REFERENCE CARD for WHO EMERGENCY UNIT FORM: TRAUMA DATES/TIMES: Do Not Leave Dates/Times Blank
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Section 9 Patient Care Record Documentation Guidelines
SECTION 9 PATIENT CARE RECORD DOCUMENTATION GUIDELINES Quick Reference Introduction to Patient Care Record Documentation 9-2 When to complete a Patient Care Record 9-3 Why use a patient Record 9-3 How to complete a Patient Record 9-3 Approaches to Documentation: System by System 9-4 Body Region 9-5 Gathering information using CHART format (System by System) 9-5 Gathering information using CHART format (Body Region) 9-6 Narrative using CHART format 9-7 Gathering information using SOAP format (System by System) 9-8 9-8 Gathering information using SOAP format (Body Region) 9-9 Narrative using SOAP format Illness and Injury Reference for Competency Sign offs 4.3 and 6.1 9-10 Introduction Patient Care Record Documentation Medavie HealthEd recognizes the need for students to provide detailed and accurate Patient Care Record Documentation. It is important for the student, school staff and preceptors to recognize the value of documenting patient care, in that it serves as a safety mechanism for the patient, as well as the practitioner. To that end, students, school staff and preceptors must develop the student‟s ability to document all aspects of the patient care they provide. Documentation provides a written record between practitioners of the assessment and treatment they have provided. This establishes greater patient safety and the smooth transition of patient care from one provider to another. In regard to the student and practitioner, accurate and detailed information on the Patient Care Record will serve as the primary record in any litigation that may be brought forward by a patient or their family. -

Inadvertent Intracranial Insertion of Nasogastric Tubes: an Overview and Nursing Implications
LITERATURE REVIEW Inadvertent Intracranial Insertion of Nasogastric Tubes: An Overview and Nursing Implications Malcolm Elliott Introduction Lecturer, Department of Nursing, Nasogastric (NG) tubes are a common medical device University of Wollongong Australia that can be used for various purposes including prevention of nausea, vomiting and gastric distension, Louise Jones Undergraduate Bachelor of Nursing student, removal of stomach contents for analysis, and lavage of University of Wollongong the stomach (Kozier, Erb, Berman & Burke 2000). Australia Other reasons for use include medication administration and enteral feeding. ABSTRACT Nasogastric tubes are a commonly used medical As with any medical device that is designed to be device. There are numerous complications inserted into the body, an NG tube can cause great associated with their use, one of the most harm with potentially fatal consequences. One such significant is when they are inadvertently consequence is when the tube is inadvertently inserted inserted into the cranium. Clinicians need into the cranium via a defect in the cranial vault. This to be aware of this complication and the type unfortunate complication may occur if clinicians are of patient who is most susceptible. not aware that it can occur or not aware of the type of KEY WORDS patient most at risk. nasogastric tubes, intracranial, complications The aim of this paper is therefore to highlight this complication of NG tube insertion so that its occurrence can be avoided. Case Reviews Various cases (see Table 1) have been reported in the literature of patients who have had an NG tube inadvertently inserted into the cranium. Investigative scans of these patients revealed that skull fractures allowed the NG tube to pass into the cranium. -

Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010
Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution 3.0 License: http://creativecommons.org/licenses/by/3.0/ We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to use, share, and adapt it. The citation key on the following slide provides information about how you may share and adapt this material. Copyright holders of content included in this material should contact [email protected] with any questions, corrections, or clarification regarding the use of content. For more information about how to cite these materials visit http://open.umich.edu/education/about/terms-of-use. Any medical information in this material is intended to inform and educate and is not a tool for self-diagnosis or a replacement for medical evaluation, advice, diagnosis or treatment by a healthcare professional. Please speak to your physician if you have questions about your medical condition. Viewer discretion is advised: Some medical content is graphic and may not be suitable for all viewers. Citation Key for more information see: http://open.umich.edu/wiki/CitationPolicy Use + Share + Adapt { Content the copyright holder, author, or law permits you to use, share and adapt. } Public Domain – Government: Works that are produced by the U.S. Government. (USC 17 § 105) Public Domain – Expired: Works that are no longer protected due to an expired copyright term. Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain. -
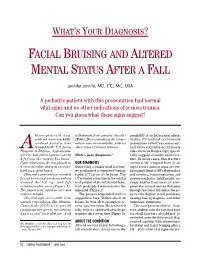
Facial Bruising and Altered Mental Status After a Fall
WHAT’S YOUR DIAGNOSIS? FACIAL BRUISING AND ALTERED MENTAL STATUS AFTER A FALL Jennifer Junnila, MD, LTC, MC, USA A pediatric patient with this presentation had normal vital signs and no other indications of serious trauma. Can you guess what these signs suggest? three-year-old boy, withdrawal from painful stimuli) possibility of an intracranial abnor- with an unremarkable (Table). The remainder of the exami- mality. Periorbital ecchymosis medical history, was nation was unremarkable, with no (sometimes called “raccoon eyes”) A brought to the U.S. Army other signs of serious trauma. and retroauricular ecchymosis Hospital at Bagram, Afghanistan (also know as Battle’s sign) specifi- after he had fallen approximately What’s your diagnosis? cally suggest a basilar skull frac- 8 ft from the roof of his home. ture. In most cases, this fracture Upon admission, he was placed in OUR DIAGNOSIS occurs at the temporal bone, lead- a cervical collar and was immobi- Suspecting a basilar skull fracture, ing to such common signs as cere- lized on a spine board. we performed a computed tomog- brospinal fluid (CSF) rhinorrhea Physical examination revealed raphy (CT) scan of the brain. The and otorrhea, hemotympanum, and facial bruising predominately CT revealed a fracture in the orbital pneumocephalus. Additionally, be- around the left eye and left roof portion of the left frontal bone, cause basilar fractures can com- retroauricular area (Figure 1). with probable extension into the press the cranial nerves that pass His pupils were equal in size and sphenoid (Figure 2). through the basal foramina, the pa- reactive to light. -

Rapid Fire Visual Diagnosis Sharpen Your Diagnostic Skills Binita R
Rapid Fire Visual Diagnosis Sharpen Your Diagnostic Skills Binita R. Shah, MD., FAAP Distinguished Professor of Emergency Medicine and Pediatrics SUNY Downstate Medical Center Brooklyn; New York Faculty Disclosure In the past 12 months, I have had the following financial relationships: The McGraw-Hill Companies, Inc. Royalties relationship Editor-in-Chief: Binita R. Shah Atlas of Pediatric Emergency Medicine; 2nd ed 2013 I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation 1 My Heartfelt Gratitude For all the children-patients and their families for allowing me to videotape and photograph these images so that we may all become better learners, pediatricians and educators ……… Learning Objectives Sharpen Your Diagnostic Skills to Recognize a variety of pediatric conditions through picture potpourri Recognize pediatric “look-alikes” conditions 2 Practice Change Reconsider diagnosis when the physical examination, laboratory findings and/or patient course do not follow the expected pattern of diagnosis First Patient An Infant with This “Rash” 3 Most likely Diagnosis 1. Child abuse (inflicted bruises) 2. Port-wine stain 3. Hemangioma 4. Neonatal lupus Port-wine Stain (Nevus Flammeus) Irregularly shaped, macular with varying hues of pink to purple Present at birth Most common location : face Usually unilateral (85%) Large lesions follow a dermatomal distribution Usually does not cross midline 4 This Infant with Port-wine Stain is MOST at Risk For A. No associated abnormalities -

Head Injury Pediatric After-Hours Version - Standard - 2017
Head Injury Pediatric After-Hours Version - Standard - 2017 DEFINITION Injuries to the head including scalp, skull and brain trauma INITIAL ASSESSMENT QUESTIONS 1. MECHANISM: "How did the injury happen?" For falls, ask: "What height did he fall from?" and "What surface did he fall against?" (Suspect child abuse if the history is inconsistent with the child's age or the type of injury.) 2. WHEN: "When did the injury happen?" (Minutes or hours ago) 3. NEUROLOGICAL SYMPTOMS: "Was there any loss of consciousness?" "Are there any other neurological symptoms?" 4. MENTAL STATUS: "Does your child know who he is, who you are, and where he is? What is he doing right now?" 5. LOCATION: "What part of the head was hit?" 6. SCALP APPEARANCE: "What does the scalp look like? Are there any lumps?" If so, ask: "Where are they? Is there any bleeding now?" If so, ask: "Is it difficult to stop?" 7. SIZE: For any cuts, bruises, or lumps, ask: "How large is it?" (Inches or centimeters) 8. PAIN: "Is there any pain?" If so, ask: "How bad is it?" 9. TETANUS: For any breaks in the skin, ask: "When was the last tetanus booster?" - Author's note: IAQ's are intended for training purposes and not meant to be required on every call. TRIAGE ASSESSMENT QUESTIONS Call EMS 911 Now [1] Major bleeding (actively dripping or spurting) AND [2] can't be stopped FIRST AID: apply direct pressure to the entire wound with a clean cloth CA: 50, 10 [1] Large blood loss AND [2] fainted or too weak to stand R/O: impending shock FIRST AID: have child lie down with feet elevated CA: 50, -

