The MA Gambling Impact Cohort: Transitions Across Four Waves
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The War in the Bronx
THE WAR IN THE BRONX J?SYOHOLOGISTS ray that in ordinary theless, much of the basic inaterial taught to life me use only 25% of our mental non-commissioned reserves in the Brons is cilpacities. The Waves and the Spar8 learn similar to that which a Hunter officer candi- t,o use at least SO%." This is the way the date at Smith College would learn. N;~v;ll Training School of the women's Re- For 1Pha.t Jobs Are Thsg Training? servr at the Bronx Buildings of Hunter Col- lege describes the improved mental activity The Training School at tlie Brons is \\.hat which naval training brings to the American is known as a "boot school," that is one women who go through its indoctrination. which offers preliminary indoctrination and classifies students according to the jobs for A tight-packed, concentrated, six week' which they are most suited. Specific train- coarse. leaves recruits "amazed at their pow- ing for these classifications (called ratings,! ers of retention and digestion of facts," in is acquired in a specialist's school after t.he words of the Public Relations Division. graduation from the "boot school." For es- Alid this combined with a vigorous physical ample, if after completing h'er course nt Hun- clductlt.ion program turns out women both ter she wishes to become a Raclio 3Ian. tlie pl~ysicallyfit and mentally receptive for spe- Apprentice Seaman Wave or Spar goes on ciitlizecl training to release a man for active to the Xavy radio training scliool at 3Iadison. duty. That the Hunter College campus in Wisconsin, to work for t.he official rating of tlie Bronx sllould be the scene of this trans- Radio >Ian. -

Women Ashore: the Contribution of WAVES to US Naval Science and Technology in World War II
Women Ashore: The Contribution of WAVES to US Naval Science and Technology in World War II Kathleen Broome Williams On 30 July 1947, US Navy (USN) women celebrated their fifth anniversary as WAVES: Women Accepted for Volunteer Emergency Se rv ice. In ceremonies across the count ry, flags snapped and crisp young women saluted. Congratulatory messages arrived from navy brass around the globe. The Commander-in-Chief (C-in-C) of the Atlantic Fleet, Admiral William H.P. Blandy, noted (perhaps too optimistically) that "the splendid serv ices rendered by the WAVES...and their uncomplaining spirit of sacrifice and devotion to duty at all times" would never be forgotten by "a grateful navy."' Admiral Louis E. Denfeld, C-in-C Pacific, wrote more perceptively that "the vital role" played by the WAVES "in the defeat of the Axis nations is known to all and, though often unsung in peacetime, their importance has not decreased." Significantly, Admiral Denfeld added that he would welcome the addition of the WAVES "to the Regular Naval Establishment," an issue then hanging in the balance.' Indeed, for all the anniversary praise, the WAVES' contribution to wartime successes did not even guarantee them a permanent place in the navy once peace returned nor, until recently, has their "vital role" in the Allied victory received much scholarly attention. This article helps to round out the historical record by briefly surveying one aspect of the role of the WAVES: their contribution to naval science and technology. The navy has always been a technical service but World War II was the first truly technological war. -

Waves of Modern Terrorism: Examining the Past and Predicting the Future
WAVES OF MODERN TERRORISM: EXAMINING THE PAST AND PREDICTING THE FUTURE A Thesis submitted to the Faculty of The School of Continuing Studies and of The Graduate School of Arts and Sciences in partial fulfillment of the requirements for the degree of Master of Arts in Liberal Studies By Erin Walls, B.A. Georgetown University Washington, D.C. April 5, 2017 WAVES OF MODERN TERRORISM: EXAMINING THE PAST AND PREDICTING THE FUTURE Erin Walls, B.A. Mentor: Joseph Smaldone, Ph.D. ABSTRACT David C. Rapoport’s “The Four Waves of Modern Terrorism,” is one of the most influential and widely debated theories in the field of terrorism studies. Following the terrorist attacks in the United States on September 11, 2001, Rapoport created his theoretical framework for modern terrorism by grouping previously indistinguishable patterns of political violence into four distinct waves, each lasting a generation and inspired by ideologies derived from anarchism, anti-colonialism, socialism, and religious fundamentalism. Since 1979 the world has existed within the fourth “Religious” wave that will dissipate by 2025 if the generational life cycle remains constant. Rapoport’s model will serve as the foundational source for this thesis. It will discuss the importance of the wave model and how it can be useful in counterterrorism efforts. Rapoport argues that academics and governments unduly focus on specific organizations and contemporary events, which make us less sensitive to generational patterns. Individual terrorist organizations will have specific defining features but understanding overarching global and generational patterns in real time can help shape thinking on the most effective ways to combat terrorism. -

