Based Intervention to Improve Developmental Status
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Environmental Impact Assessment Report
Environmental Impact Assessment Report For Public Disclosure Authorized Changzhi Sustainable Urban Transport Project E2858 v3 Public Disclosure Authorized Public Disclosure Authorized Shanxi Academy of Environmental Sciences Sept, 2011 Public Disclosure Authorized I TABLE OF CONTENT 1. GENERAL ................................................................ ................................ 1.1 P ROJECT BACKGROUND ..............................................................................................1 1.2 B ASIS FOR ASSESSMENT ..............................................................................................2 1.3 P URPOSE OF ASSESSMENT AND GUIDELINES .................................................................4 1.4 P ROJECT CLASSIFICATION ...........................................................................................5 1.5 A SSESSMENT CLASS AND COVERAGE ..........................................................................6 1.6 I DENTIFICATION OF MAJOR ENVIRONMENTAL ISSUE AND ENVIRONMENTAL FACTORS ......8 1.7 A SSESSMENT FOCUS ...................................................................................................1 1.8 A PPLICABLE ASSESSMENT STANDARD ..........................................................................1 1.9 P OLLUTION CONTROL AND ENVIRONMENTAL PROTECTION TARGETS .............................5 2. ENVIRONMENTAL BASELINE ................................ ................................ 2.1 N ATURAL ENVIRONMENT ............................................................................................3 -

Due to the Special Circumstances of China Nancy L
Bridgewater Review Volume 5 | Issue 2 Article 6 Nov-1987 Due to the Special Circumstances of China Nancy L. Street Bridgewater State College, [email protected] Recommended Citation Street, Nancy L. (1987). Due to the Special Circumstances of China. Bridgewater Review, 5(2), 7-10. Available at: http://vc.bridgew.edu/br_rev/vol5/iss2/6 This item is available as part of Virtual Commons, the open-access institutional repository of Bridgewater State University, Bridgewater, Massachusetts. --------------ES SAY-------------- Due To The Special Circumstances ofCHIN1\... BY NANCY LYNCH STREET ,~d Ifim 'h, ,boY< 'id, in 'h, <xch'nge pmgrnm 'On"''' "'''",n Shanxi Teacher's University and Bridgewater State College. I pondered it for awhile, then dropped it. I would find out soon enough the "special circumstances of China." First, I had to get ready to go to China. Ultimately, the context of the phrase would enlighten me. During the academic year 1985-1986 I taught at Shanxi Teacher's University which is located in Linfen, Shanxi Province, People's Republic of China. Like the Chinese, I would soon learn the virtues of quietness and patience. I would listen and look and remember. Perhaps most important of all, I would make friends whom I shall never forget. FROM BE]ING TO LINFEN Cultural Revolution. Seventeen hours by from personal observations here and The Setting train north to Beijing, eight hours south abroad; and finally, from days and weeks The express train arrives in Linfen to Xi'an (home of the clay warriors found of talk and gathering oral history from from Beijing in the early morning, around in the tomb of the Emperor Ching Shi students, colleagues and friends. -

Evaluation of Sustainable Development of Resources-Based Cities in Shanxi Province Based on Unascertained Measure
sustainability Article Evaluation of Sustainable Development of Resources-Based Cities in Shanxi Province Based on Unascertained Measure Yong-Zhi Chang and Suo-Cheng Dong * Institute of Geographic Sciences and Natural Resources Research, the Chinese Academy of Sciences, Beijing 100101, China; [email protected] * Correspondence: [email protected]; Tel.: +86-10-64889430; Fax: +86-10-6485-4230 Academic Editor: Marc A. Rosen Received: 31 March 2016; Accepted: 16 June 2016; Published: 22 June 2016 Abstract: An index system is established for evaluating the level of sustainable development of resources-based cities, and each index is calculated based on the unascertained measure model for 11 resources-based cities in Shanxi Province in 2013 from three aspects; namely, economic, social, and resources and environment. The result shows that Taiyuan City enjoys a high level of sustainable development and integrated development of economy, society, and resources and environment. Shuozhou, Changzhi, and Jincheng have basically realized sustainable development. However, Yangquan, Linfen, Lvliang, Datong, Jinzhong, Xinzhou and Yuncheng have a low level of sustainable development and urgently require a transition. Finally, for different cities, we propose different countermeasures to improve the level of sustainable development. Keywords: resources-based cities; sustainable development; unascertained measure; transition 1. Introduction In 1987, the World Commission on Environment and Development (WCED) proposed the concept of “sustainable development”. In 1996, the first official reference to “sustainable cities” was raised at the Second United Nations Human Settlements Conference, namely, as being comprised of economic growth, social equity, higher quality of life and better coordination between urban areas and the natural environment [1]. -

