Estimation of Non-Point Source BOD Loading in Urban Area
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
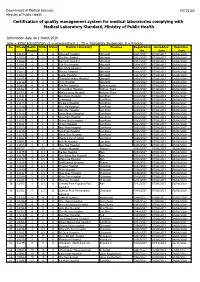
Certification of Quality Management System for Medical Laboratories Complying with Medical Laboratory Standard, Ministry of Public Health
Department of Medical Sciences F0715102 Ministry of Public Health Certification of quality management system for medical laboratories complying with Medical Laboratory Standard, Ministry of Public Health Information date on 1 March 2019 new = initial accreditation, r1 = reassessment 1 , TS = Temporary Suspension, P = Process No. HCode Health RMSc Status Medical Laboratory Province Registration Accredited Expiration Region No. Date Date 1 10673 2 2 r1 Uttaradit Hospital Uttaradit 0001/2557 07/08/2017 06/08/2020 2 11159 2 2 r1 Tha Pla Hospital Uttaradit 0002/2557 07/08/2017 06/08/2020 3 11160 2 2 r1 Nam Pat Hospital Uttaradit 0003/2557 07/08/2017 06/08/2020 4 11161 2 2 r1 Fak Tha Hospital Uttaradit 0004/2557 07/08/2017 06/08/2020 5 11162 2 2 r1 Ban Khok Hospital Uttaradit 0005/2557 07/08/2017 06/08/2020 6 11163 2 2 r1 Phichai Hospital Uttaradit 0006/2557 07/08/2017 06/08/2020 7 11164 2 2 r1 Laplae Hospital Uttaradit 0007/2557 07/08/2017 06/08/2020 8 11165 2 2 r1 ThongSaenKhan Hospital Uttaradit 0008/2557 07/08/2017 06/08/2020 9 11158 2 2 r1 Tron Hospital Uttaradit 0009/2557 07/08/2017 06/08/2020 10 10863 4 4 r1 Pak Phli Hospital Nakhonnayok 0010/2557 07/08/2017 06/08/2020 11 10762 4 4 r1 Thanyaburi Hospital Pathum Thani 0011/2557 07/08/2017 06/08/2020 12 10761 4 4 r1 Klong Luang Hospital Pathum Thani 0012/2557 07/08/2017 06/08/2020 13 11141 1 1 P Ban Hong Hospital LamPhun 0014/2557 07/08/2014 06/08/2017 14 11142 1 1 P Li Hospital LamPhun 0015/2557 07/08/2014 06/08/2017 15 11144 1 1 P Pa Sang Hospital LamPhun 0016/2557 07/08/2014 06/08/2017 -

Clinical Epidemiology of 7126 Melioidosis Patients in Thailand and the Implications for a National Notifiable Diseases Surveilla
applyparastyle “fig//caption/p[1]” parastyle “FigCapt” View metadata, citation and similar papers at core.ac.uk brought to you by CORE Open Forum Infectious Diseases provided by Apollo MAJOR ARTICLE Clinical Epidemiology of 7126 Melioidosis Patients in Thailand and the Implications for a National Notifiable Diseases Surveillance System Viriya Hantrakun,1, Somkid Kongyu,2 Preeyarach Klaytong,1 Sittikorn Rongsumlee,1 Nicholas P. J. Day,1,3 Sharon J. Peacock,4 Soawapak Hinjoy,2,5 and Direk Limmathurotsakul1,3,6, 1Mahidol-Oxford Tropical Medicine Research Unit (MORU), Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand, 2 Epidemiology Division, Department of Disease Control, Ministry of Public Health, Nonthaburi, Thailand, 3 Centre for Tropical Medicine and Global Health, Nuffield Department of Clinical Medicine, Old Road Campus, University of Oxford, Oxford, United Kingdom, 4 Department of Medicine, University of Cambridge, Cambridge, United Kingdom, 5 Office of International Cooperation, Department of Disease Control, Ministry of Public Health, Nonthaburi, Thailand, and 6 Department of Tropical Hygiene, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand Background. National notifiable diseases surveillance system (NNDSS) data in developing countries are usually incomplete, yet the total number of fatal cases reported is commonly used in national priority-setting. Melioidosis, an infectious disease caused by Burkholderia pseudomallei, is largely underrecognized by policy-makers due to the underreporting of fatal cases via the NNDSS. Methods. Collaborating with the Epidemiology Division (ED), Ministry of Public Health (MoPH), we conducted a retrospec- tive study to determine the incidence and mortality of melioidosis cases already identified by clinical microbiology laboratories nationwide. A case of melioidosis was defined as a patient with any clinical specimen culture positive for B. -
