Corner Brook Acute Care Hospital Project – Value for Money Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Community Needs and Resources Assessment for the Port Aux Basques and Burgeo Areas
PRIMARY HEALTH CARE IN ACTION A Community Needs and Resources Assessment for the Port aux Basques and Burgeo Areas 2013 Prepared by: Danielle Shea, RD, M.Ad.Ed. Primary Health Care Manager, Bay St. George Area Table of Contents Executive Summary Page 4 Community Health Needs and Resources Assessment Page 6 Survey Overview Page 6 Survey Results Page 7 Demographics Page 7 Community Services Page 8 Health Related Community Services Page 10 Community Groups Page 15 Community Concerns Page 16 Other Page 20 Focus Group Overview Page 20 Port aux Basques: Cancer Care Page 21 Highlights Page 22 Burgeo: Healthy Eating Page 23 Highlights Page 24 Port aux Basques and Burgeo Areas Overview Page 26 Statistical Data Overview Page 28 Statistical Data Page 28 Community Resource Listing Overview Page 38 Port aux Basques Community Resource Listing Page 38 Burgeo Community Resource Listing Page 44 Strengths Page 50 Recommendations Page 51 Conclusion Page 52 References Page 54 Appendix A Page 55 Primary Health Care Model Appendix B Page 57 Community Health Needs and Resources Assessment Policy Community Health Needs and Resources Assessment Port aux Basques/ Burgeo Area Page 2 Appendix C Page 62 Community Health Needs and Resources Assessment Survey Appendix D Page 70 Port aux Basques Focus Group Questions Appendix E Page 72 Burgeo Focus Group Questions Community Health Needs and Resources Assessment Port aux Basques/ Burgeo Area Page 3 Executive Summary Primary health care is defined as an individual’s first contact with the health system and includes the full range of services from health promotion, diagnosis, and treatment to chronic disease management. -

NEWFOUNDLAND and LABRADOR COLLEGE of OPTOMETRISTS Box 23085, Churchill Park, St
NEWFOUNDLAND AND LABRADOR COLLEGE OF OPTOMETRISTS Box 23085, Churchill Park, St. John's, NL A1B 4J9 Following are the names of Optometrists registered with the Newfoundland and Labrador College of Optometrists as of 1 January 2014 who hold a therapeutic drug certificate and may prescribe a limited number of medications as outlined in the following regulation: http://www.assembly.nl.ca/Legislation/sr/Regulations/rc120090.htm#3_ DR. ALPHONSUS A. BALLARD, GRAND FALLS-WINDSOR, NL DR. JONATHAN BENSE, ST. JOHN’S, NL DR. GARRY C. BEST, GANDER, NL DR. JUSTIN BOULAY, ST. JOHN’S, NL DR. LUC F. BOULAY, ST. JOHN'S, NL DR. RICHARD A. BUCHANAN, SPRINGDALE, NL DR. ALISON CAIGER-WATSON, GRAND FALLS-WINDSOR, NL DR. JOHN M. CASHIN, ST. JOHN’S, NL DR. GEORGE COLBOURNE, CORNER BROOK, NL DR. DOUGLAS COTE, PORT AUX BASQUES, NL DR. CECIL J. DUNCAN, GRAND FALLS-WINDSOR, NL DR. CARL DURAND, CORNER BROOK, NL DR. RACHEL GARDINER, GOULDS, NL DR. CLARE HALLERAN, CLARENVILLE, NL DR. DEAN P. HALLERAN, CLARENVILLE, NL DR. DEBORA HALLERAN, CLARENVILLE, NL DR. KEVIN HALLERAN, MOUNT PEARL, NL DR. ELSIE K. HARRIS, STEPHENVILLE, NL DR. JESSICA HEAD, GRAND FALLS-WINDSOR, NL 1 of 3 DR. IAN HENDERSON, ST. JOHN'S, NL DR. PAUL HISCOCK, ST. JOHN'S, NL DR. LISA HOUNSELL, ST. JOHN’S, NL DR. RICHARD J. HOWLETT, GRAND FALLS-WINDSOR, NL DR. SARAH HUTCHENS, ST. JOHN’S, NL DR. GRACE HWANG, GRAND FALLS-WINDSOR, NL DR. PATRICK KEAN, BAY ROBERTS, NL DR. NADINE KIELLEY, ST. JOHN’S, NL DR. CHRISTIE LAW, ST. JOHN’S, NL DR. ANGELA MacDONALD, SYDNEY, NS DR. -