World War II
CONFIDENCE AND CRISES, 1920-1948 World War II Resource: Life Story: Grace Brewster Murray Hopper (1906-1992) Grace Hopper’s graduation from Midshipman’s School, 1944 Grace Hopper upon graduation from Midshipman’s School, June 27, 1944. Grace Murray Hopper Collection, Archives Center, National Museum of American History, Smithsonian Institution. © Women and the American Story 2021 Page 1 of 10 CONFIDENCE AND CRISES, 1920-1948 World War II The First “Computer Bug” The First “Computer Bug”, September 9, 1945. Courtesy of the Naval Surface Warfare Center, Dahlgren, VA., 1988. U.S. Naval History and Heritage Command Photograph. © Women and the American Story 2021 Page 2 of 10 CONFIDENCE AND CRISES, 1920-1948 World War II Commodore Grace M. Hopper, USNR Official portrait photograph of Commodore Grace M. Hopper, USNR, January 20, 1984. U.S. Naval History and Heritage Command Photograph. © Women and the American Story 2021 Page 3 of 10 CONFIDENCE AND CRISES, 1920-1948 World War II Grace Hopper was born on December 9, 1906 in New York City. She was the first of her parents’ three children. Grace was fortunate to grow up in a wealthy family that highly valued education. Her father, Walter Fletcher Murray, was an insurance salesman. Her mother, Mary Campbell Van Horne Hopper, was a housewife who loved to study math and encouraged Grace’s interest in the subject. Grace’s maternal grandfather was a civil engineer for the city of New York and often took Grace on surveying trips. Grace’s family encouraged her to explore. When she was seven years old, she took apart her alarm clock to see how it worked. -

Reminicences of the WAVES US Navy (Retired)
INDEX for Interviews with Captain Joy Bright Hancock, U. S. Navy (Retired) AV-S Program, 49 Barnaby, Capt. Ralph, 25 Bureau of Aeronautics, 17; early setting up of files, 19-20; Newsletter, 23; editorial research, 31; public relations, 31-35 Carr, Wilbur J., 27 Chung, Dr. Margaret (Mom Chung), 55; Sons of Mom Chung - organization, 56 Darden, Capt., 117 de Flores, RADM Louis, 46-47, 106 Fechteler, Admiral William, 76 Gildersleeve, Dean Virginia, 66-69 Griffin, Capt. Virgil C., 109 Hancock, Capt. Joy Bright (Mrs. Ralph Ofstie), Enlistment, WWI, 2-6; uniform, WWI, 6-7; work assignments, WWI, 7-8; impact of a woman in service, 8; work at Cape May, 11-14; marriage, 14-15; job with BUAIR, 16, 22-23; State Dept. exams, 27-28; marriage to Comdr. Hancock, 25; takes up flying, 29; enrollment in WAVES, 40- 41; WWI ribbon bestowed by Adm. King, 41-42; her role in planning for WAVES, 54 ff. liaison work, 69-71; WAVE rep. for naval aviation, 75 ff; travels, 80-83; background advantages for WAVE job, 91; P.R. chores, 102-103; becomes Director of the WAVES, 111- 112; thoughts on success of WAVES, 131-134; retirement, 135-139 Hancock, Lt. Comdr., 24, 26 Holloway, Admiral James, 138 Jacobs, VADM Randall, 5, 6l Kamuri, David, 138 King, Admiral E. J., 37-40, 42a Little, Lt. Charles Gray, 11 Maas, Congressman Melvin, 51, 54 McAfee, Capt. Mildred, 59-60, 77-78, 102-103, 111-112 Moffatt, RADM William A., 16, 18, 21, 25, 43 NC-4, 10-11 Naval Air Station, Cape May, 9 New York Shipbuilding Co., 7-8 Nimitz, Admiral Chester: attitude towards WAVES, 52, 120-121 Nunn, Captain Ira, 128 Ofstie, VADM Ralph A., 50 Palmer, Capt. -