Physical Activity and Sedentary Behaviour Research in Thailand: a Systematic Scoping Review Nucharapon Liangruenrom1,2, Kanyapat Suttikasem2, Melinda Craike1, Jason A
Liangruenrom et al. BMC Public Health (2018) 18:733 https://doi.org/10.1186/s12889-018-5643-y RESEARCH ARTICLE Open Access Physical activity and sedentary behaviour research in Thailand: a systematic scoping review Nucharapon Liangruenrom1,2, Kanyapat Suttikasem2, Melinda Craike1, Jason A. Bennie3, Stuart J. H. Biddle3 and Zeljko Pedisic1* Abstract Background: The number of deaths per year attributed to non-communicable diseases is increasing in low- and middle-income countries, including Thailand. To facilitate the development of evidence-based public health programs and policies in Thailand, research on physical activity (PA) and sedentary behaviour (SB) is needed. The aims of this scoping review were to: (i) map all available evidence on PA and SB in Thailand; (ii) identify research gaps; and (iii) suggest directions for future research. Methods: A systematic literature search was conducted through 10 bibliographic databases. Additional articles were identified through secondary searches of reference lists, websites of relevant Thai health organisations, Google, and Google Scholar. Studies written in Thai or English were screened independently by two authors and included if they presented quantitative or qualitative data relevant to public health research on PA and/or SB. Results: Out of 25,007 screened articles, a total of 564 studies were included in the review. Most studies included PA only (80%), 6.7% included SB only, and 13.3% included both PA and SB. The most common research focus was correlates (58.9%), followed by outcomes of PA/SB (22.2%), prevalence of PA/SB (12.4%), and instrument validation (3.2%). Most PA/SB research was cross-sectional (69.3%), while interventions (19.7%) and longitudinal studies (2.8%) were less represented. -

1 โรงพยาบาลกรุงเทพ Bangkok General Hospital
Telephone No. Name (Thai) Name (Eng) Website Number Province Condition 1 โรงพยาบาลกรุงเทพ BANGKOK GENERAL HOSPITAL http://www.bangkokhospital.com 02 310 3000 กรุงเทพมหานคร 2 โรงพยาบาลกรุงเทพคริสเตียน BANGKOK CHRISTIAN HOSPITAL http://www.bangkokchristianhospital.org 0-2625-9000 กรุงเทพมหานคร 3 โรงพยาบาลกลวยนํ้าไท 1 KLUAYNAMTHAI 1 HOSPITAL http://www.kluaynamthai.com 0-2769-2000 กรุงเทพมหานคร 4 โรงพยาบาลกลวยนํ้าไท 2 KLUAYNAMTHAI2 HOSPITAL http://www.kluaynamthai.com 02 399 4259 กรุงเทพมหานคร 5 โรงพยาบาลเกษมราษฎร รามคําแหง KASEMRAD RAMKHAMHAENG HOSPITAL http://www.kasemrad.co.th 02 339 0000 กรุงเทพมหานคร 6 โรงพยาบาลคลองตัน KLONGTUN HOSPITAL www.klongtun-hospital.com 02 319 2101 กรุงเทพมหานคร IPD Only 7 โรงพยาบาลคามิลเลียน CAMILLIAN HOSPITAL http://www.camillianhospital.org 02 185 1444 กรุงเทพมหานคร 8 โรงพยาบาลตํารวจ POLICE GENERAL HOSPITAL www.policehospital.org 02 207 6000 กรุงเทพมหานคร IPD Only 9 โรงพยาบาลธนบุรี 1 THONBURI 1 HOSPITAL http://www.thonburihospital.com 02 487 2000 กรุงเทพมหานคร 10 โรงพยาบาลธนบุรี 2 THONBURI 2 HOSPITAL http://www.thonburi2.com 02 487 2100 กรุงเทพมหานคร 11 โรงพยาบาลนครธน NAKORNTHON HOSPITAL http://www.nakornthon.com 02 450 9999 กรุงเทพมหานคร 12 โรงพยาบาลนวมินทร NAVAMINTHRA HOSPITAL http://www.navamin9.com 02 918 5080 กรุงเทพมหานคร 13 โรงพยาบาลนวมินทร 9 NAVAMINTHRA 9 HOSPITAL http://www.navamin9.com 02 518 1818 กรุงเทพมหานคร 14 โรงพยาบาลบางนา 1 BANGNA 1 HOSPITAL - 02 746 8630 กรุงเทพมหานคร 15 โรงพยาบาลบางปะกอก 1 BANGPAKOK 1 HOSPITAL http://www.bangpakokhospital.com 02 109 1111 กรุงเทพมหานคร 16 โรงพยาบาลบางปะกอก -