Fire Protection and Detection Equipment Servicing Licence
Fire Protection and Detection Equipment Servicing Licence Portable Fire Extinguisher Licence FESNL-1 Company Address City Province Postal/Zip Code Licence Number Expiry Date Status Bell Aliant 332 O'Connell Drive Corner Brook NL A2H 7E5 FESNL-100000-004 June 17, 2018 Issued BMB Fire Management & Consulting 38 Gillis Drive Stephenville NL A2N 3R6 FESNL-100000-047 September 13, 2018 Issued BMS Extinguishers Ltd. P.O. Box 196 Salmon Cove NL A0A 3S0 FESNL-100000-019 June 19, 2018 Issued BP Fire & Safety P.O. Box 1957 Marystown NL A0E 2M0 FESNL-100000-045 August 29, 2018 Issued DASIT Recharging P.O. Box 649 Grand Falls-Windsor NL A2A 2K2 FESNL-125000-008 June 18, 2018 Issued DN's Canopy Cleaning 18 Byrne's Road Paradise NL A1L 3S7 FESNL-120000-015 June 19, 2018 Issued Fire-Tech Systems Ltd. P.O. Box 28105 St. John's NL A1B 4J8 FESNL-146000-032 July 17, 2018 Issued Gicleurs De La Mauricie Inc. 310 Place Nolin Trois-Rivieres QC G8T 8B5 FESNL-156000-053 March 20, 2020 Issued Gros Morne Safety Services P.O. Box 329, 121 Main Street Rocky Harbour NL A0K 4N0 FESNL-100000-006 June 17, 2018 Issued Happy Valley-Goose Bay Town Council P.O. Box 40, Station B Happy Valley-Goose Bay NL A0P 1E0 FESNL-100000-040 July 31, 2018 Issued Healey's Code Red Fire & Safety Ltd. 37 Freshwater Crescent Freshwater, PB NL A0B 1W0 FESNL-120000-009 June 18, 2018 Issued Holwell's Fire & Safety 33 Acharya Drive Paradise NL A1L 2S9 FESNL-100000-034 July 22, 2018 Issued K & D Pratt Group Inc. -

Hearing Aid Providers (Including Audiologists)
Hearing Aid Providers (including Audiologists) Beltone Audiology and Hearing Clinic Inc. 16 Pinsent Drive Grand Falls-Windsor, NL A2A 2R6 1-709-489-8500 (Grand Falls-Windsor) 1-866-489-8500 (Toll free) 1-709-489-8497 (Fax) [email protected] Audiologist: Jody Strickland Hearing Aid Practitioners: Joanne Hunter, Jodine Reid Satellite Locations: Baie Verte, Burgeo, Cow Head, Flower’s Cove, Harbour Breton, Port Saunders, Springdale, Stephenville, St. Albans, St. Anthony ________________________________ Beltone Audiology and Hearing Clinic Inc. 3 Herald Avenue Corner Brook, NL A2H 4B8 1-709-639-8501 (Corner Brook) 1-866-489-8500 (Toll free) 1-709-639-8502 (Fax) [email protected] Audiologist: Jody Strickland Hearing Aid Practitioner: Jason Gedge Satellite Locations: Baie Verte, Burgeo, Cow Head, Flower’s Cove, Harbour Breton, Port Saunders, Springdale, Stephenville, St. Albans, St. Anthony ________________________________ Beltone Hearing Service 3 Paton Street St. John’s, NL A1B 4S8 1-709-726-8083 (St. John’s) 1-800-563-8083 (Toll free) 1-709-726-8111 (Fax) [email protected] www.beltone.nl.ca Audiologists: Brittany Green Hearing Aid Practitioners: Mike Edwards, David King, Kim King, Joe Lynch, Lori Mercer Satellite Locations: Bay Roberts, Bonavista, Carbonear, Clarenville, Gander, Grand Bank, Happy Valley-Goose Bay, Labrador City, Lewisporte, Marystown, New-Wes- Valley, Twillingate ________________________________ Exploits Hearing Aid Centre 9 Pinsent Drive Grand Falls-Windsor, NL A2A 2S8 1-709-489-8900 (Grand Falls-Windsor) 1-800-563-8901 (Toll free) 1-709-489-9006 (Fax) [email protected] www.exploitshearing.ca Hearing Aid Practitioners: Dianne Earle, William Earle, Toby Penney ________________________________ Maico Hearing Service 84 Thorburn Road St. -

