Dietary Reference Intakes for Water, Potassium, Sodium, Chloride
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Moringa Oleifera 31.05.2005 8:55 Uhr Seite 1
Moringa oleifera 31.05.2005 8:55 Uhr Seite 1 Moringa oleifera III-4 Moringa oleifera LAM., 1785 syn.: Guilandina moringa LAM.; Hyperanthera moringa WILLD.; Moringa nux-ben PERR.; Moringa pterygosperma GAERTN., 1791 Meerrettichbaum, Pferderettichbaum Familie: Moringaceae Arabic: rawag Malayalam: murinna, sigru Assamese: saijna, sohjna Marathi: achajhada, shevgi Bengali: sajina Nepali: shobhanjan, sohijan Burmese: daintha, dandalonbin Oriya: sajina Chinese: la ken Portuguese: moringa, moringueiro English: drumstick tree, Punjabi: sainjna, soanjna horseradish tree, ben tree Sanskrit: shobhanjana, sigru French: moringe à graine ailée, Sinhalese: murunga morungue Spanish: ángela, ben, moringa Gujarati: midhosaragavo, saragavo Swahili: mrongo, mzunze Hindi: mungna, saijna, shajna Tamil: moringa, murungai Kannada: nugge Telegu: mulaga, munaga, Konkani: maissang, moring, tellamunaga moxing Urdu: sahajna Fig. 1: Flower detail (front and side view) Enzyklopädie der Holzgewächse – 40. Erg.Lfg. 6/05 1 Moringa oleifera 31.05.2005 8:55 Uhr Seite 2 Moringa oleifera III-4 Drumstick tree, also known as horseradish tree and ben It is cultivated and has become naturalized in other parts tree in English, is a small to medium-sized, evergreen or of Pakistan, India, and Nepal, as well as in Afghanistan, deciduous tree native to northern India, Pakistan and Bangladesh, Sri Lanka, Southeast Asia, West Asia, the Nepal. It is cultivated and has become naturalized well Arabian peninsula, East and West Africa, throughout the beyond its native range, including throughout South Asia, West Indies and southern Florida, in Central and South and in many countries of Southeast Asia, the Arabian Pe- America from Mexico to Peru, as well as in Brazil and ninsula, tropical Africa, Central America, the Caribbean Paraguay [17, 21, 29, 30, 51, 65]. -

Guideline for Dietary Fibre Intake
Guideline for dietary fibre intake Gezondheidsraad Health Council of the Netherlands To the Minister of Health, Welfare and Sport Subject : Presentation of advisory report Guideline for dietary fibre intake Your reference:- Our reference : U 383/CS/cn/754-C Enclosures : 1 Date : March 21, 2006 Dear Minister, I hereby present an advisory report concerning the Guideline for Dietary Fibre Intake, which has been prepared, at the request of my predecessor Professor JGAJ Hautvast, by the Health Council's Committee on Dietary Fibre and reviewed by the Standing Committee on Nutrition and the Standing Committee on Medicine. I have today also presented this report to the Minister of Agriculture, Nature and Food Quality. This is the fourth in a series of advisory reports designed to revise the Dutch dietary ref- erence intakes (Nederlandse Voedingsnormen), which were adopted in 1992 by the former Food and Nutrition Council (Voedingsraad). Dietary fibre received very little attention in that report, however. The advisory report Guidelines for a Healthy Diet (Richtlijnen Goede Voeding), which was published by the Food and Nutrition Council in 1986 and is currently being revised, also included a very brief passage about dietary fibre. The attached advisory report is therefore the first thorough evaluation of the physiological effects of dietary fibre to have been undertaken in the Netherlands. The Committee has chosen not to set a dietary reference intake for fibre, but instead to issue a guideline. This decision is motivated by the fact that dietary fibre is the collective term for a group of substances with very wide-ranging physiological effects. -

