Annual Report – Full
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Wineries of Bendigo
Annual wine events Regional World’s Longest Lunch Bendigo, March Bendigo’s leafy Rosalind Park is the setting for this Wineries celebration of local wine and food. A degustation menu with Bendigo region wines awaits you at the gorgeous long table stretching through the park. of Bendigo Part of Melbourne Food and Wine Festival. Strategem Bendigo Winemakers Festival, April Bendigo’s gentle rolling hills unveil a wine The Strategem Bendigo Winemakers Festival region full of character and flavour. transforms Rosalind Park into Bendigo’s biggest alfresco wine garden with local wines, food stalls, Imagine yourself meandering along country roads live music and a great crowd. enjoying the view and being greeted by the winemakers at cellar door. Or, coming along to Barrel Tasting Weekend, July one of the local events for a perfect day of Bendigo region wine, food and music. Bendigo’s winemakers throw open the doors of their barrel halls and take you inside to taste wine straight Locally grown wines give a true flavour of a region from the barrel. full of winemaking history dating back to the 1850s. Today, Bendigo’s winemakers meticulously craft Bendigo Heritage Uncorked and Heritage After Dark plenty of award-winning wines. Take in these two unique events plus other niche wine Regular visitors to the region fondly refer to it as and food experiences as part of Bendigo Uncorked Week. “The Winemakers Region”, because chances are A week of individual events in October every year that you’ll meet the winemaker tending vines or working celebrates local wine and food in some of Bendigo’s most in the winery. -

List of Parishes in the State of Victoria
List of Parishes in the State of Victoria Showing the County, the Land District, and the Municipality in which each is situated. (extracted from Township and Parish Guide, Department of Crown Lands and Survey, 1955) Parish County Land District Municipality (Shire Unless Otherwise Stated) Acheron Anglesey Alexandra Alexandra Addington Talbot Ballaarat Ballaarat Adjie Benambra Beechworth Upper Murray Adzar Villiers Hamilton Mount Rouse Aire Polwarth Geelong Otway Albacutya Karkarooc; Mallee Dimboola Weeah Alberton East Buln Buln Melbourne Alberton Alberton West Buln Buln Melbourne Alberton Alexandra Anglesey Alexandra Alexandra Allambee East Buln Buln Melbourne Korumburra, Narracan, Woorayl Amherst Talbot St. Arnaud Talbot, Tullaroop Amphitheatre Gladstone; Ararat Lexton Kara Kara; Ripon Anakie Grant Geelong Corio Angahook Polwarth Geelong Corio Angora Dargo Omeo Omeo Annuello Karkarooc Mallee Swan Hill Annya Normanby Hamilton Portland Arapiles Lowan Horsham (P.M.) Arapiles Ararat Borung; Ararat Ararat (City); Ararat, Stawell Ripon Arcadia Moira Benalla Euroa, Goulburn, Shepparton Archdale Gladstone St. Arnaud Bet Bet Ardno Follett Hamilton Glenelg Ardonachie Normanby Hamilton Minhamite Areegra Borug Horsham (P.M.) Warracknabeal Argyle Grenville Ballaarat Grenville, Ripon Ascot Ripon; Ballaarat Ballaarat Talbot Ashens Borung Horsham Dunmunkle Audley Normanby Hamilton Dundas, Portland Avenel Anglesey; Seymour Goulburn, Seymour Delatite; Moira Avoca Gladstone; St. Arnaud Avoca Kara Kara Awonga Lowan Horsham Kowree Axedale Bendigo; Bendigo -

Road Management Plan 2020-2021
Department of Transport Road Maintenance Category - Road List Version : 1 ROAD NAME ROAD NUMBER CATEGORY RMC START RMC END ACHERON WAY 4811 4 ROAD START - WARBURTON-WOODS POINT ROAD (5957), WARBURTON ROAD END - MARYSVILLE ROAD (4008), NARBETHONG AERODROME ROAD 5616 4 ROAD START - PRINCES HIGHWAY EAST (6510), SALE ROAD END - HEART AVENUE, EAST SALE AIRPORT ROAD 5579 4 ROAD START - MURRAY VALLEY HIGHWAY (6570), KERANG ROAD END - KERANG-KOONDROOK ROAD (5578), KERANG AIRPORT CONNECTION ROAD 1280 2 ROAD START - AIRPORT-WESTERN RING IN RAMP, TULLAMARINE ROAD END - SHARPS ROAD (5053), TULLAMARINE ALBERT ROAD 5128 2 ROAD START - PRINCES