Immigration Portal
Immigration Portal Main Page This section of our website has been constructed to help you, the visitor to this link, to get a better idea of the lifestyle and services that Channel-Port aux Basques offers you and your families as immigrants to our community. Please log on to the various links and hopefully, you'll find the answers to your questions about Channel-Port aux Basques. In the event that you need additional information, don't hesitate to contact the Economic Development Strategist for the town at any of the following means: E-mail:[email protected] Telephone: (709) 695-2214 Fax: (709) 695-9852 Regular mail: Town of Channel-Port aux Basques 67 Main Street P.O. Box 70 Channel-Port aux Basques, NL A0M 1C0 History Channel-Port aux Basques, the Gateway to Newfoundland, has been welcoming visitors for 500 years, from Basque Fisherman in the 1500's who found the ice free harbour a safe haven, to ferry passengers who commenced arriving on the "Bruce" steamship in 1898 to take the railway across the island. The area was actually settled on a year-round basis until fisher-folk from the Channel Islands established Channel in the early 1700's, although people had been working the south coast fishery year-round for a century before this. The name Port aux Basques came into common usage from 1764 onwards following surveys of Newfoundland and undertaken by Captain James Cook on behalf of the British Admiralty. Captain Cook went on to fame, if not fortune, as a result of his surveys in the Pacific Ocean, but it was he who surveyed the St. -

8 Day Newfoundland Discovery
Tour Code NFLD 8 Day Newfoundland Discovery 8 days Created on: 29 Sep, 2021 Price Day 1: Arrive in Corner Brook, NL Arrive in Corner Brook in Newfoundland, Canada's most easterly province and also known as "The Rock". The town of Corner Brook is located on the west side of the island and renowned for its world-famous salmon bearing river, the Humber. Overnight: Corner Brook Day 2: Corner Brook - Cow Head, NL Today we explore incredible Gros Morne National Park, with its towering inland fjords and walking trails. We will learn about the geology of the area at the Gros Morne Visitor Centre and experience it first hand with a scenic walk through the Tablelands area discovering the unique flora and fauna native to the region. Moose, caribou, waterfalls and dozens of unforgettable photographic scenes add to this UNESCO World Heritage Destination. Next we visit Lobster Cove Lighthouse in Rocky Harbour and enjoy a boat cruise of Bonne Bay and participate in an age-old tradition - the "Screech In" ceremony, featuring live traditional music, a cod fish, and a taste of the famous Newfoundland Screech. Following the boat cruise, we continue up the Northern Peninsula of Newfoundland to the town of Cow Head. Overnight: Cow Head Included Meal(s): Breakfast, Lunch and Dinner Day 3: Cow Head - St. Anthony, NL This morning we travel the well-known Viking Trail Route to the most northerly tip of Newfoundland, to the L'Anse aux Meadows National Historic Site. We will see where the Vikings, the first Europeans to reach the New World, landed and established a settlement. -

