Ensuring Access to Safe Abortion Supplies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Abortion and the Law in New
NSW PARLIAMENTARY LIBRARY RESEARCH SERVICE Abortion and the law in New South Wales by Talina Drabsch Briefing Paper No 9/05 ISSN 1325-4456 ISBN 0 7313 1784 X August 2005 © 2005 Except to the extent of the uses permitted under the Copyright Act 1968, no part of this document may be reproduced or transmitted in any form or by any means including information storage and retrieval systems, without the prior written consent from the Librarian, New South Wales Parliamentary Library, other than by Members of the New South Wales Parliament in the course of their official duties. Abortion and the law in New South Wales by Talina Drabsch NSW PARLIAMENTARY LIBRARY RESEARCH SERVICE David Clune (MA, PhD, Dip Lib), Manager..............................................(02) 9230 2484 Gareth Griffith (BSc (Econ) (Hons), LLB (Hons), PhD), Senior Research Officer, Politics and Government / Law .........................(02) 9230 2356 Talina Drabsch (BA, LLB (Hons)), Research Officer, Law ......................(02) 9230 2768 Lenny Roth (BCom, LLB), Research Officer, Law ...................................(02) 9230 3085 Stewart Smith (BSc (Hons), MELGL), Research Officer, Environment ...(02) 9230 2798 John Wilkinson (MA, PhD), Research Officer, Economics.......................(02) 9230 2006 Should Members or their staff require further information about this publication please contact the author. Information about Research Publications can be found on the Internet at: www.parliament.nsw.gov.au/WEB_FEED/PHWebContent.nsf/PHPages/LibraryPublications Advice on -

The Clinton Administration's Promotion of Abortion at the 1994 Cairo Conference and the Strength of the Islamic Response
Rumage: Resisting the West: The Clinton Administration's Promotion of Abo CALIFORNIA WESTERN INTERNATIONAL LAW JOURNAL VOLUME 27 FALL 1996 NUMBER 1 RESISTING THE WEST: THE CLINTON ADMINISTRATION'S PROMOTION OF ABORTION AT THE 1994 CAIRO CONFERENCE AND THE STRENGTH OF THE ISLAMIC RESPONSE SARAH A. RUMAGE" "When I use a word," Humpty Dumpty said, in rather a scornful tone, "it means just what I choose it to mean-neither more nor less." "The question is," said Alice, "whether you can make words mean so many different things." "The question is," said Humpty Dumpty, "which is to be master-that's all."' "Whoever hath an absolute authority to interpret any written or spoken laws, it is he who is truly the lawgiver, to all intents and purposes, and not the person who first spoke or wrote them. "2 INTRODUCTION Who makes the law, and who decides what the law means? For modem lawyers, the true riddle is not in the actors' identification, but whether these are different questions involving different actors, or instead the same question involving the same actors. For theologians, however, the question may even signify the dividing point between God and man. And until quite recently, * B.A., University of Miami (Florida) in anthropology, 1976; J.D., New York Law School, 1982; M.A. in history, 1993; LL.M. Temple University School of Law, 1996; Ph.D. candidate at John Hopkins University School of Advanced International Studies. I wish to thank Professor Fouad Ajami for his helpful comments and encouragement, Professor Imad-Ad-Dean Ahmad for his great patience and critical eye, Professor Robert Gurland for opening the world of philosophical ethics to me, and especially my students at Temple University School of Law, who never failed to make me think. -
Abortion Facts and Figures 2021