No. Provider Type Status Provider Name Telephone Number Address District Province Postcode
NO. PROVIDER TYPE STATUS PROVIDER NAME TELEPHONE NUMBER ADDRESS DISTRICT PROVINCE POSTCODE BANGKOK 1 HOSPITAL PRIVATE BANGKOK GENERAL HOSPITAL 02 310 3000 2 SOI SOONVIJAI7 HUAIKHWANG BANGKOK 10320 2 HOSPITAL PRIVATE BANGKOK CHRISTIAN HOSPITAL 02 6259000 124 BANGRAK BANGKOK 10500 3 HOSPITAL GOVERNMENT WACHIRA HOSPITAL*IPD ONLY* 02 244 3000 681 DUSIT BANGKOK 10300 4 HOSPITAL PRIVATE KLUAYNAMTHAI 1 HOSPITAL 02 769 2000 80 SOI RUBIA KHLONG TOEI BANGKOK 10110 5 HOSPITAL PRIVATE KLUAYNAMTHAI2 HOSPITAL 02 399 4259 27 SOI SUKHUMVIT 68 BANGNA BANGKOK 10260 6 HOSPITAL PRIVATE KASEMRAD RAMKHAMHAENG HOSPITAL 02 339 0000 99/9 SAPHAN SUNG BANGKOK 10240 7 HOSPITAL PRIVATE KASEMRAD BANGKAE HOSPITAL 02 804 8959 240/24- 25 MOO 1 BANGKHAE BANGKOK 10160 8 HOSPITAL PRIVATE KASEMRAD PRACHACHUEN HOSPITAL 02 910 1600 950 BANGSUE BANGKOK 10800 9 HOSPITAL PRIVATE KLONGTUN HOSPITAL *IPD ONLY* 02 319 2101 3284 HUAIKHWANG BANGKOK 10320 10 HOSPITAL PRIVATE CAMILLIAN HOSPITAL 02 185 1444 423 WATTANA BANGKOK 10110 11 HOSPITAL PRIVATE CHAO PHYA HOSPITAL 02 434 1111 113/44 BANGKOK NOI BANGKOK 10700 12 HOSPITAL PRIVATE CGH PHAHOLYOTHIN HOSPITAL 02 552 8777 290 BANGKHEN BANGKOK 10220 13 HOSPITAL PRIVATE CGH SAIMAI HOSPITAL 02 991 8999 91 MOO 1 SAIMAI BANGKOK 10220 14 HOSPITAL PRIVATE SAINT LOUIS HOSPITAL 02 838 5555 215 SATHON BANGKOK 10120 15 HOSPITAL GOVERNMENT POLICE GENERAL HOSPITAL *IPD ONLY* 02 207 6000 492/1 PATHUMWAN BANGKOK 10330 16 HOSPITAL PRIVATE THEPTHARIN HOSPITAL 02 348 7000 3850 KHLONG TOEI BANGKOK 10250 17 HOSPITAL PRIVATE THAI NAKARIN HOSPITAL 02 361 2727 345 MOO 11 BANGNA BANGKOK 10260 18 HOSPITAL PRIVATE THONBURI 1 HOSPITAL 02 487 2000 34/1 BANGKOK NOI BANGKOK 10700 19 HOSPITAL PRIVATE THONBURI 2 HOSPITAL 02 487 2100 BRANCH 1 NO. -

Clinical Epidemiology of 7126 Melioidosis Patients in Thailand and the Implications for a National Notifiable Diseases Surveilla
applyparastyle “fig//caption/p[1]” parastyle “FigCapt” Open Forum Infectious Diseases MAJOR ARTICLE Clinical Epidemiology of 7126 Melioidosis Patients in Thailand and the Implications for a National Notifiable Diseases Surveillance System Viriya Hantrakun,1, Somkid Kongyu,2 Preeyarach Klaytong,1 Sittikorn Rongsumlee,1 Nicholas P. J. Day,1,3 Sharon J. Peacock,4 Soawapak Hinjoy,2,5 and Direk Limmathurotsakul1,3,6, 1Mahidol-Oxford Tropical Medicine Research Unit (MORU), Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand, 2 Epidemiology Division, Department of Disease Control, Ministry of Public Health, Nonthaburi, Thailand, 3 Centre for Tropical Medicine and Global Health, Nuffield Department of Clinical Medicine, Old Road Campus, University of Oxford, Oxford, United Kingdom, Downloaded from https://academic.oup.com/ofid/article-abstract/6/12/ofz498/5629151 by guest on 01 June 2020 4 Department of Medicine, University of Cambridge, Cambridge, United Kingdom, 5 Office of International Cooperation, Department of Disease Control, Ministry of Public Health, Nonthaburi, Thailand, and 6 Department of Tropical Hygiene, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand Background. National notifiable diseases surveillance system (NNDSS) data in developing countries are usually incomplete, yet the total number of fatal cases reported is commonly used in national priority-setting. Melioidosis, an infectious disease caused by Burkholderia pseudomallei, is largely underrecognized by policy-makers due to the underreporting of fatal cases via the NNDSS. Methods. Collaborating with the Epidemiology Division (ED), Ministry of Public Health (MoPH), we conducted a retrospec- tive study to determine the incidence and mortality of melioidosis cases already identified by clinical microbiology laboratories nationwide. A case of melioidosis was defined as a patient with any clinical specimen culture positive for B. -

