Opt out 595 West State Street, Doylestown, PA 18901 HSX Einstein Medical Center Elkins Park hospital ED Opt out 60 Township Line Rd, Elkins Park, PA 19027 HSX Einstein Medical Center Montgomery hospital ED Opt out 559 W Germantown Pike, East Norriton, PA 19403 HSX Einstein Medical Center Philadelphia hospital ED Opt out 5501 Old York Rd, Philadelphia, PA 19141 HSX Holy Redeemer Hospital hospital ED Opt Out 1648 Huntingdon Pike, Meadowbrook, PA 19046 HSX Mercy Fitzgerald Hospital hospital ED Opt Out 1500 Lansdowne Avenue, Darby, PA 19023 HSX Mercy Nazareth Hospital hospital ED Opt Out 2601 Holme Avenue, Philadelphia, PA 19152 HSX Mercy Philadelphia Hospital hospital ED Opt Out 501 South 54th Street, Philadelphia, PA 19143 HSX St. -
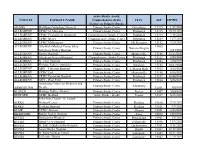
Ready; Comprehensive Stroke Center
Acute Stroke -ready; COUNTY FACILITY NAME Comprehensive stroke CITY ZIP EXPIRES Center; or Primary Stroke ADAMS WellSpan Gettysburg Hospital Primary Stroke Center Gettysburg 17325 1/22/2024 ALLEGHENY UPMC St. Margaret Primary Stroke Center Pittsburgh 15215 10/20/2022 ALLEGHENY UPMC Presbyterian Shadyside Comprehensive Stroke Center Pittsburgh 15213 7/18/2021 ALLEGHENY UPMC Mercy Comprehensive Stroke Center Pittsburgh 15219 12/7/2021 ALLEGHENY UPMC McKeesport Primary Stroke Center Mc Keesport 15132 7/20/2021 ALLEGHENY Alle-Kiski Medical Center d/b/a/ 15065 Primary Stroke Center Natrona Heights Allegheny Valley Hospital 3/14/2021 ALLEGHENY Forbes Hospital Primary Stroke Center Monroeville 15146 11/17/2022 ALLEGHENY Allegheny General Hospital Comprehensive Stroke Center Pittsburgh 15212 3/20/2021 ALLEGHENY St. Clair Hospital Primary Stroke Center Pittsburgh 15243 2/24/2023 ALLEGHENY Heritage Valley - Swickley Primary Stroke Center Swickley 15143 10/17/2021 ALLEGHENY AHN - Jefferson Hospital Primary Stroke Center Jefferson Hills 15025 3/13/2023 ALLEGHENY UPMC East Primary Stroke Center Monroeville 15146 6/16/2023 ALLEGHENY UPMC Passavant Hospital Primary Stroke Center Pittsburgh 15237 10/28/2022 ALLEGHENY AHN - West Penn Primary Stroke Center Pittsburgh 15224 5/26/2021 Armstrong Center for Medicine and Primary Stroke Center Kittanning ARMSTRONG Health 16201 3/8/2022 BEAVER Heritage Valley - Beaver Primary Stroke Center Beaver 15009 10/4/2021 BEDFORD UPMC Bedford Acute Stroke - Ready Everett 15537 6/25/2021 Penn State Health - St. Joseph BERKS Medical Center Primary Stroke Center Reading 19610 7/24/2022 BERKS Reading Hospital Primary Stroke Center Reading 19611 9/9/2021 BLAIR UPMC Altoona Primary Stroke Center Altoona 16601 5/15/2023 BRADFORD Robert Packer Hospital Primary Stroke Center Sayre 18840 12/5/2022 BUCKS Doylestown Hospital Primary Stroke Center Doylestown 18901 3/5/2021 BUCKS Grand View Hospital Primary Stroke Center Sellersville 18960 11/4/2022 BUCKS St. -

Hospital Health System
2021 Donate Life Hospital Challege Gift of Life Donor Program Hospital Registrants (64 as of 1-25-21) HOSPITAL HEALTH SYSTEM OPO REPRESENTATIVE OPO REP EMAIL Delaware County Memorial Hospital Crozer Health Joe Paparo [email protected] Taylor Hospital Crozer Health Joe Paparo [email protected] Crozer Chester Medical Center Crozer Health Joe Paparo [email protected] WellSpan Ephrata Community Hospital Wellspan Kelly Edwards [email protected] Hospital of the University of Pennsylvania Penn Medicine Greg Marino [email protected] Riddle Hospital Main Line Health System Debbie Cotellese [email protected] WellSpan Gettysburg Hospital Wellspan Karen Bronchella [email protected] Temple University Hospital Temple Christopher Schimpf [email protected] Wilkes barre general hospital Commonwealth Health Jacki Giuffrida [email protected] Roxborough Memorial Hospital Prime Health Joe Paparo [email protected] Lower Bucks Hospital Prime Health Denise Cirio [email protected] Regional Hospital of Scranton Commonwealth Health Jacki Giuffrida [email protected] Moses Taylor Hospital Commonwealth Health Jacki Giuffrida [email protected] UPMC Pinnacle West Shore UPMC Karen Bronchella [email protected] UPMC Pinnacle Community Osteopathic UPMC Karen Bronchella [email protected] UPMC Pinnacle Harrisburg UPMC Karen Bronchella [email protected] UPMC Carlisle UPMC Karen Bronchella [email protected] UPMC Hanover UPMC Karen Bronchella [email protected] St. Mary Medical Center Trinity Health Denise Cirio [email protected] UPMC Lititz UPMC Karen Bronchella [email protected] Pottstown Hospital Tower Health Debbie Cotellese [email protected] St. Luke's Monroe Campus St. Luke’s Health Network Maria Bleil [email protected] Suburban Community Hospital Prime Health Tameka Childs-Wolfe [email protected] Geisinger Medical Center Geisinger Alayne Rosner [email protected] Mount Nittany Medical Center Alayne Rosner [email protected] Corporal Michael J. -

Internship and Residency Matches Class of 2011
Internship and Residency Matches Class of 2011 Match Type Specialty Site, City and State Allopathic Internship Traditional Rotating Allegheny General Hospital Pittsburgh, PA 1 Medical College of Georgia Augusta, GA 1 Summa Health System Akron, OH 1 University of Florida Collegeof Medicine Jacksonville, FL 2 University of North Dakota Grand Forks, ND 1 Transitional Year Henry Ford Health System Detroit, MI 1 New Hanover Regional Medical Center Wilmington, NC 1 St. Elizabeth Health Center Youngstown, OH 1 Allopathic Residency Anesthesiology Albany Medical Center Albany, NY 1 Cleveland Clinic Foundation Avon, OH 1 Dallas Southwest Medical Ctr Dallas, TX 1 Hershey Medical Center Hershey, PA 1 Jackson Memorial Hospital Miami, FL 2 Loyola University Maywood, IL 1 Shands Hosp., U of Florida Gainesville, FL 1 UPMC Education Program Pittsburg, PA 2 Emergency Medicine Akron General Medical Center Akron, OH 2 Albert Einstein Medical Center Philadelphia, PA 1 Baystate Medical Center Springfield, MA 2 Detroit Receiving Hospital Detroit, MI 1 Florida Hospital East Orlando Orlando, FL 1 Hershey Medical Center Hershey, PA 1 John Peter Smith Hospital Fort Worth, TX 1 Michigan State University Kalamazoo, MI 2 Summa Health System Akron, OH 1 Texas A&M - Scott-White Temple, TX 1 University of Illinois Collegeof Medicine-Peoria Peoria, IL 1 University of Iowa Hospitals and Clinics Iowa City, IA 1 York Hospital York, PA 3 Family Medicine Bayfront Medical Center St. Petersburg, FL 1 Broward General Medical Center Fort Lauderdale, FL 1 Community Hospitals Indianapolis, -

Accredited Primary Stroke Centers
Accredited Primary Stroke Centers County Facility Name City Zip Montgomery Abington Memorial Hospital Abington 19001 Armstrong ACMH – Armstrong County Kittanning 16201 Philadelphia Albert Einstein Med. Center Philadelphia 19141 Allegheny Allegheny General Hospital Pittsburgh 15212 Bucks Aria Health – Bucks County Campus – Bucks County Langhorne 19047 Philadelphia Aria Health – Frankford Campus – Philadelphia County Philadelphia 19124 Philadelphia Aria Health – Torresdale Campus – Philadelphia County Philadelphia 19114 Chester Brandywine Hospital Coatesville 19320 Mercer Co., NJ Capital Health Medical Center – Hopewell New Jersey – Mercer Co., New Jersey Pennington NJ 8534 Mercer Co., NJ Capital Health Regional Medical Center – Trenton New Jersey – Mercer Co., NJ Trenton NJ 8638 Franklin Chambersburg Hospital Chambersburg 17201 Chester Chester County Hospital – Chester County West Chester 19380 Philadelphia Chestnut Hill Hospital Philadelphia 19118 Cambria Conemaugh Memorial Medical Center Johnstown 15905 Delaware Crozer Chester Medical Center, Taylor Ridley Park 19078 Delaware Crozer Chester Medical Center, Upland Upland 19013 Delaware Delaware County Memorial Hospital Drexel Hill 19026 Bucks Doylestown Hospital Doylestown 18901 Northampton Easton Hospital Easton 18042 Montgomery Einstein Medical Center Montgomery East Norriton 19403 Lancaster Ephrata Community Hospital Ephrata 17522 Union Evangelical Community Hospital Lewisburg 17837 Allegheny Forbes Hospital Monroeville 15146 Lackawanna Geisinger Community Medical Center – Scranton -