Suppression Mechanisms of Alkali Metal Compounds
SUPPRESSION MECHANISMS OF ALKALI METAL COMPOUNDS Bradley A. Williams and James W. Fleming Chemistry Division, Code 61x5 US Naval Research Lnhoratory Washington, DC 20375-5342, USA INTRODUCTION Alkali metal compounds, particularly those of sodium and potassium, are widely used as fire suppressants. Of particular note is that small NuHCOi particles have been found to be 2-4 times more effective by mass than Halon 1301 in extinguishing both eountertlow flames [ I] and cup- burner flames [?]. Furthermore, studies in our laboratory have found that potassium bicarbonate is some 2.5 times more efficient by weight at suppression than sodium bicarhonatc. The primary limitation associated with the use of alkali metal compounds is dispersal. since all known compounds have very low volatility and must he delivered to the fire either as powders or in (usually aqueous) solution. Although powders based on alkali metals have been used for many years, their mode of effective- ness has not generally been agreed upon. Thermal effects [3],namely, the vaporization of the particles as well as radiative energy transfer out of the flame. and both homogeneous (gas phase) and heterogeneous (surface) chemistry have been postulated as mechanisms by which alkali metals suppress fires [4]. Complicating these issues is the fact that for powders, particle size and morphology have been found to affect the suppression properties significantly [I]. In addition to sodium and potassium, other alkali metals have been studied, albeit to a consider- ably lesser extent. The general finding is that the suppression effectiveness increases with atomic weight: potassium is more effective than sodium, which is in turn more effective than lithium [4]. -

Asparagus
Give Your Family More of the Good Stuff! Asparagus Basics $ and $ n excellent sourc hop ave is a e of V gus ita < Look for stalks that are firm ra ps build stro m a hel ng bo in with tightly closed tips. Color sp ich ne K A wh s. , can be bright green, creamy white or even purple. < Stalks with the same thickness will cook in the same amount of time. < Fresh asparagus may be best Types of quality and lowest price when harvested locally, usually April Asparagus and May. Generally, thinner spears are < Asparagus is also available more delicate and tender; canned and frozen. thicker spears have stronger flavor and hearty texture. Asparagus Math: Thicker spears can be sliced on the diagonal into smaller One pound = 12 to 15 spears, pieces to cook more quickly. 9 to 10 inches long and 1/2 < Green – the most common to 3/4 inches thick type. = 3 cups trimmed < White – covered with soil as it grows to keep green 1 = 2 /2 cups cooked pigments from developing. Considered a delicacy and may cost more than green. tore Well < Purple – has more sugar and S less fiber than green. The skin aste Less is burgundy or purple but the W flesh is pale green to creamy I Refrigerate fresh asparagus for up white. Cooking may cause I to 5 days. Wash under cool running water more green to show. Less • Stand stalks in 1 inch of water just before using. Remove tough ends: commonly available and may like a flower bouquet and cover • Hold an end of the stalk in each cost more than green. -

Nutrition Guideline: Vitamins and Minerals
Nutrition Guideline For Professional Reference Only Vitamins and Minerals Applicable to: Nurses, Physicians and Other Health Professionals Recommendations Most individuals can meet their vitamin and mineral needs by healthy eating using Canada’s Food Guide. The following strategies can help an individual achieve appropriate intakes of vitamins and minerals: • Choosing a variety of foods from all four food groups of Canada’s Food Guide every day and eating the recommended number of servings from each food group every day. • Choosing meals that include at least three of the four food groups. • For adults: Eating three regular meals, and snacks if needed, throughout the day. • For children: Providing three regular meals and two to three snacks every day. Provide snacks that include foods from Canada’s Food Guide. • Considering taking a vitamin or mineral supplement if you are not meeting the recommended number of servings of each food group from Canada’s Food Guide. Ask for advice from your physician or health care provider. The following people need to take vitamin or mineral supplements: o Women who are pregnant, breastfeeding, or who could become pregnant, need a multivitamin containing folic acid and vitamin B12 every day. o Pregnant women need to ensure that their multivitamin contains iron. o Refer to the guideline Calcium and Vitamin D for recommendations about vitamin D supplementation • Recognizing that single-nutrient supplements carry a higher risk of adverse reactions. Seek referral to a physician or Registered Dietitian if you are considering taking one. • Notifying your physician or Registered Dietitian if you take a multivitamin-mineral, herbal or any other type of nutrition supplement. -