Bangkok, Thailand
American Embassy Bangkok, Thailand American Citizen Services Unit 95 Wireless Road Bangkok 10330 Telephone: (66) (2) 205-4049, Fax: (66) (2) 205-4103 Website: http://bangkok.usembassy.gov MEDICAL TREATMENT IN THAILAND In an effort to better serve Americans in Thailand, the U.S. Embassy has compiled the following list of local area hospitals for the Northeast, Central, and Southern regions of Thailand. Many of the hospitals on the list are staffed by doctors with a reasonable command of English who are familiar with American medical care. In many cases, doctors have received training in the U.S. or other Western countries. Hospitals outside of the capitol may not be able to offer a wide range of English services. Please note, this list is not meant to be exhaustive or definitive, nor does it represent any guarantees of competence by the Department of State or the American Embassy. Hospitals are separated by location, with the largest number of facilities located in Bangkok. Those interested in medical care information for Northern Thailand may contact the American Consulate General in Chiang Mai by phone at (66) (53) 107-700 or by fax at (66)(53) 252-633. The Consulate General in Chiang Mai is located at 387 Vidhayanond Road. CENTRAL THAILAND BANGKOK * OFFERS 24-HOUR AMBULANCE SERVICE FACILITY FACILITY BANGKOK HOSPITAL BANGKOK CHRISTIAN HOSPITAL INTERNAT’L MEDICAL CTR. 124 SILOM ROAD 2 SOI SOONVIJAI 7 SILOM, BANGKOK NEW PETCHABURI ROAD WWW.BANGKOKCHRISTIANHOSPITAL.ORG WWW.BANGKOKHOSPITAL.COM PHONE: (66) (2) 233-6981 PHONE: (66) (2) 310-3000 FAX: (66) (2) 236-2911 FAX: (66) (2) 755-1310 BANGKOK MISSION HOSPITAL BANGKOK NURSING HOME (BNH) HOSPITAL 430 PITSANULOKE RD. -
Imrc2020bookabstract.Pdf
The 1st International Medical Student Conference 2020 1st IMRC 2020 “Moving forward together in Data Science” December 19-20, 2020 Phramongkutklao College of Medicine Bangkok, Thailand WELCOME MESSAGE Dear all delegates, On behalf of the organizing committee, it is my great pleasure and honor to cordially invite you to the 1st IMRC 2020, situated in the heart of Bangkok, Thailand. As a chairman of organizing committee, I would like to take this opportunity to thanks our keynote and invited speakers. Furthermore, I invite you to visit Bangkok, a cultural capital of Thailand. I proudly present you a unique culture and the many attractions of this metropolitan. Definitely, you will also enjoy delicious Thai food. I hope that the IMRC 2020 will be a memorable congress to benefit all the delegates. I look forward to warmly welcoming you to IMRC 2020. Maj.Gen. Surasak Tanudsintum, M.D. Dean of Phramongkutklao College of Medicine Director of Phramongkutklao Hospital Chairman of IMRC 2020 2 WELCOME MESSAGE Dear fellow medical students, As the organizing chairperson of the 1st International Medical Student Conference (IMRC 2020), I would like to express my whole-hearted welcome toward all those who are fascinated in our conference. I am enthusiastic to explore voluminous of your exceptional academic work, not only because they are initiated by medical students, but also because they illustrated how much our generation care toward the national and global health concerns. Amidst global outbreak of SARS-CoV-2, it is within our deep concern for global public health situation, we decided to hold IMRC 2020 as hybrid conference, and participants can choose to participate on-site conference or join our virtual conference online at home. -