HIGHWAY EAST (6510), SOUTH MELBOURNE ROAD END - FERRARS STREET (5130), ALBERT PARK ALBION ROAD BRIDGE 5867 3 ROAD START - 50M WEST OF LAWSON STREET, ESSENDON ROAD END - 15M EAST OF HOPETOUN AVENUE, BRUNSWICK WEST ALEXANDRA AVENUE 5019 3 ROAD START - HODDLE HIGHWAY (6080), SOUTH YARRA ROAD BREAK - WILLIAMS ROAD (5998), SOUTH YARRA ALEXANDRA AVENUE 5019 3 ROAD BREAK - WILLIAMS ROAD (5998), SOUTH YARRA ROAD END - GRANGE ROAD (5021), TOORAK ANAKIE ROAD 5893 4 ROAD START - FYANSFORD-CORIO ROAD (5881), LOVELY BANKS ROAD END - ASHER ROAD, LOVELY BANKS ANDERSON ROAD 5571 3 ROAD START - FOOTSCRAY-SUNSHINE ROAD (5877), SUNSHINE ROAD END - MCINTYRE ROAD (5517), SUNSHINE NORTH ANDERSON LINK ROAD 6680 3 BASS HIGHWAY (6710), BASS ROAD END - PHILLIP ISLAND ROAD (4971), ANDERSON ANDERSONS CREEK ROAD 5947 3 ROAD START - BLACKBURN ROAD (5307), DONCASTER EAST ROAD END - HEIDELBERG-WARRANDYTE ROAD (5809), DONCASTER EAST ANGLESEA -

Parish and Township Plan Numbers
Parish and Township plan numbers This is a complete list of Victorian parishes and townships, together with plan numbers assigned by the Victorian Department of Crown Lands and Survey at some point between 1950 and 1970. The list has been reproduced from the Vicmap Reference Tables on the Department of Sustainability and Environment's land information website. Browse the list or use a keyword search to identify the plan number/s for a location. The plans are listed alphabetically. Townships and parishes are inter-sorted on the list. Some entries refer to locations within parishes or townships; these entries may be duplicated. The plan number can be used to locate copies of plans that PROV holds in the series VPRS 16171 Regional Land Office Plans Digitised Reference Set. For example, using the Search within a Series page on the PROV online catalogue with series number '16171' and the text '5030' will return the specific plans relating to the township of Ballarat. In this case, searching for 'Ballaarat' by name will return al the plans in the Ballarat land district, covering much of central and western Victoria. PROV does not hold copies of plans for the locations highlighted in pale yellow below. In most cases this is because parish-level plans were not created for areas such as national parks, where there were few land transactions to record. Plans showing these locations can be downloaded from the landata website under the section 'Central Plan Office Records'. 5001 Township of Aberfeldy 2016 Parish of Angora 2001 Parish of Acheron 2017 -
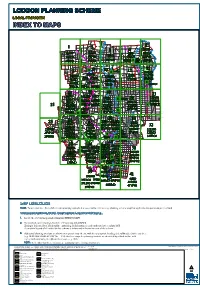
Loddon Planning Scheme Loddon Planning Scheme
LODDONLODDONLODDON PLANNINGPLANNINGPLANNING SCHEMESCHEMESCHEME LOCALLOCAL PROVISIONPROVISION INDEXINDEXINDEX TOTOTO MAPSMAPSMAPS 66RD RD 11 22 LODDON VALLEY Gredgwin 44 Creek 6ESO6ESO Canary33 44 33 Mincha Island 1LSIO1LSIO 2ESO12ESO1Leaghur Loddon Mt. Hope 1LSIO1LSIO 6SMO6SMOPYRAMID 1LSIO1LSIO Loddon 4HO4HO 6SMO6SMO Vale 4HO4HO 6SMO6SMO Barraport 3VPO13VPO1 1VPO11VPO1 2VPO12VPO1 Canary 4VPO14VPO1Pyramid 6VPO16VPO1Bald 1VPO11VPO1 Gladfield Minmindie Island South Rock 3VPO23VPO2 55 Hill5HO5HOLEITCHVILLE - 1VPO21VPO2 2VPO22VPO2 4SMO4SMORD 55 6VPO26VPO2 RD 5VPO15VPO1 BOORT - WYCHEPROOF BOORT - KERANG Yarrawalla RD BOORT - PYRAMID Boort 1313 99 88 RD Durham Terrick RD 99 1010 BOORT - PYRAMID Ox 1212 1212 Terrick Boort 11HO11HO 1212 77 Lake 1111 11HO11HO 77 1111 Mologa13SMO13SMO East Park Boort RD BOORT - CHARLTON Marmal 8ESO18ESO1 7ESO17ESO1 8ESO18ESO1 12SMO12SMO 13VPO113VPO1 7ESO17ESO1 10LSIO10LSIO Yarrawalla 8HO8HO 8LSIO8LSIO South 8HO8HO 8LSIO8LSIO 12VPO112VPO1 13VPO213VPO2Mitiamo 7LSIO7LSIO PYRAMID - BENDIGO 10VPO110VPO1Serpentine RD BOORT - MITIAMO 1414 7VPO17VPO1 8SMO8SMO 1414 Creek RD 14VPO214VPO2 10HO10HO Hayanmi Mysia 10HO10HO 7VPO27VPO2 8VPO18VPO1 8VPO28VPO2 Fernihurst Jarklin Bullock Wychitella Praire 1616 1818 Borung 1919 Calivil 2323 16HO16HO 18LSIO18LSIOWEDDERBURN18HO18HO Bears 23SMO23SMO 19HO19HO 2020 Lagoon20SMO20SMO 2222 16LSIO16LSIO 18SMO18SMO 18VPO118VPO1 CALDER 18SMO18SMO 18VPO118VPO1 19LSIO19LSIO 22SMO22SMO 23VPO123VPO1 16SMO16SMO 22SMO22SMO Yallock Korong Dingee Kinypanial Creek 2424 23VPO223VPO2 18VPO218VPO2Vale 18WMO18WMO -

