Dealing with Covid-19 Infections in Kolkata, India
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

India Government Mint Alipore, Kolkata, West Bengal
India Government Mint Alipore, Kolkata, West Bengal - 700053 India Ph 91-033-24010132/2401 4938 ; Fax 033-24010553 email: [email protected] EXPRESSION OF INTEREST NOTICE NO. 1 for 2019-2020 Web- https://igmkolkata.spmcil.com / e-mail- [email protected] INVITING EXPRESSION OF INTEREST (EOI) FOR APPOINTMENT OF EXPERIENCED AND REGISTERED DESIGNING FIRMS FOR PLANNING, DESIGN AND PRODUCTION WORK OF INDIA GOVERNMENT MINT MUSEUM AT KOLKATA (WEST BENGAL) General Manager, India Government Mint, Kolkata, West Bengal, invites Expression of Interest (EOI) for Appointment of experienced & registered Architect/Designing firm for Museum Interior designing, detail drawing and production work of India Government Mint, Kolkata, West Bengal and taking the approval for the following work at Alipore, Kolkata Sr. Name of Project Approximate Cost of Statutory Authority for No. interiors area project Sanction of Plans 1. Museum Interiors designing & 366 sq mts 4.4 cr India Government Mint, Work execution of India Kolkata, Government Mint West Bengal Eligibility, Qualification and Experience Criteria for Architectural Firm:- 1. The applicant should be an Architect/Designer/Design firm/Consortium of Companies. Appropriate documents supporting their status must be submitted. 2. The applicant should have an Architect, registered with the Council of Architecture with at least 5 years of experience of national & international repute. (to be supported by attested copy of registration) 3. Applicant with national/international competition projects and awarded jury member will be given preference. 4. The Applicant should have been mainly engaged in similar works, and should have worked on at least 2 projects of a similar nature in the last 4 years. -

List of Contact Person As Well As Hospitals of KPGM Policy '2017-18'
List of Contact Person as well as Hospitals of KPGM Policy ’2017-18’ Insurance Company : National Insurance Company Limited, Division – XXII, CRO – II, Kolkata-700 001. TPA : MDIndia Health Insurance TPA Pvt. Ltd. Office : 18, Lalbazar Street, Kolkata – 700 001. Phone Number : 033 – 2214 – 1936 / 1937 : Dr. Pijush Kanti Ghosh - 93320-80207 For Cashless : Mr. Soumen Jena - 99321-79757 : Dr. Sukanta Hens - 76992-23715 Reimbursement Claim : Mr. T. N. Das - 87980-85986 : 10:00 a.m. to 5:30 p.m. (Monday – Friday) Office Hours : 10:00 a.m. to 2:00 p.m. (Saturday) Claim Co-Coordinator : Mr. T. N. Das - 87980-85986 Nodal Officer, KPGM : Rabi Bhusan Paul - 94326 – 12632 KPGM Stuff : ASI - Kanchan Kr. Chowbey - 98366 - 32468 KPGM Office, Lalbazar : 033 – 2250 – 5156 List of empanelled Hospitals / Nursing Homes in Kolkata, Vellore and Districts for cashless facility for the members of Kolkata Police Group Mediclaim Policy’2017-18. K.P.G.M HOSPITAL LIST- 2017-2018 (KOLKATA) Sl. Contact Hospital Name Location Address Contact No No Person P-4&5, Gariahat Road Block-A, 033-66260000/ 1 AMRI -Dhakuria Kolkata Scheme-L11, Dhakuria, Kolkata Suvendu Pal 99030-11694 700029 230 Barakhola Lane, Purba Jadavpur, Behind Metro Cash n 033-66061041/ 2 AMRI -Mukundapur Kolkata Carry, Mukundapur, Kolkata - Dr Sukhendu 98310-65329 700099 JC - 16 & 17 Saltlake City, KB 033-66147700/ 3 AMRI -Saltlake Kolkata Block, Sector III, Kolkata - 700098 Victar Nandi 98310-13578 All Asia Medical 8B, Garcha First Lane, Beside 033-40012200/ 4 Institute (Harsh Kolkata Gariahat Pantaloons, Ballygunge, Ranjit Ukil 98305-92300 Medical) Kolkata - 700019 033-24567890/ B M Birla Heart 1, National Library Ave, Sector 1, 5 Kolkata S. -

Metro Railway Kolkata Presentation for Advisory Board of Metro Railways on 29.6.2012
METRO RAILWAY KOLKATA PRESENTATION FOR ADVISORY BOARD OF METRO RAILWAYS ON 29.6.2012 J.K. Verma Chief Engineer 8/1/2012 1 Initial Survey for MTP by French Metro in 1949. Dum Dum – Tollygunge RTS project sanctioned in June, 1972. Foundation stone laid by Smt. Indira Gandhi, the then Prime Minister of India on December 29, 1972. First train rolled out from Esplanade to Bhawanipur (4 km) on 24th October, 1984. Total corridor under operation: 25.1 km Total extension projects under execution: 89 km. June 29, 2012 2 June 29, 2012 3 SEORAPFULI BARRACKPUR 12.5KM SHRIRAMPUR Metro Projects In Kolkata BARRACKPUR TITAGARH TITAGARH 10.0KM BARASAT KHARDAH (UP 17.88Km) KHARDAH 8.0KM (DN 18.13Km) RISHRA NOAPARA- BARASAT VIA HRIDAYPUR PANIHATI AIRPORT (UP 15.80Km) (DN 16.05Km)BARASAT 6.0KM SODEPUR PROP. NOAPARA- BARASAT KONNAGAR METROMADHYAMGRAM EXTN. AGARPARA (UP 13.35Km) GOBRA 4.5KM (DN 13.60Km) NEW BARRACKPUR HIND MOTOR AGARPARA KAMARHATI BISARPARA NEW BARRACKPUR (UP 10.75Km) 2.5KM (DN 11.00Km) DANKUNI UTTARPARA BARANAGAR BIRATI (UP 7.75Km) PROP.BARANAGAR-BARRACKPORE (DN 8.00Km) BELGHARIA BARRACKPORE/ BELA NAGAR BIRATI DAKSHINESWAR (2.0Km EX.BARANAGAR) BALLY BARANAGAR (0.0Km)(5.2Km EX.DUM DUM) SHANTI NAGAR BIMAN BANDAR 4.55KM (UP 6.15Km) BALLY GHAT RAMKRISHNA PALLI (DN 6.4Km) RAJCHANDRAPUR DAKSHINESWAR 2.5KM DAKSHINESWAR BARANAGAR RD. NOAPARA DAKSHINESWAR - DURGA NAGAR AIRPORT BALLY HALT NOAPARA (0.0Km) (2.09Km EX.DMI) HALDIRAM BARANAGAR BELUR JESSOR RD DUM DUM 5.0KM DUM DUM CANT. CANT 2.60KM NEW TOWN DUM DUM LILUAH KAVI SUBHAS- DUMDUM DUM DUM ROAD CONVENTION CENTER DUM DUM DUM DUM - BELGACHIA KOLKATA DASNAGAR TIKIAPARA AIRPORT BARANAGAR HOWRAH SHYAM BAZAR RAJARHAT RAMRAJATALA SHOBHABAZAR Maidan BIDHAN NAGAR RD. -
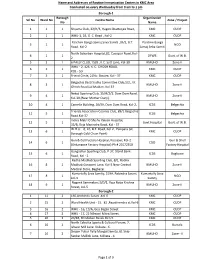
Name and Addresses of Routine Immunization Centers in KMC Area
Name and Addresses of Routine Immunization Centers in KMC Area Conducted on every Wednesday from 9 am to 1 pm Borough-1 Borough Organization Srl No Ward No Centre Name Zone / Project No Name 1 1 1 Shyama Club, 22/H/3, Hagen Chatterjee Road, KMC CUDP 2 1 1 WHU-1, 1B, G. C. Road , Kol-2 KMC CUDP Paschim Banga Samaj Seva Samiti ,35/2, B.T. Paschim Banga 3 1 1 NGO Road, Kol-2 Samaj Seba Samiti North Subarban Hospital,82, Cossipur Road, Kol- 4 1 1 DFWB Govt. of W.B. 2 5 2 1 6 PALLY CLUB, 15/B , K.C. Sett Lane, Kol-30 KMUHO Zone-II WHU - 2, 126, K. C. GHOSH ROAD, 6 2 1 KMC CUDP KOL - 50 7 3 1 Friend Circle, 21No. Bustee, Kol - 37 KMC CUDP Belgachia Basti Sudha Committee Club,1/2, J.K. 8 3 1 KMUHO Zone-II Ghosh Road,Lal Maidan, Kol-37 Netaji Sporting Club, 15/H/2/1, Dum Dum Road, 9 4 1 KMUHO Zone-II Kol-30,(Near Mother Diary). 