ABORTION FACTS & FIGURES 2021 ABORTION FACTS & FIGURES TABLE OF CONTENTS PART ONE Introduction . 1 Global Overview . 2 African Overview . 4 By the Numbers . 6 Maternal Health . .9 Safe Abortion . 11 Unsafe Abortion . 13 Post-Abortion Care . 15 Contraception . 17 Unmet Need for Family Planning . 22 Abortion Laws and Policies . 24. PART TWO Glossary . 28 Appendix I: International Conventions . 30. Appendix II: How Unsafe Abortions Are Counted . 32 Appendix III: About the Sources . .33 Regional Data for Africa . 34 Regional Data for Asia . 44 Regional Data for Latin America and the Caribbean . 54. POPULATION REFERENCE BUREAU Population Reference Bureau INFORMS people around the world about population, health, and the environment, and EMPOWERS them to use that information to ADVANCE the well-being of current and future generations . This guide was written by Deborah Mesce, former PRB program director, international media training . The graphic designer was Sean Noyce . Thank you to Alana Barton, director of media programs; AÏssata Fall, senior policy advisor; Charlotte Feldman-Jacobs, former associate vice president; Kate P . Gilles, former program director; Tess McLoud, policy analyst; Cathryn Streifel, senior policy advisor; and Heidi Worley, senior writer; all at PRB, for their inputs and guidance . Thank you as well to Anneka Van Scoyoc, PRB senior graphic designer, for guiding the design process . © 2021 Population Reference Bureau . All rights reserved . This publication is available in print and on PRB’s website . To become a PRB member or to order PRB materials, contact us at: 1875 Connecticut Ave ., NW, Suite 520 Washington, DC 20009-5728 PHONE: 1-800-877-9881 E-MAIL: communications@prb .org WEB: www .prb .org For permission to reproduce parts of this publication, contact PRB at permissions@prb org. -

Abortion Care in South-East Asia Region2.Indd
Policies, Programme and Services for Comprehensive Abortion Care in South-East Asia Region i ii Policies, programme and services for comprehensive abortion care in South-East Asia Region iii Policies, programme and services for comprehensive abortion care in South-East Asia Region ISBN 978-92-9022-823-3 © World Health Organization 2021 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial- ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specifi c organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization (http://www.wipo.int/amc/en/mediation/ rules/). Suggested citation. Policies, programme and services for comprehensive abortion care in South-East Asia Region. -

Determinants of Modern Contraceptive Use In
DETERMINANTS OF MODERN CONTRACEPTIVE USE IN CAMEROON FROM 1991 TO 2004 By CONSOLER TENUG TEBOH Presented to the Faculty of the Graduate School of The University of Texas at Arlington in Partial Fulfillment of the Requirements for the Degree of DOCTOR OF PHILOSOPHY THE UNIVERSITY OF TEXAS AT ARLINGTON December 2011 Copyright © by Consoler Teboh 2011 All Rights Reserved DEDICATION This dissertation is dedicated to a few very special people in my life, my mother: Esther Acha Teboh; my beloved wife: Christina Teboh; and the kids: Sheila, Batuo, and Esther. ACKNOWLEDGEMENTS The pursuit of studies at the doctoral level requires persistence, dedication and perseverance. In spite of these tenets, the student’s social capital in the form of guidance, mentorship and support cannot be overemphasized. Although it is humanely impossible to mention every individual who has financially, physically and emotionally supported me during the course of the program, I would like to acknowledge those who symbolically shaped my life and helped me in the completion of my academic work. I would like to start by thanking my wife and children without whom I may not have been motivated to finish the program. They have endured the long absences that I took away from quality family time. I would also like to thank my mothers: Mrs. Sophie Teboh and Mrs. Esther Teboh; brothers: Ni Dan, Ni Gabby Ni Alex, John and Emmanuel; my sisters: Ma Eli, Ma Anna, Ma Mado and Ma Bri; my in-laws, Mrs. L. Baiye, Mrs. A. Baiye, Mr. J. Baiye the children, Ni Mike, Manyi Yellow; and my aunt, Ma Grace Ndam, and all my nieces and nephews for their constant support and encouragement throughout the years. -