Shock Waves: Managing the Impacts of Climate Change on Poverty
Climate Change and Development Series SHOCK WAVES Managing the Impacts of Climate Change on Poverty Stephane Hallegatte, Mook Bangalore, Laura Bonzanigo, Marianne Fay, Tamaro Kane, Ulf Narloch, Julie Rozenberg, David Treguer, and Adrien Vogt-Schilb Shock Waves Managing the Impacts of Climate Change on Poverty Shock Waves Managing the Impacts of Climate Change on Poverty Stephane Hallegatte, Mook Bangalore, Laura Bonzanigo, Marianne Fay, Tamaro Kane, Ulf Narloch, Julie Rozenberg, David Treguer, and Adrien Vogt-Schilb © 2016 International Bank for Reconstruction and Development / The World Bank 1818 H Street NW, Washington, DC 20433 Telephone: 202-473-1000; Internet: www.worldbank.org Some rights reserved 1 2 3 4 18 17 16 15 This work is a product of the staff of The World Bank with external contributions. The findings, inter- pretations, and conclusions expressed in this work do not necessarily reflect the views of The World Bank, its Board of Executive Directors, or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Nothing herein shall constitute or be considered to be a limitation upon or waiver of the privileges and immunities of The World Bank, all of which are specifically reserved. Rights and Permissions This work is available under the Creative Commons Attribution 3.0 IGO license (CC BY 3.0 IGO) http://creativecommons.org/licenses/by/3.0/igo. -
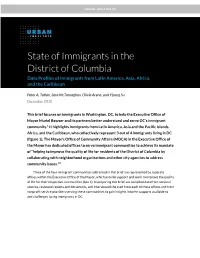
State of Immigrants in DC
URBAN–GREATER DC State of Immigrants in the District of Columbia Data Profiles of Immigrants from Latin America, Asia, Africa, and the Caribbean Peter A. Tatian, Sara McTarnaghan, Olivia Arena, and Yipeng Su December 2018 This brief focuses on immigrants in Washington, DC, to help the Executive Office of Mayor Muriel Bowser and its partners better understand and serve DC’s immigrant community.1 It highlights immigrants from Latin America, Asia and the Pacific Islands, Africa, and the Caribbean, who collectively represent 3 out of 4 immigrants living in DC (figure 1). The Mayor’s Office of Community Affairs (MOCA) in the Executive Office of the Mayor has dedicated offices to serve immigrant communities to achieve its mandate of “helping to improve the quality of life for residents of the District of Columbia by collaborating with neighborhood organizations and other city agencies to address community issues.”2 Three of the four immigrant communities addressed in this brief are represented by separate offices within the Executive Office of the Mayor, which provide support and work to improve the quality of life for their respective communities (box 1). In preparing this brief, we compiled data from national sources, reviewed reports and documents, and interviewed the staff from each of these offices and from nonprofit service providers serving these communities to gain insights into the supports available to and challenges facing immigrants in DC. BOX 1 District of Columbia Supporting Offices for Latino, Asian and Pacific Islander, and African Immigrants Mayor's Office on Latino Affairs (MOLA), https://ola.dc.gov Mayor's Office on Asian and Pacific Islander Affairs (MOAPIA), https://apia.dc.gov/ Mayor's Office on African Affairs (MOAA), https://oaa.dc.gov/ DC’s Immigrant Population Today Though Washington, DC, has not historically been a center for immigration to the US, since the 1980s our region has emerged as one of the country’s largest new gateway destinations for immigrant communities (Singer 2004). -