Activated Carbon from China
SEPARATE-RATE RESPONDENTS PRELIMINARY EXPORTER SUPPLIER DUMPING MARGIN Alashan Yongtai Activated Carbon Co., Ltd., Changji Hongke Activated Carbon Co., Ltd., Datong Forward Beijing Pacific Activated Activated Carbon Co., Ltd., Datong Locomotive Coal & 72.52% Carbon Products Co., Ltd. Chemicals Co., Ltd., Datong Yunguang Chemicals Plant, Ningxia Guanghua Cherishmet Activated Carbon Co., Ltd., Ningxia Luyuangheng Activated Carbon Co., Ltd. Datong Juqiang Activated Datong Juqiang Activated Carbon Co., Ltd., Carbon Co., Ltd. 72.52% Datong Locomotive Coal & Datong Locomotive Coal & Chemicals Co., Ltd. Chemicals Co., Ltd. 72.52% Datong Municipal Yunguang Datong Municipal Yunguang Activated Carbon Co., Ltd. Activated Carbon Co., Ltd. 72.52% Datong Yunguang Chemicals Datong Yunguang Chemicals Plant Plant 72.52% Hebei Foreign Trade and Da Neng Zheng Da Activated Carbon Co., Ltd., Shanxi Advertising Corporation Bluesky Purification Material Co., Ltd. 72.52% Ningxia Guanghua Cherishmet Activated Carbon Ningxia Guanghua Cherishmet Activated Carbon Co., Ltd. 72.52% Co., Ltd. Ningxia Huahui Activated Ningxia Huahui Activated Carbon Co., Ltd. Carbon Co., Ltd. 72.52% Ningxia Mineral & Chemical Ningxia Baota Activated Carbon Co., Ltd. Limited 72.52% China Nuclear Ningxia Activated Carbon Plant, Ningxia Guanghua Activated Carbon Co., Ltd., Shanxi Xinhua Shanxi DMD Corporation Chemical Co., Ltd., Tonghua Xinpeng Activated Carbon 72.52% Factory Actview Carbon Technology Co., Ltd., Datong Forward Activated Carbon Co., Ltd., Datong Tri-Star & Power Shanxi Industry Technology Carbon Plant, Fu Yuan Activated Carbon Co., Ltd., Jing Trading Co., Ltd. 72.52% Mao (Dongguan) Activated Carbon Co., Ltd., Xi Li Activated Carbon Co., Ltd. Datong Forward Activated Carbon Co., Ltd., Ningxia Shanxi Newtime Co., Ltd. Guanghua Chemical Activated Carbon Co., Ltd., Ningxia 72.52% Tianfu Activated Carbon Co., Ltd. -

51381-001: Shanxi Changzhi Industrial Transformation And
Initial Poverty and Social Analysis October 2018 People’s Republic of China: Shanxi Changzhi Industrial Transformation and Economic Upgrading Demonstration Project This document is being disclosed to the public in accordance with ADB’s Public Communications Policy 2011. CURRENCY EQUIVALENTS (as of 16 October 2018) Currency unit – yuan (CNY) CNY1.00 = $0.14457 $1.00 = CNY6.9170 ABBREVIATIONS ADB – Asian Development Bank CCG – Changzhi City Government GDP – gross domestic product PRC – People’s Republic of China SPG – Shanxi Provincial Government WEIGHTS AND MEASURES km – kilometer km2 – square kilometer NOTE In this report, "$" refers to United States dollars. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. INITIAL POVERTY AND SOCIAL ANALYSIS Country: People’s Republic of China Project Title: Shanxi Changzhi Industrial Transformation and Economic Upgrading Lending/Financing Project Department/ East Asia Department/Urban and Social Modality: Division: Sectors Division I. POVERTY IMPACT AND SOCIAL DIMENSIONS A. Links to the National Poverty Reduction Strategy and Country Partnership Strategy The project is directly linked to the poverty reduction strategy and new-type urbanization of the People’s Republic of China (PRC) through industrial transformation and economic upgrading. It will be implemented in Changzhi City1 in the Southeast of Shanxi Province. The City has a land area of 13,955 km² with 13 counties (cities and districts), 1 national-level high-tech development zone and 4 provincial-level economic and technological development zones. -