10 4 1 Camelia Building, 26/59, Dum Dum Road, Kol-2, ICDS Belgachia Friends Association Cosmos Club, 89/1 Belgachia 11 5 1 ICDS Belgachia Road.Kol-37 Indira Matri O Shishu Kalyan Hospital, 12 5 1 Govt.Hospital Govt. of W.B. 35/B, Raja Manindra Road, Kol - 37 W.H.U. - 6, 10, B.T. Road, Kol-2 , Paikpara (at 13 6 1 KMC CUDP Borough Cold Chain Point) Gun & Cell Factory Hospital, Kossipur, Kol-2 Gun & Shell 14 6 1 CGO (Ordanance Factory Hospital) Ph # 25572350 Factory Hospital Gangadhar Sporting Club, P-37, Stand Bank 15 6 1 ICDS Bagbazar Road, Kol - 2 Radha Madhab Sporting Club, 8/1, Radha 16 8 1 Madhab Goswami Lane, Kol-3.Near Central KMUHO Zone-II Medical Store, Bagbazar Kumartully Seva Samity, 519A, Rabindra Sarani, Kumartully Seva 17 8 1 NGO kol-3 Samity Nagarik Sammelani,3/D/1, Raja Naba Krishna 18 9 1 KMUHO Zone-II Street, kol-5 Borough-2 1 11 2 160,Arobindu Sarani ,Kol-6 KMC CUDP 2 15 2 Ward Health Unit - 15. -

An Urban River on a Gasping State: Dilemma on Priority of Science, Conscience and Policy
An urban river on a gasping state: Dilemma on priority of science, conscience and policy Manisha Deb Sarkar Former Associate Professor Department of Geography Women’s Christian College University of Calcutta 6, Greek Church Row Kolkata - 700026 SKYLINE OF KOLKATA METROPOLIS KOLKATA: The metropolis ‘Adi Ganga: the urban river • Human settlements next to rivers are the most favoured sites of habitation. • KOLKATA selected to settle on the eastern bank of Hughli River – & •‘ADI GANGA’, a branched out tributary from Hughli River, a tidal river, favoured to flow across the southern part of Kolkata. Kolkata – View from River Hughli 1788 ADI GANGA Present Transport Network System of KOLKATA Adi Ganga: The Physical Environment & Human Activities on it: PAST & PRESNT Adi Ganga oce upo a tie..... (British period) a artists ipressio Charles Doyle (artist) ‘Adi Ganga’- The heritage river at Kalighat - 1860 Width of the river at this point of time Adi Ganga At Kalighat – 1865 source: Bourne & Shepard Photograph of Tolly's Nullah or Adi Ganga near Kalighat from 'Views of Calcutta and Barrackpore' taken by Samuel Bourne in the 1860s. The south-eastern Calcutta suburbs of Alipore and Kalighat were connected by bridges constructed over Tolly's Nullah. Source: British Library ’ADI Ganga’ & Kalighat Temple – an artists ipressio in -1887 PAST Human Activities on it: 1944 • Transport • Trade • Bathing • Daily Domestic Works • Performance of Religious Rituals Present Physical Scenario of Adi Ganga (To discern the extant physical condition and spatial scales) Time Progresses – Adi Ganga Transforms Laws of Physical Science Tidal water flow in the river is responsible for heavy siltation in the river bed. -

W.B.C.S.(Exe.) Officers of West Bengal Cadre