Asparagus Densiflorus 'Sprengeri'
FPS051 Asparagus densiflorus ‘Sprengeri’ Sprengeri Asparagus Fern1 Edward F. Gilman, Ryan W. Klein, and Gail Hansen2 Introduction ‘Sprengeri’ Asparagus Fern is a rounded herbaceous perennial that is used in the landscape for its attractive, fine-textured foliage. This 1 to 4 foot-tall plant has true leaves that are scale-like and inconspicuous. The structures that most refer to as leaves are actually leaf-like branchlets called cladophylls. These tiny cladophylls are linear, flat- tened structures that are bright green in color. They occur singly or in groups of 3 or more at a node. The stems of this plant emerge directly from the ground and become woody and spiny, so be careful when handling this species. The thorns cause significant irritation to many people Figure 1. Full form—Asparagus densiflorus: ‘Sprengeri’ Sprengeri that handle the plant. Pretty, red, ovoid berries occur on asparagus fern. Asparagus densiflorus throughout the year. Several birds eat Credits: Edward F. Gilman, UF/IFAS and probably distribute the fruit. These fruits follow tiny, General Information white, flowers that occur in axillary racemes; the flowers are inconspicuous for the most part but fragrant. Seeds Scientific name: Asparagus densiflorus ‘Sprengeri’ germinate in the landscape and the plant has escaped into Pronunciation: ass-SPAR-uh-gus den-sif-FLOR-us natural habitats in parts of Florida. It can also become a Common name(s): ‘Sprengeri’ asparagus fern weed in your landscape. Family: Liliaceae Plant type: herbaceous; perennial USDA hardiness zones: 9B through 11 (Figure 2) Planting month for zone 7: year round Planting month for zone 8: year round Planting month for zone 9: year round Planting month for zone 10 and 11: year round Origin: not native to North America Invasive potential: potentially invasive 1. -
Fasciation. Lumina C
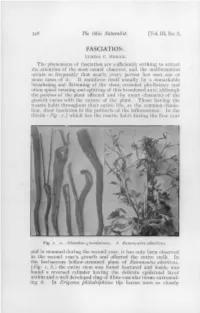
346 The Ohio Naturalist. [Vol. III, No. 3, FASCIATION. LUMINA C. RIDDLE. The phenomena of fasciation are sufficiently striking to attract the attention of the most casual observer, and the malformation occurs so frequently that nearly every person has seen one or more cases of it. It manifests itself usually by a remarkable broadening and flattening of the stem, crowded phyllotaxy and often spiral twisting and splitting of this broadened axis, although the portion of the plant affected and the exact character of the growth varies with the nature of the plant. Those having the rosette habit throughout their entire life, as the common dande- lion, show fasciation in the peduncle of the inflorescence. In the thistle (Fig. 2,) which has the rosette habit during the first year Fig. 1. a. Ailanthus glandulosus. b. Ranunculus abortivus, and is stemmed during the second year, it has only been observed in the second year's growth and affected the entire stalk. In the herbaceous hollow-stemmed plant of Ranunculus abortivus, {Fig. 1, b,) the entire stem was found fasciated and inside was found a reversed cylinder having the delicate epidermal layer within and a well developed ring of fibro-vascular tissue surround- ing it. In Erigeron philadelphicus the leaves were so closely Jan., 1903.] Fasciation. 347 compacted that the stem was entirely concealed while the top of the stalk was twisted down. In woody plants fasciated stems are nearly always split or twisted, often both, as shown in Ailanthus glandidosus {Fig. i, a.) Fasciation is found frequently occurring in man}- cultivated plants; the flowers, hyacinths, gladioli, narcissus, violets, gerani- u m s , nasturtiums ( Tropoeolum); the garden vegetables, cabbage or Brassica oleracea, and beets, Beta vulgaris ; and trees, Pinus, Thuya, Taxus, Salix, Alnus,Ulmus, Prunus and Populus. -