The Fen River in Taiyuan, China: Ecology, Revitalization, and Urban Culture
The Fen River in Taiyuan, China: Ecology, Revitalization, and Urban Culture Matthias Falke Location of Taiyuan, Shanxi province, and the Fen River Basin This map was created by Matthias Falke in 2016, using Arc Map and the basemap layer World Topographic Map; map materials are from Openstreetmap contributors. This work is licensed under a Creative Commons Attribution-ShareAlike 2.0 Generic License . Shanxi (山西) and its fertile loess-covered landscapes are also known as the cradle of China’s civilization. The 716-km-long Fen River (汾河) or Mother River (母亲河) drains most of the province via the basin of Taiyuan. The river’s stunning scenery, once the subject of poetry during the Jin (金朝, 1125–1234) and Yuan (元朝, 1279–1368) dynasties, quickly deteriorated after industrialization in the late 1950s. The construction of dams, extensive irrigation of farmland, and wastewater discharge severely impacted the river’s ecosystem. From 1956 to 2013, the average surface runoff fell from 2.65 billion m³ to 1.33 m³. Moreover, overexploitation of groundwater dropped the groundwater level in the Fen River basin by 81.4 meters. Source URL: http://www.environmentandsociety.org/node/7679 Print date: 09 July 2019 11:15:32 Falke, Matthias. "The Fen River in Taiyuan, China: Ecology, Revitalization, and Urban Culture ." Arcadia (Autumn 2016), no. 17. View of four cokeries in the Gujiao area with an annual capacity of Traditional dwelling in the rural part of Gujiao 3.8 million metric tons per year before their integration into a Photo taken by Harald Zepp, 2010. combined coke processing facility This work is used by permission of the copyright holder. -

The 9Th East China Partial Differential Equations Conference & Shanxi
The 9th East China Partial Differential Equations Conference & Shanxi International Conference on Partial Differential Equations (First Announcement) Shanxi University, Taiyuan, Shanxi, China July 16{19, 2012 Aim of the conference: The 9th East China Partial Differential Equations Conference & Shanxi International Conference on Partial Differential Equations, is to be held at Taiyuan, Shanxi, China, from July 16th to July 19th of 2012. This conference is jointly organized by the School of Mathematical Sciences of Shanxi University (Shanxi, Taiyuan), the Department of Mathematics and the Center for PDE of East China Normal University (Shanghai). It is our goal to increase the academic exchanges and interactions in PDE research in China, and also to showcase the state of art in PDE research to the young researchers especially in Shanxi. Registration: If you plan to participate this conference, please send us an e-mail by June 1st, 2012 to the organizing committee via email [email protected] and containing your name, affiliation, postal address, e-mail address, travel schedule and additional information and comments. Deadline: The deadline for registration is June 1st, 2012. Titles and abstracts of all the invited talks/contributed talks must be received by June 1st, 2012. Abstracts should be typed in LaTeX or plain text document, containing your name, institute affiliation, postal address, e-mail address, title and abstract, not to exceed 200 words and sent by email to [email protected]. Conference Schedule: July 15 (Sunday): Arrival -