W.B.C.S.(EXE.) OFFICERS OF WEST BENGAL CADRE Sl Name/Idcode Batch Present Posting Posting Address Mobile/Email No. 1 ARUN KUMAR 1985 COMPULSORY WAITING NABANNA ,SARAT CHATTERJEE 9432877230 SINGH PERSONNEL AND ROAD ,SHIBPUR, (CS1985028 ) ADMINISTRATIVE REFORMS & HOWRAH-711102 Dob- 14-01-1962 E-GOVERNANCE DEPTT. 2 SUVENDU GHOSH 1990 ADDITIONAL DIRECTOR B 18/204, A-B CONNECTOR, +918902267252 (CS1990027 ) B.R.A.I.P.R.D. (TRAINING) KALYANI ,NADIA, WEST suvendughoshsiprd Dob- 21-06-1960 BENGAL 741251 ,PHONE:033 2582 @gmail.com 8161 3 NAMITA ROY 1990 JT. SECY & EX. OFFICIO NABANNA ,14TH FLOOR, 325, +919433746563 MALLICK DIRECTOR SARAT CHATTERJEE (CS1990036 ) INFORMATION & CULTURAL ROAD,HOWRAH-711102 Dob- 28-09-1961 AFFAIRS DEPTT. ,PHONE:2214- 5555,2214-3101 4 MD. ABDUL GANI 1991 SPECIAL SECRETARY MAYUKH BHAVAN, 4TH FLOOR, +919836041082 (CS1991051 ) SUNDARBAN AFFAIRS DEPTT. BIDHANNAGAR, mdabdulgani61@gm Dob- 08-02-1961 KOLKATA-700091 ,PHONE: ail.com 033-2337-3544 5 PARTHA SARATHI 1991 ASSISTANT COMMISSIONER COURT BUILDING, MATHER 9434212636 BANERJEE BURDWAN DIVISION DHAR, GHATAKPARA, (CS1991054 ) CHINSURAH TALUK, HOOGHLY, Dob- 12-01-1964 ,WEST BENGAL 712101 ,PHONE: 033 2680 2170 6 ABHIJIT 1991 EXECUTIVE DIRECTOR SHILPA BHAWAN,28,3, PODDAR 9874047447 MUKHOPADHYAY WBSIDC COURT, TIRETTI, KOLKATA, ontaranga.abhijit@g (CS1991058 ) WEST BENGAL 700012 mail.com Dob- 24-12-1963 7 SUJAY SARKAR 1991 DIRECTOR (HR) BIDYUT UNNAYAN BHAVAN 9434961715 (CS1991059 ) WBSEDCL ,3/C BLOCK -LA SECTOR III sujay_piyal@rediff Dob- 22-12-1968 ,SALT LAKE CITY KOL-98, PH- mail.com 23591917 8 LALITA 1991 SECRETARY KHADYA BHAWAN COMPLEX 9433273656 AGARWALA WEST BENGAL INFORMATION ,11A, MIRZA GHALIB ST. agarwalalalita@gma (CS1991060 ) COMMISSION JANBAZAR, TALTALA, il.com Dob- 10-10-1967 KOLKATA-700135 9 MD. -

Master Hira Buyers Agreement Format
1 MASTER HIRA BUYERS AGREEMENT FORMAT Modified on 28.03.19 CHANDITALA AGREEMENT FOR SALE This agreement for sale (“Agreement”) executed on this _____day of _______,20____. By and Between (1) SHAH PROJECTS PRIVATE LIMITED(PAN AABCN2989H) a Company incorporated under the Companies Act, 1956 having its registered office at No.1, Sardar Sankar Road , P.S Tollygunge, P.O Kalighat, Kolkata -700026, represented by its Director, Sri Rajiv Shah(PAN: ALJPS6781N), son of Sri Gyarsi Lal Shah, working for gain at No.1, Sardar Sankar Road, P.S Tollygunge, P.O Kalighat, Kolkata - 700026 (2) SRI.RAJIV SHAH(PAN ALJPS6781N), son of Sri Gyarsi Lal Shah, residing at 16/8, Mandal Temple Lane, Block-P, P.O. New Alipore, P.S New Alipore, Kolkata -700053 (3) SMT. NISHA SHAH(PAN AMAPS5067K) Wife of Sri Rajiv Shah, residing at 16/8, Mandal Temple Lane, Block-P, P.O. New Alipore, P.S New Alipore, Kolkata -700053, (4) SRI SAURAV SHAH (PAN: AMAPS3643P)son of Sri Rajiv Shah, residing at 16/8, Mandal Temple Lane, Block-P, P.O. New Alipore, P.S New Alipore, Kolkata -700053 (5) SMT. SHWETA SHAH(PAN: AHDPM6429R), Wife of Sri Saurav Shah (6) SRI MAYANKH SHAH (PAN: AJIPS8151M), and (7) SMT. SWETA SHAH(PAN: ACZPA9574G), wife of Sri Mayankh Shah, residing at 16/8, Mandal Temple Lane, Block-P, P.O. New Alipore, P.S New Alipore, Kolkata -700053 all of whom represented by 2 Mr.