(Asparagus Officinalis): a Source of Developmental, Chemical and Urinary Intrigue
Supplementary Material Green and white asparagus (Asparagus officinalis): A Source of Developmental, Chemical and Urinary Intrigue Eirini Pegiou 1, Roland Mumm 2, Parag Acharya 3, Ric C.H. de Vos 2, Robert D. Hall 1,2,4,* 1 Wageningen University & Research, Laboratory of Plant Physiology, P.O. Box 16, 6700AA Wageningen, The Netherlands; [email protected] 2 Wageningen University & Research, Business Unit Bioscience, P.O. Box 16, 6700AA Wageningen, The Netherlands; [email protected] (R.M.); [email protected] (R.C.H.d.V.) 3 Unilever Foods Innovation Centre, Bronland 14, 6708WH Wageningen, The Netherlands; [email protected] 4 Netherlands metabolomics Centre, Einsteinweg 55, 2333CC Leiden, The Netherlands * Correspondence: [email protected] Supplementary Tables Table S1: List of non-volatile secondary metabolites detected and reported in A. officinalis (green and/or white) materials (when not indicated, this was not reported in the article and green can be assumed). For the description of the analytical techniques the following codes apply; the separation or ionization technique (HPLC: high performance liquid chromatography, MALDI: matrix assisted laser desorption/ionization) and the detector (MS: mass spectrometry, UV: ultraviolet, NMR: nuclear magnetic resonance, I: imaging) (MW: molecular weight in g/mol, FW: fresh weight, DW: dry weight). Analytical Detected secondary metabolite, Asparagus material (reported technique Molecular formula (MW) concentration) (Reference) Polyphenols Flavonoids quercetin-3-O-rutinoside Green spears -

Plan for Notifying Employees Not to Report to Work
PLAN FOR NOTIFYING EMPLOYEES NOT TO REPORT TO WORK The Hanford Administrative Committee, in accordance with Article XIII, Section 4., has determined that the following plan will be implemented by the EMPLOYER for the purpose of notifying employees covered by the Hanford Site Stabilization Agreement not to report to work. The EMPLOYER will cause an announcement to be made over local radio stations broadcasting within the Tri-Cities and Yakima areas at least two hours prior to the employees’ regular starting time advising that construction operations are closed and that the EMPLOYERS’ employees should not report to work. A general announcement will be considered to apply to all employees of the EMPLOYER, and to all activities of the EMPLOYER, except for those employees and/or activities which are specifically identified as not be affected by the announcement. Further, employees will recognize and adhere to a similar announcement issued by the OWNER, the U.S. Department of Energy, and will assume that such general announcements addressing the Hanford site and/or Hanford employees will include employees of the EMPLOYERS. The announcement will apply only to the shift immediately following the time of the announcement unless the announcement gives instructions to the contrary. Every effort will be made by the EMPLOYER (or OWNER) to get the announcement on the following radio stations: TRI-CITIES YAKIMA KALE - FM 95 KONA - AM 169 KUTI - AM 980 KZZK - FM 102.7 KORD - AM 870 KIT - AM 1280 KONA - FM 105.3 KIOK - AM 960 KHWK - FM 106.5 KOTY - AM 1340 Travel Pay Effective: 09/01/08 APPENDIX “A” HANFORD DAILY TRAVEL PAY Daily Travel Pay for Construction Crafts will be paid as follows: Area Daily Pay 300 $18.50 400 $18.50 200 East $22.00 200 West $22.75 100 (All) $23.50 Rev. -

Robert Frost Elementary Nd at the Beginning of the Year, Parents Must File an Crossing Guards Are Stationed at Pearl and 22Nd and 1915 N
EMERGENCY FORMS WALKERS/BIKE RIDERS Robert Frost Elementary nd At the beginning of the year, parents must file an Crossing guards are stationed at Pearl and 22nd and 1915 N. 22 Ave. emergency form with the office providing the emergency duties monitor students as they walk over the overpass Pasco, WA 99301 telephone numbers of the parents as well as alternate that extends over 20th Avenue. Students should observe all (509) 543-6795 persons to contact in the event the school is unable to pedestrian rules. contact the parents. Parents must notify the school if this Students may not ride skateboards, bikes, scooters or information changes during the year. roller blades over the overpass or on school grounds. Bikes and scooters should be locked up to the bike rack MEDICATION/ILLNESS located on the south side of the building. Students must We cannot give medication at school without all of the provide their own locks to secure their bikes on the bike following: rack. 1. All medication, including over the counter drugs, LOST AND FOUND must be prescribed by a licensed medical physician, osteopathic physician or dentist and left A lost and found area is located in the hallway next to in it's original container. the office. Many times articles of value are also turned into 2. Send only amount needed to take while at school, the office. As soon as a student has lost an article, they usually pharmacists will provide an extra bottle should check the lost and found area and with the office. when requested. We strongly urge that all clothing personal property be labeled with the student's name. -