People's Republic of China: Shanxi Environment Improvement Project
Performance Evaluation Report Reference Number: PPE: PRC 2009-60 Project Number: 28388 Loan Number: 1715 December 2009 People's Republic of China: Shanxi Environment Improvement Project Independent Evaluation Department CURRENCY EQUIVALENTS Currency Unit – yuan (CNY) At Appraisal At Completion At Independent Evaluation (November 1999) (March 2006) (July 2009) CNY1.00 = $0.121 $0.124 $0.144 $1.00 = CNY 8.278 CNY8.039 CNY6.950 ABBREVIATIONS ADB – Asian Development Bank ADTA – advisory technical assistance CBM/CMM – Coal-bed-methane/coal-mine-methane CHP – combined heat power CO2 – carbon dioxide DDHC – Datong District Heating Company DDHP – Datong District Heating Project EA – executing agency EARD – East Asia Department EIRR – economic internal rate of return EPB – Environmental Protection Bureau ET – emissions permit trading FIRR – financial internal rate of return HES – Heat exchange station ICB international competitive bidding JGC – Jiaoqu Gas Company LPG – liquefied petroleum gas NEMC – national environmental monitoring center NO2 – nitrogen dioxide NOx – nitrogen oxide PCB – price control bureau PCR – project completion report PDP – pollution discharge permit PGC – Pingding Gas Company PCR – project completion report PMO – project management office PPER – project performance evaluation report PPTA – project preparatory technical assistance PRC – People's Republic of China RESC – regional environmental supervision center RRP – report and recommendation of the President SO2 – sulfur dioxide SPG – Shanxi provincial government SSCCL -

Up to Jan 16, 2012)
Current Location: Project Information Newly Approved Projects by DNA of China (Total: 76) (Up to Jan 16, 2012) Estimated Project Ave. GHG No. Project Name Project Owner CER Buyer Type Reduction (tCO2e/y) Ningxia Zhongwei China Power Investment Xiangshan Wind-farm Corporation Ningxia China Power Renewable 1 Energy Aluminium Group Treasure Boat Limited 87,402 Investment Corporation energy Zhongwei New Energy Fanjiazhai 49.5MW Co., Ltd. Project Guodian Shuozhou Guodian Shuozhou Haifeng Hutoushan Renewable Shell Trading International 2 Haifeng Wind Power Co., 84,611 Phase II 49.5MW Wind energy Limited Ltd. farm Project Guodian Shuozhou Guodian Shuozhou Haifeng Liujiayao Renewable Shell Trading International 3 Haifeng Wind Power Co., 89,489 49.5MW Wind farm energy Ltd. Ltd. Project Henan Biyang China Resources New Renewable 4 Zhongtian Wind Power Energy (Biyang) Wind Unilateral project 91,087 energy Project Power Co., Ltd. Guangdong Xinyi China Resources New Renewable 5 Qianpai Wind Power Energy (xinyi) Wind Unilateral project 77,916 energy Project Power Co., Ltd. Datang Qiubei Renewable Datang Qiubei Wind 6 yangxiongshan Wind EDF Trading Limited 85,261 energy Power Co., Ltd. Power Project Henan Yuxi Yanshan Sanmenxia Huayang Renewable 7 Wind Power Project Power Generation Co., EDF Trading Limited 88,254 energy Ltd. Tuokexun Wind Farm Datang Tuokexun Wind Renewable 8 Phase II Project Power Development Co., EDF Trading Limited 87,450 energy Ltd. Yunnan Eryuan Renewable Datang Eryuan Fengyu 9 Qilongshan Wind Power EDF Trading Limited 96,653 energy Wind Power Co., Ltd. Project Yunnan Eryuan Fengle Renewable Datang Eryuan Fengyu 10 EDF Trading Limited 89,550 Wind Power Project energy Wind Power Co., Ltd. -
The Security and Stability Analysis of 500Kv West Channel to Shanxi Datong Power Grid
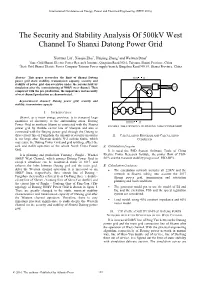
International Conference on Energy, Power and Electrical Engineering (EPEE 2016) The Security and Stability Analysis Of 500kV West Channel To Shanxi Datong Power Grid Xinyuan Liu1, Xiaojia Zhai2, Huiping Zheng1 and Weiwen Duan1 1State Grid Shanxi Electric Power Research Institute, Qingnian Road NO.6, Taiyuan, Shanxi Province, China 2State Grid Shanxi Electric Power Company Taiyuan Power supply branch, Bingzhou Road NO.89, Shanxi Province, China Abstract—This paper researches the limit of Shanxi Datong power grid static stability, transmission capacity, security and stability of power grid characteristics under the serious fault by simulation after the commissioning of 500kV west channel. Then compared with the pre production, the importance and necessity of west channel production are demonstrated. Keywords-west channel; Datong power grid; security and stability; transmission capacity I. INTRODUCTION Shanxi, as a major energy province, is to transport large quantities of electricity to the surrounding areas. Datong Power Grid in northern Shanxi is connected with the Shanxi FIGURE I. THE TOPOLOGY OF DATONG 500KV POWER GRID power grid by Double circuit line of Shenyan and also is connected with the Beijing power grid through the Datong to three circuit line of Fangshan. the amount of security measures II. CALCULATION PROGRAM AND CALCULATION is too large after Shenyan double N-2 serious faults, which CONDITION may cause the Datong Power Grid and grid splitting, affect the safe and stable operation of the whole North China Power A. Calculation Program Grid. It is used the PSD System Software Tools of China It is planning and production Yantong - Pinglu - Wuzhai Electric Power Research Institute, the power flow of PSD- 500kV West Channel, which ensures Datong Power Grid in BPA and the transient stability program of PSD-BPA. -