Maternal Mortality
Overview of the PA PQC July 26, 2019 © 2019 JHF, PRHI, HCF, & WHAMglobal 1 Perinatal Quality Collaboratives (PQCs) PQCs are networks of teams working to identify processes that need to be improved and quickly adopt best practices to achieve collective aims © 2019 JHF, PRHI, HCF, & WHAMglobal 2 PA PQC Aims Reduce maternal mortality and morbidity Improve Identification of and Care for Pregnant and Postpartum Women with Opioid Use Disorders (OUD) Improve Identification of and Care for Opioid-Exposed Newborns (OEN) © 2019 JHF, PRHI, HCF, & WHAMglobal 3 The PA PQC is designed to help birth sites and NICUs drive improvement and adopt standards of care towards the three aims © 2019 JHF, PRHI, HCF, & WHAMglobal 4 PA PQC is Leveraging Statewide Efforts Coordinates with DOH’s, DHS’, and DDAP’s Multi-Disciplinary Workgroup on Infants with Substance Exposure (MDWISE) to disseminate guidelines (e.g., Plans of Safe Care) Serves as an action arm of the PA DOH Maternal Mortality Review Committee (MMRC) PA PA MMRC PQC © 2019 JHF, PRHI, HCF, & WHAMglobal 5 Jewish Healthcare Foundation (JHF) JHF and its operating arms, including WHAMglobal, are helping to standup, administer, and facilitate the PA PQC © 2019 JHF, PRHI, HCF, & WHAMglobal 6 The NEPaPQC is Part of the PA PQC © 2019 JHF, PRHI, HCF, & WHAMglobal 7 Roles of Birth Sites / NICUs Form a multi-disciplinary quality improvement team with maternity and neonatal providers and staff at your site and outpatient clinics Participate in in-person, one-day Learning Collaborative sessions with continuing -

Pennsylvania Stroke Centers As of 8/11/2017
Pennsylvania Stroke Centers as of 8/11/2017 FACILITY NAME Acute Stroke -ready; CITY ZIP Comprehensive stroke Center or Primary Stroke COUNTY Center? Montgomery Abington Memorial Hospital Primary Stroke Center Abington 19001 Armstrong ACMH – Armstrong County Primary Stroke Center Kittanning 16201 Philadelphia Albert Einstein Med. Center Primary Stroke Center Philadelphia 19141 Allegheny Allegheny General Hospital Primary Stroke Center Pittsburgh 15212 Bucks Aria Health – Bucks County Campus – Bucks County Primary Stroke Center Langhorne 19047 Philadelphia Aria Health – Frankford Campus – Philadelphia County Primary Stroke Center Philadelphia 19124 Philadelphia Aria Health – Torresdale Campus – Philadelphia County Primary Stroke Center Philadelphia 19114 Chester Brandywine Hospital Primary Stroke Center Coatesville 19320 Cumberland Carlisle Regional Medical Center Primary Stroke Center Carlisle 17015 Franklin Chambersburg Hospital Primary Stroke Center Chambersburg 17201 Chester Chester County Hospital – Chester County Primary Stroke Center West Chester 19380 Philadelphia Chestnut Hill Hospital Primary Stroke Center Philadelphia 19118 Cambria Conemaugh Memorial Medical Center Primary Stroke Center Johnstown 15905 Delaware Crozer Chester Medical Center, Taylor Primary Stroke Center Ridley Park 19078 Delaware Crozer Chester Medical Center, Upland Primary Stroke Center Upland 19013 Delaware Delaware County Memorial Hospital Primary Stroke Center Drexel Hill 19026 Bucks Doylestown Hospital Primary Stroke Center Doylestown 18901 Northampton