Blunt Trauma
Multisystem Trauma Objectives Describe the pathophysiology and clinical manifestations of multisystem trauma complications. Describe the risk factors and criteria for the multisystem trauma patient. Describe the nursing management of the patient recovering from multisystem trauma. Describe the collaboration with the interdisciplinary teams caring for the multisystem trauma patient. Multisystem Trauma Facts Leading cause of death among children and adults below the age of 45 4th leading cause of death for all ages Accounts for approximately 170,000 deaths each year and over 400 deaths per day Affects mostly the young and the old Kills more Americans than stroke and AIDS combined Leading cause of disability Costs: 100 billion dollars to U.S. society annually Research dollars only 4% of U.S. federal research dollars Most traumas are preventable! Who Is a Trauma Patient? Evidence-Based Categories: Physiologic Criteria Mechanism of Injury Criteria Patient/Environmental Criteria Anatomic Criteria mc.vanderbilt.edu Umm.edu Physiologic Criteria Systolic blood pressure <90mm HG Respiratory rate 10 or >29 per minute Glasgow Coma Scale score <14 Nremtacademy.com Anatomic Criteria Penetrating injuries to the head, neck, torso or proximal extremities 2 or more obvious femur or humerus fractures Amputation above the waist or ankle Crushed, de-gloved or mangled extremities Open or depressed skull fracture Unstable chest wall (flail chest) Paralysis Pelvic fracture www.pulmccrn.org Mechanism of Injury Criteria Blunt Trauma: -

Investigating and Documenting Relevant Facts Demonstrating
Demonstrating compliance with § 483.12 Investigating and Documenting Relevant Facts Objectives; briefly review the new regulatory requirements at § 483.12; “Freedom from Abuse, Neglect and Exploitation” discuss the importance of assessing common types of tissue injuries and recognize when indicators of abuse or neglect may be present identify components of an effective and consistent investigative process CMS’s focus of the NEW § 483.12 regulation is to; • ensure that residents are not subjected to abuse, neglect, misappropriation of property, and exploitation • establish requirements for the facility response to any allegations that has occurred Emphasizing that the facility must; • develop and implement written policies and procedures that prohibit and prevent abuse, neglect, misappropriation and exploitation • ensure that direct care/direct access workers are trained to recognize when treatment is abusive or when it constitutes neglect or exploitation • ensure an effective and consistent investigative processes Modified definitions • ‘‘abuse’’ includes actions such as the willful infliction of injury, unreasonable confinement, intimidation, or punishment with resulting physical harm, pain or mental anguish • ‘‘willful’’ means the individual must have acted deliberately, not that the individual must have intended to inflict injury or harm • ‘‘abuse’’ includes the deprivation by an individual of goods or services that are necessary to attain or maintain physical, mental, and psychosocial well-being • ‘‘sexual abuse’’ includes non-consensual -