Copy of Provider Network Oct 2020.Xlsx
รายชื&อสถานพยาบาลค่สัญญาู TPA Party Administration No. Region Province Name (Thai) Name (Eng) Telephone Number Hospital type Type Specialty Condition Remark 1 กรุงเทพและปริมณฑล กรุงเทพมหานคร คณะแพทยศาสตร์วชิรพยาบาล มหาวิทยาลัยนวมินทราธิราช WACHIRA HOSPITAL 02 244 3000 Hospital Government General IPD Only 2 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกทันตกรรมบางกอกสไมล์(อโศก) BANGKOK SMILE DENTAL CLINIC – SUKHUMVIT 21 02 664 2155 Clinic Private General OPD Only BRANCH 3 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกเวชกรรม จุฬารัตน์ 7 CHULARAT 7 CLINIC 02 328 7653 Clinic Private General OPD Only 4 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกเวชกรรม จุฬารัตน์ 8 CHULARAT 8 CLINIC 02 326 7993 Clinic Private General OPD Only 5 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกเวชกรรมกล้วยนํUาไท ชุมชน70ไร่ KLUAYNAMTHAI CLINICWECHGUM (CHUMCHON 70 RAI) 02 671 4053 Clinic Private General OPD Only 6 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกเวชกรรมกล้วยนํUาไท ทุ่งสองห้อง KLUAYNUMTHAI CLINICWECHAGUM (TUNGSONGHONG) 02 500 4296 Clinic Private General OPD Only 7 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกเวชกรรมกล้วยนํUาไท สาขา สวนเพลิน Kluaynamthai Medical Clinic, Suan Phloen Branch 02 042 6337 Clinic Private General OPD Only 8 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกเวชกรรมกล้วยนํUาไท สาขาพหลโยธิน KLUAYNAMTHAI CLINIC PAHOLYOTIN 02 115 7638 Clinic Private General OPD Only 9 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกเวชกรรมกล้วยนํUาไท สาขาอ่อนนุช KLUAYNAMTHAI CLINIC ONNUT 02 742 4398 Clinic Private General OPD Only 10 กรุงเทพและปริมณฑล กรุงเทพมหานคร คลินิกเวชกรรมกล้วยนUาไทํ สุขุมวิท56 KLUAYNAMTHAI -

The Annual Report 2017
The Annual Report 2017 Summary of the 2nd THKJR Data Analysis Meeting Contents Contents ............................................................................................................................................... 1 Preface .................................................................................................................................................. 9 Background of THKJR ........................................................................................................... 10 Role of Steering Committees in THKJR ................................................................. 13 THKJR Regional Coordinators 2016 – 2018 ....................................................... 14 Data Structure and Data Security .............................................................................. 15 Annual Report 2017 ................................................................................................................. 16 THKJR’s Next Step ................................................................................................................... 42 APPENDICES ................................................................................................................................... 43 THKJR Advisory Board ........................................................................................................ 44 Annual Activity Report 2017 – 2018 ....................................................................... 45 THKJR Steering Committees .......................................................................................... -

Recurrence and Death from Breast Cancer After Complete Treatments