Benton City Blaine Bremerton Brewster
KUJ-F CHR KCED Hot AC* Benton City 99.1 52000w 1263ft DA 91.3 1000w -72ft +New Northwest Broadcasters, LLC Centralia Community College KMMG Regional Mexican [Repeats: KDYK 1020] Sister to: KALE, KEGX, KIOK, KKSR, KTCR 360-736-9391 96.7 820w 889ft 509-783-0783 fax: 509-735-8627 600 Centralia College Blvd, 98531 +Bustos Media Corporation 830 N Columbia Center Blvd Ste B2 GM Wade Fisher Sister to: KDYK, KDYM, KZML, KZTA, KZTB Kennewick 99336 Centralia/Chehalis Market 509-457-1000 fax: 509-452-0541 GM Kurt Luchs SM Ken Olsen PO Box 2888, Yakima 98907 PD A.J. Brewster CE Mike Powers KNBQ Country 706 Butterfield Rd, Yakima 98901 www.power991fm.com 102.9 70000w 2192ft GM Ricky Tatum SM Ruben Muniz Richland/Kennewick/Pasco Arbitron 7.2 Shr 1700AQH -Clear Channel Communications PD Jesus Rosales CE Dewey Trostell 2nd market Walla Walla 206494-2000 fax: 206-286-2376 www.radlolagrande.com/yakima/ 351 Elliott Ave W Ste 300, Seattle 98119 Richland/KennewickPasco Arbitron 3.0 Shr 700 AQH GM Michele Grosenick SM Alison Hesse Burien PD Jay Kelly CE Ken Broeffle Blaine www.qcountry1029.com KGNW Religious Teaching Centralia/Chehalis Market 820 50000/5000 DA-2 KARI Religious Teaching 2nd market Seattle/Tacoma/Everett +Salem Communications Corp. 550 5000/2500 DA-2 3rd market Olympia Sister to: KKMO, KKOL, KLFE, KNTS -^Multicultural Radio Broadcasting 206443-8200 fax:206-777-1133 Sister to: KVRI 2201 6th Ave Ste 1500, Seattle 98121 Centralia-Chehalis 360-371-5500 fax:360-371-7617 GM Andrew Adams SM Chad Gammage Box 75150, White Rock BC V4B 5 PD Dave Drui CE Monte Passmore KITI Oldies 4840 Lincoln Rd, Blaine 98230 www.kgnw.com 1420 500015000 DA-2 GM/SM/PD Gary Nawman CE Mike Gilbert Seattle/Tacoma/EvereH Arbitron 0.3 Shr 38,100 Cume +Premier Broadcasters, Inc. -

DRIDIETARY REFERENCE INTAKES Thiamin, Riboflavin, Niacin, Vitamin
Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline http://www.nap.edu/catalog/6015.html DIETARY REFERENCE INTAKES DRI FOR Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline A Report of the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and its Panel on Folate, Other B Vitamins, and Choline and Subcommittee on Upper Reference Levels of Nutrients Food and Nutrition Board Institute of Medicine NATIONAL ACADEMY PRESS Washington, D.C. Copyright © National Academy of Sciences. All rights reserved. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline http://www.nap.edu/catalog/6015.html NATIONAL ACADEMY PRESS • 2101 Constitution Avenue, N.W. • Washington, DC 20418 NOTICE: The project that is the subject of this report was approved by the Governing Board of the National Research Council, whose members are drawn from the councils of the National Academy of Sciences, the National Academy of Engineering, and the Institute of Medicine. The members of the committee responsible for the report were chosen for their special competences and with regard for appropriate balance. This project was funded by the U.S. Department of Health and Human Services Office of Disease Prevention and Health Promotion, Contract No. 282-96-0033, T01; the National Institutes of Health Office of Nutrition Supplements, Contract No. N01-OD-4-2139, T024, the Centers for Disease Control and Prevention, National Center for Chronic Disease Preven- tion and Health Promotion, Division of Nutrition and Physical Activity; Health Canada; the Institute of Medicine; and the Dietary Reference Intakes Corporate Donors’ Fund.