__________ (PAN_______) son of _________ (Mobile No._________) residing at ________________ hereinafter jointly referred to as the OWNERS (which expression shall unless excluded by or repugnant to the subject or context be deemed to mean and include in respect of the companies their respective successor or successors-in- interest and assigns and in respect of the individuals their respective heirs, legal representatives and assigns) of the FIRST PART AND SRIJAN REALTY PRIVATE LTD. -

Date Wise Details of Covid Vaccination Session Plan
Date wise details of Covid Vaccination session plan Name of the District: Darjeeling Dr Sanyukta Liu Name & Mobile no of the District Nodal Officer: Contact No of District Control Room: 8250237835 7001866136 Sl. Mobile No of CVC Adress of CVC site(name of hospital/ Type of vaccine to be used( Name of CVC Site Name of CVC Manager Remarks No Manager health centre, block/ ward/ village etc) Covishield/ Covaxine) 1 Darjeeling DH 1 Dr. Kumar Sariswal 9851937730 Darjeeling DH COVAXIN 2 Darjeeling DH 2 Dr. Kumar Sariswal 9851937730 Darjeeling DH COVISHIELD 3 Darjeeling UPCH Ghoom Dr. Kumar Sariswal 9851937730 Darjeeling UPCH Ghoom COVISHIELD 4 Kurseong SDH 1 Bijay Sinchury 7063071718 Kurseong SDH COVAXIN 5 Kurseong SDH 2 Bijay Sinchury 7063071718 Kurseong SDH COVISHIELD 6 Siliguri DH1 Koushik Roy 9851235672 Siliguri DH COVAXIN 7 SiliguriDH 2 Koushik Roy 9851235672 SiliguriDH COVISHIELD 8 NBMCH 1 (PSM) Goutam Das 9679230501 NBMCH COVAXIN 9 NBCMCH 2 Goutam Das 9679230501 NBCMCH COVISHIELD 10 Matigara BPHC 1 DR. Sohom Sen 9435389025 Matigara BPHC COVAXIN 11 Matigara BPHC 2 DR. Sohom Sen 9435389025 Matigara BPHC COVISHIELD 12 Kharibari RH 1 Dr. Alam 9804370580 Kharibari RH COVAXIN 13 Kharibari RH 2 Dr. Alam 9804370580 Kharibari RH COVISHIELD 14 Naxalbari RH 1 Dr.Kuntal Ghosh 9832159414 Naxalbari RH COVAXIN 15 Naxalbari RH 2 Dr.Kuntal Ghosh 9832159414 Naxalbari RH COVISHIELD 16 Phansidewa RH 1 Dr. Arunabha Das 7908844346 Phansidewa RH COVAXIN 17 Phansidewa RH 2 Dr. Arunabha Das 7908844346 Phansidewa RH COVISHIELD 18 Matri Sadan Dr. Sanjib Majumder 9434328017 Matri Sadan COVISHIELD 19 SMC UPHC7 1 Dr. Sanjib Majumder 9434328017 SMC UPHC7 COVAXIN 20 SMC UPHC7 2 Dr. -

Kalighat for 21St Century
CONCEPT SCHEME KALIGHAT FOR 21ST CENTURY INTERNATIONAL FOUNDATION FOR SUSTAINABLE DEVELOPMENT IN ASSOCIATION WITH THE BOSTON PLEDGE, USA AND GOVT. OF WEST BENGAL PRESENTATION BY MODULAR CONSULTANTS (P) Ltd. Prime Consultant MCPL IFSD SCOPE OF WORK Census & public enlightenment Renovation programme for existing occupiers / services provides in the redevelopment area Restructure of vehicular traffic Open / covered walk-track to Kali Temple Dredging & embankment protection of Adi Ganga upto Sluise Gate and connect the River Cruise from Sahara’s proposed Embarkation Jetty near Outram Ghat Construction of Foot Bridge over Adi Ganga Reconstruction of Adi Ganga Bathing Ghat Beautification of existing façade Rejuvenating the Craftsmanship of Patuas Travellers’ / Tourists’ Amenities Modernization of Kali Temple Water supply system including treatment plant Sewerage Disposal Solid waste management system Environment Management Plan Electricity supply and distribution system MCPL IFSD STATEMENT OF INTENT 1. Clean existing scum, filth and slummy environment of the temple area. 2. Remove and rehabilitate existing street vendors and street stalls. 