Oseljh R. Smauwooll Robert D.Jv.Pill
Editor ill Chief /oselJh R. SmaUwooll pc. D,C. L,. LL D,. D, Lilt \lanaging Editor Robert D. Jv.Pill I:L A , . \1. ,A , Volunle One NEWFOUNDLAND BOOK PUBLISHERS (1967) LIMITED _.JV uVJ'LLLl/.· C:,DVlnl.~VU three and by 1940 the last family, Robinson, had moved from man's Protective Union was fonnally established in August the Cove. From 1945 to 1966 no people were reported to be 1929. living in Bottle Cove itself and the people living on the Bottle In 1920 Major Sidney Cotton qv used Botwood as a base Cove access road were included in the populaticn reported for for his pioneer work in aviation. He fonned the Aerial Survey Littleport. In the late I 960s a Martin family moved to Bottle (Newfoundland) Company there, and made important innova Cove to fish and after their home burned down their property tions in winter flying and aerial seal spOiling. His pioneer avi was sold to a Vincent family (the population of four recorded ation there was the first of its kind in Newfoundland and Can in Bottle Cove in 1971). In 1972 the Government of New ada, and, some believe. in the world . In the 1930s both the foundland expropriated land from the Darrigan family and United States and the United Kingdom explored the possibil built a picnic area and opened part of the Cove as a public ity of using Botwood as a commercial transatlantic air base. beach. In 1981 part of the beach was still used by Littleport with Ireland as the eastern terminus. -

Newfoundland & Labrador and the Iceberg Festival
Newfoundland & Labrador and the Iceberg Festival A 13 Day Tour from Corner Brook to St. John's 30 Year Exclusive Arts Club Anniversary Tour 03 - 16 June, 2022 Day 1: Friday, June 3, 2022 – Depart Vancouver on Air Canda to Deer Lake, Newfoundland Transfer from Deer Lake airport to your hotel in Corner Brook. Accommodation in Corner Brook will be at the Greenwood Inn & Suites. Day 2: Saturday, June 4, 2022 – Corner Brook Welcome to Corner Brook! It was in the nearby Bay of Islands that Captain Cook honed his surveying and cartographic skills that makes this area relevant to a significant portion of his career. Today is a totally free day for you to relax and recuperate from your long journey yesterday. (B) Cook Memorial Day 3: Sunday, June 5, 2022 – Corner Brook This morning, meet your tour director and traveling companions for a welcome breakfast followed by an orientation tour. Scenic drive along Humber Arm and the Bay of Islands en route to Frenchman’s Cove and Lark Harbour. Scenic drive returning to Corner Brook includes views of Guernsey, Tweed, and the Pearl Islands. You have free time this evening. (B) Humber Arm Frenchman’s Cove Lake Harbour Day 4: Monday, June 6, 2022 – Corner Brook – Gros Morne National Park – Port au Choix – St. Barbe Leaving Corner Brook enjoy a scenic drive along Deer Lake en route to Gros Morne National Park, a UNESCO World Heritage Site. Here visit the Lobster Cove Head lighthouse and Broom Point. In Port au Choix visit Port Au Choix National Historic Site with evidence of early indigenous habitation. -
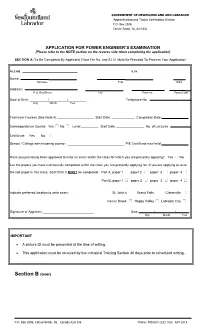
Power Engineer Exam Application