Preventing Unsafe Abortion and Its Consequences Priorities for Research and Action
Priorities for Action Research and Abortion Preventing and Unsafe its Consequences nsafe abortion is a significant yet preventable cause of maternal mortality and morbidity. The Ugravity and global incidence of unsafe abortion Preventing call for a better understanding of the factors behind the persistence of unsafe abortion and of the barriers to preventing unsafe abortion and managing its conse- Unsafe Abortion quences. This volume brings together the proceedings from an inter-disciplinary consultation to assess the and its global and regional status of unsafe abortion and to identify a research and action agenda to reduce unsafe abortion and its burden on women, their families, and Consequences public health systems. The volume addresses a compre- hensive range of issues related to research on prevent- ing unsafe abortion, outlines regional priorities, and Priorities for identifies critical topics for future research and action on preventing unsafe abortion. Research and Action Iqbal H. Iqbal Shah H. Warriner Ina K. Editors Ina K. Warriner Iqbal H. Shah cover 4.indd 1 31/01/2006 13:34:26 Preventing Unsafe Abortion and its Consequences Priorities for Research and Action Editors Ina K. Warriner Iqbal H. Shah A-Intro.indd 1 09/02/2006 10:44:45 Suggested citation: Warriner IK and Shah IH, eds., Preventing Unsafe Abortion and its Consequences: Priorities for Research and Action, New York: Guttmacher Institute, 2006. 1. Abortion, Induced - adverse effects 2. Abortion, Induced - epidemiology 3. Women’s health services 4. Health priorities -

Modernization and Contraception in Kenya
MODERNIZATION AND CONTRACEPTION IN KENYA FROM 1998 TO 2008-2009 by DIANA ALAKA OPOLLO Presented to the Faculty of the Graduate School of Social Work The University of Texas at Arlington in Partial Fulfillment of the Requirements for the Degree of DOCTOR OF PHILOSOPHY THE UNIVERSITY OF TEXAS AT ARLINGTON December 2011 Copyright © by Diana Alaka Opollo 2011 All Rights Reserved DEDICATION This dissertation is dedicated to the most special people in my life, with whom I have been able to achieve my dreams: my father, the Late Mr. Phillip Ochara Opollo and my mother, Mrs. Joyce A. Opollo. ACKNOWLEDGEMENTS Pursuing a doctorate degree requires extreme dedication, tenacity, and perseverance. Equally required and certainly very important, more times than others, are support and the right guidance. While this page is not enough to mention each person who has supported me in my academic journey, I would like to specially thank a few who significantly influenced my life, and helped me to complete my higher education and achieve my dreams. My academic journey began at a very young age; the vision and desire of pursuing a doctorate degree was instilled in me by my family at an early age, but that was just a dream. With the consistent support and unconditional love from my family; I was able to complete my education. I would like to start by thanking my immediate family for their constant support and encouragement throughout the years; my father, the late Phillip Ochara Opollo, my mother Mrs. Joyce Opollo, my sisters Nancy Achieng, Winnie Aguko, Leah Vaughn, Rachel Tschann, Jakki Opollo, and my brothers Ken Opollo and Bobby Opollo. -

MODELING SON PREFERNCE in PAKISTAN by SADIA SAEED