Foguangsi on Mount Wutai: Architecture of Politics and Religion Sijie Ren University of Pennsylvania, [email protected]
University of Pennsylvania ScholarlyCommons Publicly Accessible Penn Dissertations 1-1-2016 Foguangsi on Mount Wutai: Architecture of Politics and Religion Sijie Ren University of Pennsylvania, [email protected] Follow this and additional works at: http://repository.upenn.edu/edissertations Part of the Asian Studies Commons, History of Art, Architecture, and Archaeology Commons, History of Religion Commons, and the Religion Commons Recommended Citation Ren, Sijie, "Foguangsi on Mount Wutai: Architecture of Politics and Religion" (2016). Publicly Accessible Penn Dissertations. 1967. http://repository.upenn.edu/edissertations/1967 This paper is posted at ScholarlyCommons. http://repository.upenn.edu/edissertations/1967 For more information, please contact [email protected]. Foguangsi on Mount Wutai: Architecture of Politics and Religion Abstract Foguangsi (Monastery of Buddha’s Radiance) is a monastic complex that stands on a high terrace on a mountainside, in the southern ranges of Mount Wutai, located in present-day Shanxi province. The mountain range of Wutai has long been regarded as the sacred abode of the Bodhisattva Mañjuśrī and a prominent center of the Avataṃsaka School. Among the monasteries that have dotted its landscape, Foguangsi is arguably one of the best-known sites that were frequented by pilgrims. The er discovery of Foguangsi by modern scholars in the early 20th century has been considered a “crowning moment in the modern search for China’s ancient architecture”. Most notably, the Buddha Hall, which was erected in the Tang dynasty (618-907 CE), was seen as the ideal of a “vigorous style” of its time, and an embodiment of an architectural achievement at the peak of Chinese civilization. -

Natural Resources, Rent Dependence, and Public Goods Provision in China: Evidence from Shanxi’S County-Level Governments Yuyi Zhuang* and Guang Zhang
Zhuang and Zhang The Journal of Chinese Sociology (2016) 3:20 The Journal of DOI 10.1186/s40711-016-0040-3 Chinese Sociology RESEARCH Open Access Natural resources, rent dependence, and public goods provision in China: evidence from Shanxi’s county-level governments Yuyi Zhuang* and Guang Zhang * Correspondence: [email protected] Abstract School of Public Affairs, Xiamen University, Xiamen, Fujian Province This paper investigates how natural-resource endowments affect the provision of 361005, People’s Republic of China local public goods in China. According to fiscal sociology, due to the rentier effect, resource-rich local governments tend to have more state autonomy and are less responsive to society, resulting in poor governance. Moreover, due to political myopia, resource-abundant local governments tend to neglect the accumulation of human capital. Shanxi’s county-level governments are excellent samples to test these hypotheses. Statistical results show that resource-abundant local governments tend to spend less on social expenditures as well as specific education, social security and healthcare, and environmental protection expenditures. Meanwhile, coal-rich governments spend significantly more on self-serving administrative expenditures. The results suggest that negative impacts of natural resources on governmental fiscal extraction and expenditure behaviors are an important causal mechanism of the resource-curse hypothesis. To curb this problem, the current fiscal system needs to be reformed accordingly. Keywords: Resource curse, Coal, Public goods provision, Shanxi Province Introduction Why are developing countries and regions rich in natural resources often characterized by slow economic growth? Exploring this “resource curse,” economists, political scien- tists, and sociologists have put forward various causal mechanisms and explanations.