NORTH WEST VICTORIA HISTORIC MINING PLOTS 1848-1976 Historic Notes
NORTH WEST VICTORIA HISTORIC MINING PLOTS 1848-1976 Historic Notes David Bannear Heritage Victoria CONTENTS: Amherst Division 3 Bendigo 23 Korong 212 Amherst Mining Division AMHERST DIVISION - GENERAL 1848: The original discovery of gold at Amherst or Daisy Hill occurred late in 1848. The discovery, by a shepherd Thomas Chapman, on the sheep run of McNeill and Hall, Glen Mona, caused the first gold rush in Victoria.[Flett, 1979, p254] 1851: Dr. Herman Bruhn, the well-known prospector, found gold in the area (Amherst) in 1851, but the first real discovery took place in about May 1852, when a party of Germans, going overland from Adelaide to Bendigo, got gold near the later site of Amherst Cemetery, close to Daisy Hill, where Chapman got his gold in 1848. [Flett, 1979, p254] 1852: The first important rush to Daisy Hill started, following the discovery of gold in Blacksmith’s Gully in December 1852. The locality was a bout a mile east of the later town, and was known as Cowley’s Rush. [Flett, 1979, p254] 1853: Gold was going discovered in March 1853 at Kangaroo Gully and Grecian Gully was opened in May. There was about 1000 diggers on the field [Flett, 1979, p254]. 1854: The first discovery of gold at Talbot, about three miles south-east of Daisy Hill, and then known as Back Creek, took place at Kangaroo Flat, on the Back Creek and about two miles south-west of Talbot, early in 1854. The workings there, until August, were confined to a small lead on the flat, but towards the end of 1854 gold was discovered at Ballarat Hill, and amidst considerable activity, built up to a ‘Goodwoman’s Rush’ in March 1855 [Flett, 1979, p254-255]. -
Loddon Shire Council Flood Emergency Plan – a Sub-Plan of the MEMP – Version 1, June 2019 Ii
Loddon Shire Council FLOOD EMERGENCY PLAN A Sub-Plan of the Municipal Emergency Management Plan For Loddon Shire Council and VICSES Unit Wedderburn Version 1, June 2019 “Intentionally Blank” Loddon Shire Council Flood Emergency Plan – A Sub-Plan of the MEMP – Version 1, June 2019 ii Table of Contents Table of Contents ............................................................................................................................................ iii Distribution of MFEP ........................................................................................................................................ v Document Transmittal Form / Amendment Certificate ................................................................................. v List of Abbreviations & Acronyms ................................................................................................................. vi Part 1. Introduction ....................................................................................................................................... 1 1.1 Approval and Endorsement .................................................................................................................... 1 1.2 Purpose and Scope of this Flood Emergency Plan ................................................................................ 1 1.3 Municipal Flood Planning Committee (MFPC) ....................................................................................... 1 1.4 Responsibility for Planning, Review & Maintenance of this Plan .......................................................... -

Bendigo & Heathcote Region