3. Remove and rehabilitate stalls directly attached to the inside and outside of the temple compound walls and areas. Temple footprint should be free of any obstruction. Fresh paint on temple structure needed. 4. Incorporate spiritual AXES, NUMBERS and DIAGRAMS in new configuration of design elements brought into the proposed scheme. 5. Use pure forms and forms reminiscent of the main temple roof in new design elements as much as possible. 6. Create a SENSE OF PILGRIMAGE in the area. 7. Use Kali Temple Road as the MAIN AXIS to approach the temple. 8. Build FOUR gates on four perimeter roads of the ward. -

3 Bedroom Apartment / Flat for Rent in Ambuja Upohar the Condoville
https://www.propertywala.com/P61353197 Home » Kolkata Properties » Residential properties for rent in Kolkata » Apartments / Flats for rent in Chak Garia, Kolkata » Property P61353197 3 Bedroom Apartment / Flat for rent in Ambuja Upohar The Condoville, C… 45,000 3BHK Apartment In Ambuja Upohar The Advertiser Details Condoville 2052,Ambuja Upohar The Condoville, Chak Garia, Kolkat… Project/Society: Ambuja Upohar The Condoville Area: 193.15 SqMeters ▾ Bedrooms: Three Bathrooms: Three Monthly Rent: 45,000 Rate: 233 per SqMeter -5% Available: Immediate/Ready to move Scan QR code to get the contact info on your mobile Description View all properties by Mishra Enterprise 3 bhk flat available for rent in e m bypass, kolkata south. It is located in ambuja upohar the condoville, which is a very good society. The space is semifurnished, located on 9th floor of 18 floors. It has 3 Pictures bedrooms, 3 bathrooms and 2 balcony(S). The flat is built on the principles of feng-Shui/vaastu. It is an ideal accommodation for all and has a super built-Up area of 2079 sq. Ft. It includes 3 wardrobe(S), 1 modular kitchen, 4 ac(S), 3 geyser(S), 6 fan(S), 18 light(S), 1 curtain(S), 1 chimney(S) and 1 exhaust fan(S) and has facilities like intercom facility, lift(S), park, maintenance staff, visitor parking, water storage and security/fire alarm etc. In addition, it has vitrified flooring. It is a 5-10 year old property. Since it is located in a gated society, you can be assured of security. The flat is north facing. -

Reclaiming the Indigenous Style of Kalighat Paintings Lauren M. Slaughter