Recurrence and Death from Breast Cancer after Complete Treatments: An Experience from Hospitals in Northern Thailand Rungnapa Chairat MNS*,***, Adisorn Puttisri MD**, Asani Pamarapa MD***, Nongnoot Wongrach MNS****, Chamaiporn Tawichasri MSc*****, Jayanton Patumanond MD, PhD******, Apichat Tantraworasin MD, PhD*******, Chaiyut Charoentum MD******** * PhD Program in Clinical Epidemiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand ** Department of General Surgery, Sawanpracharak Hospital, Nakorn Sawan, Thailand *** Department of General Surgery, Uttaradit Hospital, Uttaradit, Thailand **** Department of General Surgery, Lampang Hospital, Lampang, Thailand ***** Clinical Epidemiology Society at Chiang Mai, Chiang Mai, Thailand ****** Clinical Research Center, Faculty of Medicine, Thammasart University, Bangkok, Thailand ******* Department of Surgery, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand ******** Department of Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand Objective: To describe the pattern of disease progression and to describe locoregional recurrence, distant recurrence, and death rates in breast cancer patients after complete treatment. Material and Method: Medical records of women diagnosed with breast cancer at two university affiliated tertiary care hospitals in the Northern Thailand that had complete treatments between 2006 and 2010 were traced. Extracted key information included patient clinical profiles and documented recurrence of cancer. The causes of death were verified from breast cancer case registration database, death certificates through The Ministry of Internal Affairs’ civil registration, by direct telephone contact, or by distributed prepaid postcards. Results: Medical records of 829 women diagnosed with breast cancer without prior evidence of distant metastasis, and had complete recommended treatment were included. Six hundred thirty seven women had not experienced any events up to the end of the follow-up (76.8%). -

A Prospective, Longitudinal, Multicenter, Observational Study To
A Prospective, Longitudinal, Multicenter, Observational Study to Assess Insulin Treatment Patterns in Diabetic Patients in Thailand: Results from the TITAN Study Petch Rawdaree MD*, Veerasak Sarinnapakorn MD**, Somchai Pattanaungkul MD***, Weerapan Khovidhunkit MD, PhD****, Poj Tannirandorn MD*****, Thavatchai Peerapatdit MD****** * Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand ** Diabetes and Endocrinology Unit, Department of Medicine, Rajavithi Hospital, College of Medicine, Rangsit University, Bangkok, Thailand *** Division of Endocrinology and Metabolism, Department of Internal Medicine, Phramongkutklao Hospital, Bangkok, Thailand **** Division of Endocrinology and Metabolism, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand ***** Endocrinology Unit, Department of Medicine, Police General Hospital, Bangkok, Thailand ****** Division of Endocrinology and Metabolism, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective: To assess usage patterns, effectiveness, and safety of newly prescribed insulin treatment in patients with diabetes in Thailand. Material and Method: Type 1 or type 2 diabetes mellitus patients who failed achievement of HbA1c <7%, and were about to start or switch to a new insulin treatment were enrolled into this prospective, longitudinal, multicenter, observational study. Data regarding insulin usage pattern, HbA1c, fasting plasma glucose (FPG), and hypoglycemia were collected at enrollment, three and six-month. Results: Between July 2008 and February 2010, 751 patients were recruited. Mean (SD) age was 57.0 (12.8) years. Mean BMI was 26.1 (5.0) kg/m2. At enrollment, 269 (35.8%), 241 (32.1%), 206 (27.4%), and 35 (4.7%) patients were prescribed neutral protamine Hagedorn (NPH) insulin, long-acting insulin analogues (LAA), premixed insulin (Premixed), and insulin combinations, respectively.