Urban Heat Islands During Heat Waves: a Comparative Study Between Boston and Phoenix
VOLUME 60 JOURNAL OF APPLIED METEOROLOGY AND CLIMATOLOGY MAY 2021 Urban Heat Islands during Heat Waves: A Comparative Study between Boston and Phoenix a a LIANG WANG AND DAN LI a Department of Earth and Environment, Boston University, Massachusetts (Manuscript received 4 June 2020, in final form 24 February 2021) ABSTRACT: In this study, we simulate the magnitude of urban heat islands (UHIs) during heat wave (HWs) in two cities with contrasting climates (Boston, Massachusetts, and Phoenix, Arizona) using the Weather Research and Forecasting (WRF) Model and quantify their drivers with a newly developed attribution method. During the daytime, a surface UHI (SUHI) is found in Boston, which is mainly caused by the higher urban surface resistance that reduces the latent heat flux and the higher urban aerodynamic resistance ra that inhibits convective heat transfer between the urban surface and the lower atmosphere. In contrast, a daytime surface urban cool island is found in Phoenix, which is mainly due to the lower urban ra that facilitates convective heat transfer. In terms of near-surface air UHI (AUHI), there is almost no daytime AUHI in either city. At night, an SUHI and an AUHI are identified in Boston that are due to the stronger release of heat storage in urban areas. In comparison, the lower urban ra in Phoenix enhances convective heat transfer from the atmosphere to the urban surface at night, leading to a positive SUHI but no AUHI. Our study highlights that the magnitude of UHIs or urban cool islands is strongly controlled by urban–rural differences in terms of aerodynamic features, vegetation and moisture conditions, and heat storage, which show contrasting characteristics in different regions. -

Women's History Month
Women’s History Month HONORING WOMEN WHO FIGHT ALL FORMS OF DISCRIMINATION March 2018 Women’s History Month Women’s History Month honors and celebrates the struggles and achievements of American women throughout the history of the United States. The Department of Defense (DoD) pays tribute to the women who, through their steadfast determination and inspirational contributions, have shaped America’s history and continue to pave the way forward. 2 Women’s History Month Origin Women’s History Month has its origins in 1981 when Congress passed Public Law 97-28 which authorized and requested the President to proclaim the week beginning March 7, 1982 as “Women’s History Week.” In 1987, after being petitioned by the National Women’s History Project, Congress passed Public Law 100-9 which designated the month of March, 1987 as “Women’s History Month.” Women's History Origin 3 Women’s History Month This year’s theme is: Honoring Women Who Fight All Forms Of Discrimination. This presentation features nine women: Pilot Bernice Haydu, Ensigns Harriet Pickens and Frances Wills, Lt. Cmdr. Marilyn Melendez Dykman, Lt. Susan Cuddy, Col. Debra Lewis, Capt. Eleanor L’Ecuyer, Capt. Mildred H. McAfee, and Pvt. Minnie Spotted Wolf. 4 Pilot Bernice “Bee” Haydu Women have been graduating from the Air Force Academy since 1980 and flying in combat missions since Operation Desert Storm. Prior to this however, women served as Women Airforce Service Pilots (WASPs) during World War II. Bernice “Bee” Haydu not only served as a WASP, but fought for them to be recognized as veterans. When the WASP program was disbanded in 1944, it left the women veterans no rank and no benefits for their service. -