Review Article
Review Article Physical signs of child abuse K. Archana1, K. R. Don2* ABSTRACT Physical abuse is nonaccidental physical injury (ranging from minor bruises to severe fractures or death) as a result of punching, beating, kicking, biting, shaking, throwing, stabbing, choking, hitting (with a hand, stick, strap, or other object), burning, or otherwise harming a child, which is inflicted by a parent, caregiver, or other person who has responsibility for the child. Such injury is considered abuse regardless of whether the caregiver intended to hurt the child. This article reviews the causes, physical signs and symptoms, risk factors, exams and tests, and prevention and treatment of child abuse. KEY WORDS: Identification, Physical child abuse, Prevention and treatment, Signs and symptoms INTRODUCTION Physical abuse involves physical aggression such as hitting, shaking, throwing, poisoning, burning or Child abuse or maltreatment constitutes all forms of scalding, drowning, suffocating, or otherwise causing physical and/or emotional ill-treatment, sexual abuse, physical harm to a child.[4] neglect or negligent treatment or commercial or other exploitation, resulting in actual or potential harm to Sexual abuse is defined as any sexual act, overt or the child’s health, survival, development or dignity in covert, between a child and an adult (or older child, the context of a relationship of responsibility, and trust where the younger child’s participation is obtained or power.[1] through seduction or coercion). Irrespective of how childhood sexual abuse is defined it generally has Child maltreatment is a considerable social and significant negative and pervasive psychological public health problem in the United States. -
Session Iv: Disaster Medical Operations — Part 2
COMMUNITY EMERGENCY RESPONSE TEAM SESSION IV: DISASTER MEDICAL OPERATIONS — PART 2 Michigan Version Revised by: Michigan Citizen Corps Council May 2003 EMERGENCY MANAGEMENT INSTITUTE NATIONAL EMERGENCY TRAINING CENTER DISASTER MEDICAL OPERATIONS SESSION IV DISASTER MEDICAL OPERATIONS—PART 2 TIME: 2 hours 30 minutes OBJECTIVES At the conclusion of this session, the participants will be able to: 1. Perform head-to-toe patient assessments. 2. Select and set up a treatment area. 3. Employ appropriate care for wounds. 4. Identify and treat fractures, sprains, and strains. 5. Take appropriate measures to maintain the public health. SCOPE ° Introduction, Review, And Session Overview ° Organization Of Disaster Medical Operations ° Conducting Head-To-Toe Assessments ° Establishing Treatment Areas ° Treating Burns ° Wound Care ° Treating Fractures, Sprains, And Strains ° Splinting ° Treating Hypothermia ° Treating Frostbite ° Public Heath Considerations ° Session Summary TRAINING The lead instructor will begin this session by welcoming the METHODS participants to Session IV: Disaster Medical Operations—Part 2, and will introduce the instructors for the session. The instructor will then present a brief review of Disaster Medical Operations— Part 1, covering the “killers” and triage procedures. Next, the instructor will present a brief overview of the topics for the session. This section will end with a presentation of the session learning objectives. IG IV-1 DISASTER MEDICAL OPERATIONS TRAINING Then the instructor will present an overview of how disaster medical METHODS operations are organized and the responsibilities of each operational (Continued) function Next, the instructor will explain and demonstrate the procedures for conducting head-to-toe patient assessments using a mannequin. The participants will then be divided into pairs so that they can practice head-to-toe patient assessments under observation. -

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse Portable Guides to Investigating Child Abuse Foreword Investigation of potential incidents of child abuse is a critical and sensitive matter. Protection of children and fairness to parents are complementary, not mutually exclusive ends. Balancing these interests is a very difficult and challenging law enforcement responsibility. It is an important part of the investigative process that physical and sexual abuse of children not be camouflaged as accidental injury. To determine whether a child’s injuries are accidental or intentional requires careful investigation, and this guide provides many practical pointers toward that end. Original Printing June 1996 Second Printing June 1997 Third Printing March 2000 Fourth Printing December 2002 NCJ 160938 n recent years the public’s increased awareness and reports of suspected child abuse have put I pressure on law enforcement to improve their investigations of such cases. This was underscored in late 1987 when a New York City toll collector observed a small girl covered with bruises in the rear of a car. The collector radioed the New York State Police, who stopped the car. The child’s foster father, an attorney, explained to police that the bruises were accidental, and he was released. A week later, the child was dead from a beating. Law enforcement personnel frequently must determine whether a child’s accident or illness was caused by a parent or caretaker. However, it is often difficult even for medical personnel to discriminate between injuries and illnesses that are accidental and those that are not. -

Markers of Physical Elder Abuse and Neglect Elearning
Markers of Physical Abuse Markers of Physical Elder how to assess for physical abuse when Abuse and Neglect interviewing a client. After completing the Markers of Physical Transfer of Learning Workbook Elder Abuse and Neglect eLearning, and By Kevin Bigelow through the use of this workbook, participants will be able to: n Adult Protective Services worker will investigate and encounter Define Physical Abuse and be able A various types of abuse including to identify various types of injuries physical abuse. It is important that the as potential indicators of abuse APS worker be aware of injuries and Identify the findings of the UCI indicators of injuries; and that they are Bruising Study and the implications able to assess what the client is saying that this may have for abuse about their injuries in the light of the investigations injuries or symptoms that can be Identify various types of physical observed. Regardless of the initial injuries as well as the symptoms allegation that begins the investigation, that may accompany various workers must always assess for physical injuries abuse. The eLearning, Markers of Physical Identify symptoms and injuries that Elder Abuse and Neglect, developed by may constitute medical the Center of Excellence at the University emergencies and may require of California at Irvine will provide valuable immediate action of the part of information on physical abuse, the types the worker of injuries that may be caused by physical Identify other types of physical abuse, how to identify these injuries, and abuse and the signs and symptoms that may accompany these types of abuse.