MODELING SON PREFERNCE IN PAKISTAN by SADIA SAEED Presented to the Faculty of the Graduate School of The University of Texas at Arlington in Partial Fulfillment of the Requirements for the Degree of DOCTOR OF PHILOSOPHY THE UNIVERSITY OF TEXAS AT ARLINGTON MAY 2012 Copyright © by Sadia Saeed 2012 All Rights Reserved ACKNOWLEDGEMENTS Pursuing doctoral studies requires dedication, hard work, patience and perseverance, support and guidance. Though only my name will be appear on the title page of this dissertation, there are many people behind this effort and I owe my gratitude to all those people who supported and helped me during my research and graduate studies. Without their help and support I would not be able to complete my studies. First of all I would like to thank my late father Muhammad Saeed Dar. My PhD was his dream. In a male dominant society, where sons are considered precious gems, my father always considered me a treasure. He always said that girls are a blessing from Allah Almighty and I am blessed that Allah Almighty gave me a daughter like you. He never differentiated between me and my brother. He always said that girls should be highly educated, independent, and confident. It was his guidance, support and encouragement which gave me the courage to travel alone to the United States to pursue my PhD. I would like to thank my mother Nasira Saeed, who always helped me in every matter of my life. She is a high school graduate, but she always helped me in my studies. She used to sit with me through the whole night during my exams. -

Abortion Policies and Reproductive Health Around the World
Abortion Policies and Reproductive Health around the World United Nations Department of Economic and Social Affairs Population Division DESA The Department of Economic and Social Affairs of the United Nations Secretariat is a vital interface between global policies in the economic, social and environmental spheres and national action. The Department works in three main interlinked areas: (i) it compiles, generates and analyses a wide range of economic, social and environmental data and information on which States Members of the United Nations draw to review common problems and take stock of policy options; (ii) it facilitates the negotiations of Member States in many intergovernmental bodies on joint courses of action to address ongoing or emerging global challenges; and (iii) it advises interested Governments on the ways and means of translating policy frameworks developed in United Nations conferences and summits into programmes at the country level and, through technical assistance, helps build national capacities. Notes The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. This report presents data for countries using a traditional classification by development group. The “developed regions” comprise all countries and areas of Europe plus Northern America, Australia, New Zealand and Japan. The “developing regions” comprise all countries and areas of Africa, Asia (excluding Japan), Latin America and the Caribbean plus Melanesia, Micronesia and Polynesia. -

Abortion, Family Planning, and Population Policy: Prospects for the Common-Ground Approach
Fairfield University DigitalCommons@Fairfield Sociology & Anthropology Faculty Publications Sociology & Anthropology Department 9-2009 Abortion, family planning, and population policy: Prospects for the common-ground approach Dennis Hodgson Fairfield University, [email protected] Follow this and additional works at: https://digitalcommons.fairfield.edu/sociologyandanthropology- facultypubs Archived with permission from the copyright holder. Copyright 2009 Wiley and Population Council. Link to the journal homepage: (http://wileyonlinelibrary.com/journal/padr) Peer Reviewed Repository Citation Hodgson, Dennis, "Abortion, family planning, and population policy: Prospects for the common-ground approach" (2009). Sociology & Anthropology Faculty Publications. 37. https://digitalcommons.fairfield.edu/sociologyandanthropology-facultypubs/37 Published Citation Hodgson, Dennnis. "Abortion, family planning, and population policy: Prospects for the common-ground approach" Population and Development Review 35, no. 3 (September 2009): 479-518. This item has been accepted for inclusion in DigitalCommons@Fairfield by an authorized administrator of DigitalCommons@Fairfield. It is brought to you by DigitalCommons@Fairfield with permission from the rights- holder(s) and is protected by copyright and/or related rights. You are free to use this item in any way that is permitted by the copyright and related rights legislation that applies to your use. For other uses, you need to obtain permission from the rights-holder(s) directly, unless additional rights -