Reclaiming the Indigenous Style of Kalighat Paintings Lauren M. Slaughter This essay re-examines the nature of Kalighat painting, a painting style which emerged in India in the early nineteenth century and ended not long after the early twentieth century. Stemming from traditional Indian scroll painting, Kalighat paintings were created by patuas who migrated from Bengal villages into Calcutta and set up their “shop- studios” around the Kalighat temple (Guha-Thakurta, Making 17; Jain 9). Patuas represent a caste of traveling scroll-painters and performers; the earliest mention of this artisan caste appears in Brahma Vaivarta Purana, a thirteenth-century Sanskrit text (Chatterjee 50). As a result of W. G. Archer’s 1953 Bazaar Paintings of Calcutta: The Style of Kalighat, the general consensus of scholarly literature suggests that Kalighat painting reflects a western influence on thepatua artists. In line with the work of Tapati Guha-Thakurta and B.N. Mukherjee, however, I want to argue that there is not enough evidence to support the claim that this style was shaped by contact with western painting; instead I will argue that it was essentially indigenous in style, medium, and subject matter. Because stating that Kalighat paintings are British-derived diminishes their value and robs these works of their true substance, my aim is to substantiate their indigenous origins and, in so doing, explain how this re-interpretation provides new ways of understanding the innovative style of Kalighat patuas. Chrestomathy: Annual Review of Undergraduate Research, School of Humanities and Social Sciences, School of Languages, Cultures, and World Affairs, College of Charleston Volume 11 (2012): 242-258 © 2012 by the College of Charleston, Charleston SC 29424, USA. -

West Bengal Human Rights Commission Bhabani Bhavan, 2Nd Floor, Alipore, Kolkata - 27
West Bengal Human Rights Commission Bhabani Bhavan, 2nd Floor, Alipore, Kolkata - 27. 682/WBHRC/Com/11-12 Date : 17.08.12 Present :. 1. Justice Asok Kumar Ganguly .. Chairperson 2. Justice N.C. Sil .. Member 3. Shri S.N. Roy .. Member Justice N.C. Sil, member of this Commission had visited the Male vagrants’ Home, Bangaon, Petrapole on 01.07.12. At the time of his inspection, Sri Abhijit Bhattacharjee, SDO, Bangaon, Sri Swadesh Mondal, Deputy Magistrate, Bangaon and Sri Mihir Kr. Saha, Manager of the Home were also present. A detailed report of his inspection which was circulated before the Commission was submitted by him. A copy of the said inspection report is enclosed herewith. Now, in view of the inspection of Justice N.C. Sil, the following recommendations are being made: 1. The inmates who give their address and want to go back to their family be sent back to their home after verification of the correctness of the address. 2. The Home authorities are required to keep vigil so that no inmate can escape from the Home 3. Govt. should take steps to provide adequate staff particularly cook for the Home 4. There should be cots for the inmates in order to avert further deterioration of their health. 5. Adequate medical facilities should be provided for the inmate in the Home. 6. Government should consider to augment fund for the upkeeping of inmates. The Govt. should inform the Commission within a period of two months from the date of receipt of these recommendations as to the action taken or proposed to be taken in this regard.