BENDIGO & HEATHCOTE REGION Victoria’s Goldfields Official Visitor Guide BENDIGO VISITOR CENTRE Australia’s grandest Visitor Centre TALK TO A LOCAL Our local specialists are here to help you plan your memorable visit to Bendigo. We can assist with: • Accommodation, attractions, tours and events • Visitor Map and Guide Books • Extensive local book collection and souvenirs With access to 120+ Bendigo accommodation properties, bookable in store, over the phone or online. Our service features personally managed accommodation, tour and event bookings, last minute rates and hot deals. LIVING ARTS SPACE A dynamic contemporary arts space showcasing unique local and regional talents. See Page 37 for further details. UNIQUELY BENDIGO Bendigo’s premier outlet for quality regional crafted designs. Take a piece of Bendigo home with you or visit us online at www.uniquelybendigo.com See Page 56 for further details. POST OFFICE GALLERY A satellite space of Bendigo Art Gallery has an annual program of changing exhibitions and events. See Page 37 for further details. Insta #explorebendigo Open everyday from 9am–5pm (except Christmas Day) 51-67 Pall Mall, Bendigo 3550 Bendigo’s Official Accommodation, Email: [email protected] Tour & Ticketing Specialists Freecall 1800 813 153 or visit www.bendigotourism.com CONTENTS ACKNOWLEDGEMENT OF COUNTRY The City of Greater Bendigo would like to acknowledge that we are on Dja Dja Wurrung and Taungurung Country whose ancestors and their descendants are the traditional owners of this country. We acknowledge that they have been custodians for many centuries and continue to perform age old ceremonies of celebration, initiation and renewal. We acknowledge their living culture and their unique role in the life of this region. -
NCCMA Annual Report 2007-08
Looking to the future, consolidating the past 2007–08 ANNUAL REPORT The communities we serve Patho Mincha Torrumbarry Bald Rock Pyramid Hill Yarrawalla Wharparilla Roslynmead Echuca Mologa Yarrawalla South Kotta Kanyapella South Mitiamo Pine Grove Simmie Hayanmi Strathallan Lockington Ballendella McColl Prairie Nanneella Calivil Tennyson Milloo Fairy Dell Rochester Diggora West Dingee Yallook Hunter Tandarra Kamarooka North Drummartin Kamarooka Kamarooka East Elmore Mayreef Summerfi eld Runnymeade Raywood Neilborough East Creek View Colbinabbin West Sebastian North Huntley Bagshot North Yarraberb Goornong Campbells Forest Myola East Myola BarnadownDerby Huntly Woodvale Muskerry East Leichardt Sailors Gully Myers Flat Toolleen Epsom Eaglehawk California Gully White Hills Marong Long Gully Wilson Reef Maiden Gully Bendigo Junortoun Golden Square Kennington Flora Hill Axedale Woodstock Kangaroo Flat Strathfi eld- saye Spring Gully Axe Creek Lockwood Mandurang Knowsley Shelbourne East Emu Creek Eppalock Lockwood South Shelbourne Mandurang South Derrinal Sedgwick Ravenswood Heathcote Pilchers Bridge Argyle Nuggetty Ravenswood South Porcupine Flat Harcourt North Sutton Grange Maldon Harcourt Culfearne Koondrook Teal Point Gannawarra Koroop Kerang East Milnes Bridge Mead McMillans Macorna North Wee Wee Rup Horfi eld Macorna Mincha West Leitchville Gunbower Cohuna Woorinen North Tyntynder South Beverford Tyntynder Central Speewa Kunat Tresco West Tresco Fish Point Benjeroop Winlaton Murrabit West Westby Mystic Park Beauchamp Lake Charm Lalbert Korrak -
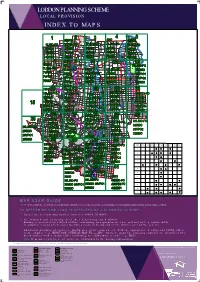
Loddon Planning Scheme Indextomaps
LODDON PLANNING SCHEME L O C A L P R O V I S I O N I N D E X T O M A P S RD D R k L e e OD r Gredgwin C D ON Canary D I V Mincha M Island A Leaghur Loddon A Mt. Hope L R L Y E P L Vale Barraport Y o d d o - LE n Canary L Bald Pyramid VI Gladfield CH Minmindie Island South IT Rock Hill LE RD D G R N A R E PROOF K BOORT - WYCHE - T ID R M RA O Y - P O T B R OO Yarrawalla RD B Boort RD Durham RD ON B T OORT - Ox RL PYRAMID HA Boort C Lake T - Mologa OR D East BO Boort R D I Marmal M A R Y Yarrawalla P - South O G I D N Mitiamo E B RD S MO e BOORT - MITIA r p e C n r t e i D e n R k e Hayanmi Mysia Fernihurst k c o ll Jarklin u B Wychitella Praire Borung Calivil N UR RB DE ED W Bears Lagoon CA LD ER Yallock Korong Dingee C - Kinypanial Vale r T e k R South e e D O k e R O r B R C Richmond iv er Plains Serpentine Y R A Kamarooka D Tandarra N D U O North R D I Wedderburn B Nine M