GOVERNMENT OF NEWFOUNDLAND AND LABRADOR Apprenticeship and Trades Certification Division P.O. Box 2006 Corner Brook, NL A2H 6J8 APPLICATION FOR POWER ENGINEER’S EXAMINATION [Please refer to the NOTE portion on the reverse side when completing the application] SECTION A (To Be Completed By Applicant) (Your File No. and S.I.N. Must Be Provided To Process Your Application) FILE NO. S.I.N. ___________________________________ Name: Surname First Initial Address: P.O. Box/Street City Province Postal Code Date of Birth: / / Telephone No. Day Month Year Technical Courses (See Note 4) Start Date: Completion Date: Correspondence Course: Yes No Level Start Date No. of Lectures Certificate Yes No School / College administering course: P/E Certificate now held Have you previously been approved to write an exam within the class for which you are presently applying? Yes No List the papers you have successfully completed within the class you are presently applying for. If you are applying to write the last paper in this class, SECTION C MUST be completed. Part A, paper 1 paper 2 paper 3 paper 4 Part B, paper 1 paper 2 paper 3 paper 4 Indicate preferred location to write exam: St. John’s Grand Falls Clarenville Corner Brook Happy Valley Labrador City Signature of Applicant Date / / Day Month Year IMPORTANT A picture ID must be presented at the time of writing. This application must be received by the Industrial Training Section 30 days prior to scheduled writing. Section B (over) P.O. Box 2006, Corner Brook, NL Canada A2H 6J8 Phone: 709.637-2333 Fax: 637-2519 GOVERNMENT OF NEWFOUNDLAND AND LABRADOR Apprenticeship and Trades Certification Division P.O. -

The Pre-Industrial Condition of the Forest Limits of Corner Brook Pulp and Paper Limited
THE PRE-INDUSTRIAL CONDITION OF THE FOREST LIMITS OF CORNER BROOK PULP AND PAPER LIMITED Report prepared by Corner Brook Pulp & Paper Ltd to address the requirements of the Forest Stewardship Council, National Boreal Standard 2011 THE PRE-INDUSTRIAL CONDITION OF THE FOREST LIMITS OF CORNER BROOK PULP AND PAPER LIMITED Wayne A. Brown1 and E. Doyle Wells2 1 Wayne A. Brown, BScF, RPF, (Retired) Fibre Quality & Continuous Improvement Superintendent, Corner Brook Pulp & Paper Co. Ltd., Howley, NL 2 E. Doyle Wells, PhD, (Retired) Forest Ecologist, NRCan-CFS, St. John‟s, NL THE PRE-INDUSTRIAL CONDITION OF THE FOREST LIMITS OF CORNER BROOK PULP AND PAPER LIMITED EXECUTIVE SUMMARY The purpose of this report is to provide a knowledge base of the pre-industrial conditions (PIC) of the forest limits of Corner Brook Pulp and Paper Limited from which future forest management strategies can provide direction for the maintenance of forest ecosystems in perpetuity. For the purpose of this report, the pre-industrial period covers the time before the year 1890. Prior to that time, sawmilling was common and timber was removed for firewood and lumber. However, forest utilization occurred locally around coastal communities, and the impact on forest ecosystems was minimal. The completion of the cross-Island railway in the 1890s linked communities and provided access to the vast forest resources of the interior parts of the Island. Consequently, logging and sawmilling increased dramatically. However, the establishment, in 1909, of the first paper mill in central Newfoundland coincided with the decline of the lumber industry. This was followed in 1925 by the opening of the second paper mill in Corner Brook. -

Recent Newfoundland Bird Records