Abortion Worldwide 2017: Uneven Progress and Unequal Access
Uneven Progress and Unequal Access Uneven Progress and Unequal Access Susheela Singh Lisa Remez Gilda Sedgh Lorraine Kwok Tsuyoshi Onda Acknowledgments his report was written by Susheela Singh, Lisa San Francisco, and Fundación Oriéntame and TRemez, Gilda Sedgh, Lorraine Kwok and Tsuyoshi Fundación Educación para la Salud Reproductiva Onda—all of the Guttmacher Institute. It was (USA and Colombia); Ilana Dzuba, Gynuity (USA); edited by Jared Rosenberg; Michael Moran and Katy Footman, Marie Stopes International (UK); Kathleen Randall were responsible for production. Diana Greene Foster, University of California, San Francisco; Beth Fredrick, Johns Hopkins Bloomberg The authors thank the following Guttmacher School of Public Health (USA); Chimaroake colleagues for their comments and help in Izugbara, African Population and Health Research developing this report: Akinrinola Bankole, Sneha Centre (Kenya); Shireen Jejeebhoy, Independent Barot, Onikepe Owolabi, Ann Starrs and Gustavo Researcher (India); Katherine Mayall, Center for Suarez, for reviewing a draft of the report; Jonathan Reproductive Rights (USA); Ndola Prata, University Bearak, for invaluable assistance with data; Suzette of California, Berkeley; Mahesh Puri, Center for Audam and Mia Zolna, for data analysis; Alanna Research on Environment, Health and Population Galati, Rachel Jones, Elizabeth Nash and Anna Activities (Nepal); Mónica Roa, Independent Popinchalk, for providing follow-up data; and Alex Consultant (Colombia); Zeba Sathar, Population Arpaia for research support. They -
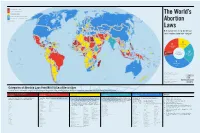
World-Abortion-Map.Pdf
I PROHIBITED ALTOGETHER II TO SAVE THE WOMAN’S LIFE III TO PRESERVE HEALTH GREENLAND The World’s IV BROAD SOCIAL OR ECONOMIC GROUNDS FINLAND V ON REQUEST (GESTATIONAL LIMITS VARY) ICELAND SWEDEN RUSSIAN FEDERATION UNKNOWN CANADA NORWAY Abortion ESTONIA LATVIA NORTHERN IRELAND DENMARK LITHUANIA NETHERLANDS IRELAND GREAT BELARUS BRITAIN GERMANY POLAND BELGIUM CZECH LUXEMBOURG UKRAINE REPUBLIC KAZAKHSTAN SLOVAK REP. MONGOLIA LIECHTENSTEIN AUSTRIA Laws SWITZERLAND HUNGARY MOLDOVA SLOVENIA FRANCE CROATIA ROMANIA ITALY SAN BOSNIA SERBIA MONACO MARINO HERZ. DEM. PEOPLE’S MONTENEGRO BULGARIA UNITED STATES ANDORRA KOSOVO GEORGIA UZBEKISTAN KYRGYZSTAN REP. OF KOREA How many women of reproductive age N. MACEDONIA PORTUGAL ALBANIA ARMENIA AZERBAIJAN SPAIN TURKMENISTAN REP. OF JAPAN TURKEY TAJIKISTAN KOREA live in countries under each category? CHINA MALTA GREECE CYPRUS SYRIA LEBANON AFGHANISTAN WEST BANK/GAZA STRIP MOROCCO TUNISIA IRAN ISRAEL IRAQ JORDAN KUWAIT NEPAL PAKISTAN BHUTAN BAHAMAS ALGERIA LIBYA QATAR MEXICO EGYPT BAHRAIN CUBA WEST SAUDI ARABIA BANGLADESH TAIWAN SAHARA UAE INDIA HONG KONG OMAN MYANMAR DOMINICAN REPUBLIC LAOS SAINT KITTS AND NEVIS MAURITANIA III BELIZE HAITI MALI JAMAICA PUERTO ANTIGUA AND BARBUDA NIGER RICO SUDAN THAILAND PHILIPPINES HONDURAS DOMINICA CAPE VERDE II 237 MILLION ERITREA YEMEN GUATEMALA SAINT VINCENT AND THE GRENADINES CHAD NICARAGUA SAINT LUCIA SENEGAL EL SALVADOR ARUBA BARBADOS GAMBIA CAMBODIA 359 MILLION 14% CURAÇAO BURKINA GRENADA GUINEA-BISSAU FASO DJIBOUTI VIETNAM COSTA RICA PANAMA TRINIDAD AND TOBAGO GUINEA BENIN MARSHALL ISLANDS 22% MICRONESIA NIGERIA SOMALIA SRI LANKA VENEZUELA ETHIOPIA SIERRA LEONE COTE TOGO CENTRAL D’IVOIRE SOUTH PALAU SURINAME GHANA AFRICAN SUDAN BRUNEI DARUSSALAM GUYANA LIBERIA REP. CAMEROON MALAYSIA COLOMBIA KIRIBATI MALDIVES EQUATORIAL GUINEA UGANDA SINGAPORE WOMEN OF SAO TOME AND PRINCIPE 90 MILLION IV DEM.