Powlett T S Wedderburn A E Mile R W Y Plains Junction A P K - D O R O O R G A I M Kamarooka D A N K E B EVANS RD E N I T N r E P e R v Berrimal Kurraca E i Glenalbyn S R West Salisbury D West R k - c o R l N Kurting I E l A T u H A C Kurraca B W E E E Gowar R G H T D East I R Fentons B Inglewood Creek N R H U W B Y R E k Bridgewater on Loddon D e D e Campbells E r W Wehla C Yarraberb - FITZPATRICKS Kingower Forest D N R A RD G O L Logan D R Derby Rheola B N H EN W D O IG Arnold Y O D - Burkes L A E West T MAP EAO EMO HO LSIO-FO SMO VPO1 VPO2 BMO M U ESO1 Flat O R S U McIntyre - B S T L R A Leichardt O E R Arnold O T N H 5 A C l A U S D u W D G R b E Cochranes a N G -

DETAILS on PAGE 4 President’S Welcome
WIN A HOLIDAY TO THE PYRENEES ..... FREE ENTRY! DETAILS ON PAGE 4 President’s Welcome As Field Day President , I would like to extend a warm welcome to all our visitors to our 2014 Field Day. The Loddon Valley Stud Merinos consist of fifteen family owned and operated studs breeding large framed dual purpose sheep that the region is renowned for. I would also like to welcome two studs who are joining our field day for the first time. They are the Forest Springs Poll Merino Stud operated by Bruce Dean and the Hynam Poll Merino Stud of Kevin and Tracey Hynam Loddon Valley member studs once again proved over the last year that we can match any sheep in Australia whether it be at sheep shows, fleece competitions, wether trials, store sheep sales or ram sales The best pen of 3 weaner rams competition will again be run, giving visitors to our field day a chance to win an accommodation package at the Summerfield Winery and a meal at the Redbank Winery in the Pyrenees wine region. A big thank you to our sponsors and advertisers for helping make our Field Day a success and Elizabeth Todd (Secretary/Treasurer), Erroll Hay (Book Co-ordinator) and Robert Ipsen (Vice President) for jobs well done. Norm Weir, President Loddon Valley Stud Merino Breeders Association WE WOULD LIKE TO THANK THE MAJOR SPONSORS OF THE LODDON VALLEY STUD MERINO FIELD DAY STOCK & LAND RODWELLS & CO. PTY LTD STUDS DISPLAYING STUDS DISPLAYING LODDONON-PROPERTY VALLEY STUD MERINOAT SERPENTINE EAST LODDON TERRICK WEST AKERINGA KOOLE VALE DISPLAYING AT EAST LODDON WOOLBREEDERS DISPLAYING -

Wineries of Bendigo
Our Annual Wine Events World’s Longest Lunch Savour Bendigo wines matched to Wineries regionally-inspired dishes presented by Wine Bank on View. A gorgeous table will of Bendigo stretch along the grand boulevards of historic Rosalind Park. The first vines in the Bendigo region were planted in 1856 and, in less than twenty years, the wines from Rosalind Park, Bendigo these grapes were winning accolades in Europe. Each March, as part of the Rich, Ripe Reds! Melbourne Food & Wine Festival The judges of the 1873 Vienna Exhibition exclaimed of Bendigo’s early Hermitage, “No colonial wine Strategem Bendigo could be that good!” Winemakers Festival Meet the winemakers of the region, Through enterprise and hard work, Bendigo’s new sample the best Bendigo wines and enjoy wave of winemakers have placed this region at the live music in a tranquil garden setting. forefront of winemaking excellence today, with award-winning Shiraz and Cabernet Sauvignon wines. The region’s friendly, personal character is winning attention, too. The majority of Bendigo’s wineries Bendigo Wealth are small to medium-sized, and are still run by the Heritage Uncorked families who founded them. Regular visitors to An iconic moveable feast event that the region fondly refer to it as “The Winemakers’ showcases the best of Bendigo. Region”, knowing it is not uncommon to meet the Bendgo wines, quality restaurants winemakers, sleeves rolled up, tending vines or and grand gold rush architecture. working in the winery. Held every second weekend in October Now with more than 20 wineries, the Bendigo region Bendigo Central Business District offers an abundance of choice in wine tourism experiences.