RECENT NEWFOUNDLAND BIRD RECORDS LESLIE M. Tu½•c Ax.T_UOUG_UPeters and Burleigh (1951) embodiedthe results of 304 field days from 1937 to 1947 and an exhaustive search of the literature in The birds of Newfoundland,it was inevitable that additional field work would changethe known statusof many speciesin that island, and that extralimital species,especially from Europe, would continue to appear. This paper includesnotes on 51 bird species,three of them recentlyin- troducedto the island. Of 37 recordedfor the first time, four are new records for continental North America. In my capacityas ornithologistwith the CanadianWildlife Service,I have traveledwidely in Newfoundlandsince 1950; also a number of per- sonshave provided me with' carefully documentedaccounts of the birds of their areas. Spacedoes not permit me to name all the many contribu- tors who have reportedbirds to me or donated specimens,but outstand- ing are Melvin McNeill, St. Anthony; Henrik Deichmann, Badger; Mrs. H. J. Reid, Ramea; Harold Horwood and James Inder, St. John's. W. Earl Godfrey kindly reviewedan early draft of this manuscript. Cattle Egret (Bubulcus ibis ibis).--An immature came aboard the trawler Blue Foam on the Newfoundland Grand Banks 31 October 1952, and later died. It was presentedto the National Museum of Canada and was the secondspecimen for North America (Godfrey, 1954; Peterson, 1954), although the speciesis now believed to have arrived in Florida somewhat earlier. I have examined an adult shot at St. Anthony 27 October 1964, and mounted by Robert Best. Little Egret (Egretta garzetta garzetta).--An adult female was shot at Flatrock, ConceptionBay, 8 May 1954 by Robert Emerson. -
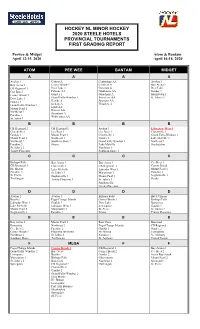
Grading Report Minor #1
HOCKEY NL MINOR HOCKEY 2020 STEELE HOTELS PROVINCIAL TOURNAMENTS FIRST GRADING REPORT Peewee & Midget Atom & Bantam April 12-15, 2020 April 16-18, 2020 ATOM PEE WEE BANTAM MIDGET A A A A Avalon 1 Cobras A Centurions AA Avalon 1 Bay Arena 1 Corner Brook 1 Crushers A Bay Arena 1 CB Regional 1 Deer Lake 1 Generals A Deer Lake Cee Bees 1 Falcons AA Gladiators AA Gander 1 Corner Brook 1 Gander 1 Guardians A Marystown 1 Deer Lake 1 Grand Falls-Windsor 1 Privateers AA St. John’s 1 Gander 1 Hawks A Spartans AA Grand Falls-Windsor 1 Jackals A Thrashes A Lynx AA Mount Pearl 1 Ravens AA Northeast 1 Scorpions A Paradise 1 Wolverines AA St. Johns 1 B B B B CB Regional 2 CB Regional 1 Avalon 1 Labrador West 1 Clarenville 1 Cee Bees 1 Cee Bees 1 Clarenville 1 Goulds 1 Mount Pearl 1 Clarenville 1 Grand Falls-Windsor 1 Mount Pearl 2 Northeast 1 Gander 1 Lake Melville 1 Northeast 2 Southern Shore 1 Grand Falls Windsor 1 Northeast 1 Paradise 2 Straits Lake Melville Sheshatshiu St. John’s 2 Northeast 1 Trinity Placentia Southern Shore 1 C C C C Bishops Falls Bay Arena 1 Bay Arena 1 Cee Bees 1 CB Regional 3 Clarenville 1 CB Regional 1 Corner Brook Hr. Breton Lake Melville Labrador West 1 Mount Pearl 1 Paradise 3 St. John’s 1 Marystown 1 Paradise 1 St. Pierre Stephenville 1 Mount Pearl 1 Stephenville 1 Twillingate Trinity Placentia 1 St. John’s 1 Straits Stephenville Trinity Placentia D D D D Avalon 2 Avalon 1 Bishops Falls Bay D’Espoir Beothic Fogo/Change Islands Corner Brook 1 Bishops Falls Labrador West 1 Goulds 1 Deer Lake Bonavista Lake Melville Labrador West 1 Lewisporte Goulds 1 Mount Pearl 3 Marystown 1 St.