Health, Wcd, Dgps and Ngos on Implementation of the Pc & Pndt
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

C O N T E N T S
22.12.2014 1 C O N T E N T S Sixteenth Series, Vol.VI, Third Session, 2014/1936 (Saka) No.21, Monday, December 22, 2014/Pausa 1, 1936 (Saka) S U B J E C T P A G E S OBITUARY REFERENCE 2 ORAL ANSWERS TO QUESTIONS Starred Question No.401 to 405 4-44 WRITTEN ANSWERS TO QUESTIONS Starred Question Nos.406 to 420 45-98 Unstarred Question Nos.4601to 4830 99-495 The sign + marked above the name of a Member indicates that the Question was actually asked on the floor of the House by that Member. 22.12.2014 2 PAPERS LAID ON THE TABLE 496-508 MESSAGE FROM RAJYA SABHA 509 BUSINESS ADVISORY COMMITTEE 509 10th Report COMMITTEE ON WELFARE OF SCHEDULED 509 CASTES AND SCHEDULED TRIBES Study Tour Report COMMITTEE ON PAPERS LAID ON THE TABLE 510 1st and 2nd Reports STANDING COMMITTEE ON AGRICULTURE 510 5th Report STANDING COMMITTEE ON INFORMATION 510-511 TECHNOLOGY 1st to 4th Reports STANDING COMMITTEE ON DEFENCE 511 2nd to 5th Reports STANDING COMMITTEE ON ENERGY 511-512 st rd 1 to 3 Reports STANDING COMMITTEE ON EXTERNAL AFFAIRS 512 3rd and 4th Reports STANDING COMMITTEE ON FINANCE 512 4th, 8th, and 9th Reports STANDING COMMITTEE ON FOOD, CONSUMER 513 AFFAIRS AND PUBLIC DISTRIBUTION 1st and 2nd Reports STANDING COMMITTEE ON LABOUR 513 3rd Report 22.12.2014 3 STANDING COMMITTEE ON COAL AND STEEL 513-514 1st to 6th Reports STANDING COMMITTEE ON COMMERCE 514 115th and 116th Reports STANDING COMMITTEE ON HOME AFFAIRS 515 182nd and 183rd Reports STATEMENTS BY MINISTERS (i)Status of implementation of the recommendations contained in the 251st Report of the Standing Committee on Industry on ‘functioning of Prime Minister’s Employment Generation Programme (PMEGP)’, pertaining to the Ministry of Micro, Small and Medium Enterprises. -
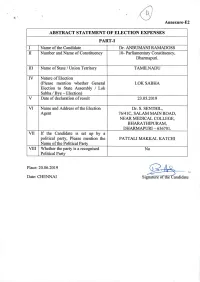
ABSTRACT STATEMENT of ELECTION EXPENSES PART-I I Name of the Candidate Dr
Annexure-E2 ABSTRACT STATEMENT OF ELECTION EXPENSES PART-I I Name of the Candidate Dr. ANBUMANI RAMADOSS II Number and Name of Constituency 10- Parliamentary Constituency, Dharmapuri. III Name of State / Union Territory TAMILNADU IV Nature of Election (Please mention whether General LOK SABHA Election to State Assembly / Lok Sabha / Bye - Election) V Date of declaration of result 23.05.2019 VI Name and Address of the Election Dr. S. SENTHIL, Agent 76/41C, SALAM MAIN ROAD, NEAR MEDICAL COLLEGE, BHARATHIPURAM, DHARMAPURI - 636701. VII If the Candidate is set up by a political party, Please mention the PATTALI MAKKAL KATCHI Name of the Political Party VIII Whether the party is a recognised No Political Party_______________ Place: 20.06.2019 O Date: CHENNAI Signature of theCandidate PART-II ABSTRACT OF STATEMENT OF ELECIONS EXPENDITURE OF CANDIDATE Amt. Incurred Amt. Incurred / Amt. Incurred Total Election S. Auth. By Authorized by Particulars Authorized by Expenditure No Candidate / Pol. Party in others in Rs. (3)+(4)+(5) Election Rs. agent in Rs. in 121 151 I Expenses in public meeting, rally, procession etc., I.(a) Expenses in Public Meeting, Rally, Procession etc. (i.e other than the ones 1732042 1732042 with Star Campaigners of the Political party. (Enclose as per Schedule-I) I.(b) Expenditure in public meeting rally, procession etc. with the Star Campaigners (i.e other than those for 1375820 1375820 general party propaganda) (Enclose as per Schedule-2) II Campaign materials other than those used in the public meeting, rally, procession -
LOK SABHA ___ SYNOPSIS of DEBATES (Proceedings Other Than
LOK SABHA ___ SYNOPSIS OF DEBATES (Proceedings other than Questions & Answers) ______ Wednesday, August 13, 2014 / Shravana 22, 1936 (Saka) ______ OBITUARY REFERENCE HON'BLE SPEAKER: Hon. Members, I have to inform the House of the sad demise of Shri Resham Lal Jangde. Shri Jangde died on 11 August, 2014 in Raipur, Chhattisgarh at the age of 89. He was a member of the First, Second and Ninth Lok Sabhas representing the Bilaspur Parliamentary Constituency of Madhya Pradesh, now in Chhattisgarh. An able parliamentarian, Shri Jangde served as a member of various Parliamentary Committees. Shri Jangde was a member of the Madhya Pradesh Legislative Assembly for three terms from 1962 to 1967, 1972 to 1977 and from 1985 to 1989. He also served as Deputy Minister in the Government of Madhya Pradesh in 1963. An active social and political worker, Shri Jangde participated in freedom movement. He worked relentlessly for social harmony and eradication of the dowry system. We deeply mourn the loss of Shri Resham Lal Jangde and convey our condolences to the bereaved family. The Members then stood in silence for a short while. ELECTION OF DEPUTY SPEAKER THE MINISTER OF HOME AFFAIRS (SHRI RAJNATH SINGH) moved that Dr. M. Thambidurai , a member of this House, be chosen as the Deputy Speaker of this House. THE MINISTER OF EXTERNAL AFFAIRS AND MINISTER OF OVERSEAS INDIAN AFFAIRS (SHRIMATI SUSHMA SWARAJ) seconded the motion. SHRI BHARTRUHARI MAHTAB moved that Dr. M. Thambidurai, a member of this House, be chosen as the Deputy Speaker of this House. SHRI TATHAGATA SATPATHY seconded the motion. -
LOK SABHA ___ BULLETIN-PART II (General Information Relating To
LOK SABHA ___ BULLETIN-PART II (General Information relating to Parliamentary and other matters) ________________________________________________________________________ Nos. 7315-7338] [Tuesday, Septemeber 18, 2018/ Bhadrapada 27, 1940(Saka) _________________________________________________________________________ No. 7315 Committee Branch-I Members of the Committee on Commerce The following are the members of the Committee on Commerce w.e.f. 01 September, 2018:- Lok Sabha 1. Shri Dibyendu Adhikari 2. Shri Subhash Chandra Baheria 3. Shri Abhishek Banerjee 4. Smt. Bijoya Chakravarty 5. Shri Jitendra Chaudhury 6. Shri Dushyant Chautala 7. Smt. Kavitha Kalvakuntla 8. Dr. Hari Babu Kambhampati 9. Shri Nityanand Rai 10. Shri Dhananjay Bhimrao Mahadik 11. Shri Kamal Nath 12. Shri Kamlesh Paswan 13. Shri K.R.P. Prabakaran 14. Shri T. Radhakrishnan 15. Shri Dipsinh Shankarsinh Rathod 16. Shri Khan Saumitra 17. Advocate (Shri) Narendra Keshav Sawaikar 18. Shri Kirti Vardhan Singh 19. Shri Vinod Kumar Sonkar 20. Shri Narsimham Thota 21. Vacant Rajya Sabha 22. Smt. Roopa Ganguly 23. Shri Naresh Gujral 24. Shri Sushil Kumar Gupta 25. Shri Ram Kumar Kashyap 26. Shri M.P. Veerendra Kumar 27. Smt. Thota Seetharama Lakshmi 28. Shri Vayalar Ravi 29. Shri Kapil Sibal 30. Dr. Kanwar Deep Singh 31. Shri Rakesh Sinha Shri Naresh Gujral has been appointed Chairperson of the Committee. ---------- No.7316 Committee Branch-I Members of the Committee on Home Affairs The following are the members of the Committee on Home Affairs w.e.f. 01 September, 2018:- Lok Sabha 1. Dr. Sanjeev Kumar Balyan 2. Shri Prem Singh Chandumajra 3. Shri Adhir Ranjan Chowdhury 4. Dr. (Smt.) Kakoli Ghosh Dastidar 5. Shri Ramen Deka 6. -