The Contributions of Grace Murray Hopper to Computer
Sfr v * ""J THE CONTRIBUTIONS OF GRACE MURRAY HOPPER TO COMPUTER SCIENCE AND COMPUTER EDUCATION DISSERTATION Presented to the Graduate Council of the University of North Texas in Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY By Carmen L. Mitchell, B.A., M.S. Denton, Texas May, 1994 Sfr v * ""J THE CONTRIBUTIONS OF GRACE MURRAY HOPPER TO COMPUTER SCIENCE AND COMPUTER EDUCATION DISSERTATION Presented to the Graduate Council of the University of North Texas in Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY By Carmen L. Mitchell, B.A., M.S. Denton, Texas May, 1994 Mitchell, Carmen L., The Contributions of Grace Murray Hopper to Computer Science and Computer Education. Doctor of Philosophy (Higher Education), May, 1994, 110 pp. Sources consulted, 73 titles. This study explored the life and work of the late Grace Murray Hopper, Rear Admiral United States Naval Reserve. The study emphasized Hopper's contributions to computer science and computer science education, including her philosophy of teaching and learning, and her pedagogical legacy for today's teachers and scholars of computer science and computer science education. The study employed historical methodology, including personal interviews by the author of individuals who knew Hopper, both in and out of the military. Some of these individuals worked with Hopper during the early days of her computing career, while others knew Hopper during her time at the Pentagon and after her retirement, until her death in January, 1992. The study also included a thorough review of the written record, including a search through the Grace Murray Hopper collection donated to the Smithsonian Institution in Washington, D.C. -

A HISTORY of WOMEN in the COAST Guard by JOHN A
A HISTORY OF WOMEN IN THE COAST GuARD BY JOHN A. TILLEY Ida Lewis served as the keeper of Lime Rock Light on a small island in Newport, R.I., for 54 vears. She began tending the light, along with her mother, at the age of 75 after her father was immobilized bV a stroke. Lewis devel oped outstanding boat-handling skills while rowing back and forth to the main land. During her vears at the lighthouse. she rescued between 78 and 24 people. Lewis was one of manv women who kept America's lights lit and mariners safe. omen have been performing piers ... within any bay, inlet, harbor, or Coast Guard duties longer port of the United States, for rendering the than there has been a Coast navigation thereof easy and safe." The first W Guard. At least one profes female federal employees probably were sional ancestor of the modern female Coast lighthouse keepers. Guardsman predated the federal govern The old-fashioned lighthouse was a prim ment itself. In 1776, John Thomas joined the itive contraption. Its light came from a Army to fight in the Revolutionary War. His whale-oil lamp mounted behind a thick wife, Hannah, took over his job as keeper of glass lens, sometimes equipped with a Gurnet Point Light, near Plymouth, Mass. weight-driven mechanism to make it rotate The oldest root of the modern Coast and pump oil to the lamp. Guard's institutional family tree can be Along with the position of keeper went a traced back to Aug. 7, 1789, when the new house, usually built into the base of the Congress appropriated funds for "the nec light tower, and a plot of land on which the essary support, maintenance and repairs of keeper's family was expected to keep live all lighthouses, beacons, buoys and public stock and grow vegetables. -
Guide to the Grace Murray Hopper Collection
Guide to the Grace Murray Hopper Collection NMAH.AC.0324 Don Darroch 1990 Archives Center, National Museum of American History P.O. Box 37012 Suite 1100, MRC 601 Washington, D.C. 20013-7012 [email protected] http://americanhistory.si.edu/archives Table of Contents Collection Overview ........................................................................................................ 1 Administrative Information .............................................................................................. 1 Arrangement..................................................................................................................... 2 Biographical / Historical.................................................................................................... 2 Scope and Contents........................................................................................................ 2 Names and Subjects ...................................................................................................... 3 Container Listing ............................................................................................................. 4 Series 1: Technical Documents, 1944 - 1949.......................................................... 4 Series 2: Photographs of MARK II, 1948................................................................. 9 Series 3: Photographs at Harvard, 1944-1945...................................................... 11 Series 4: Reports and Articles, 1946 - 1948.........................................................