Report of the National Commission on Macroeconomics and Health Report of the National Commission on Macroeconomics and Health
Report of the National Commission on Macroeconomics and Health Report of the National Commission on Macroeconomics and Health Report of the National Commission on Macroeconomics and Health Report of the Report of the National Commission on Macroeconomics and Health Report of the National Commission on Macroeconomics and Health National Commission on Report of the Macroeconomics and Health National Commission on Macroeconomics and Health MINISTRY OF HEALTH AND FAMILY WELFARE GOVERNMENT OF INDIA, 2005 EQUITABLE DEVELOPMENT • HEALTHY FUTURE Report of the National Commission on Macroeconomics and Health National Commission on Macroeconomics and Health Ministry of Health & Family Welfare Government of India, New Delhi August 2005 © Ministry of Health & Family Welfare, Government of India September 2005 ISBN 81-7525-633-8 This Report does not address tertiary care and related areas such as super speciality hospital development in the public or private sector, telemedicine, medical tourism, environmental pollution or food safety etc. though they are all equally important. The Commission Report is based on background papers which can be accessed from the NCMH website www.mohfw.nic.in. They have also been published in two companion volumes. This report was written during the period April 1, 2004 - March 31, 2005. Printed at: Cirrus Graphics Private Limited B 261, Phase I, Naraina Industrial Area, New Delhi 110 028 Tel: + 91 11 51411507/1508 Fax: +91 11 51417575 email: [email protected] Editors: Pranay G. Lal and Byword Editorial Consultants Cover design: Quote Design Studio ii REPORT OF THE NATIONAL COMMISSION ON MACROECONOMICS AND HEALTH Members of the National Commission on Macroeconomics & Health Shri P. -

Setback for NCP's Saseendran TN Has Dozen CM Candidates-In-Waiting
NEW DELHI | SATURDAY | JANUARY 6, 2018 nation 07 KERALA SEX-TALK SCANDAL Political gains TN has dozen CM motive behind Setback for NCP’s Saseendran triple talaq ing for the court’s decision on The woman had said in her candidates-in-waiting Complainant the woman’s plea for approach- petition that she had com- Bill: CPM ing the CPI(M)-led ruling LDF, plained against the former KUMAR CHELLAPPAN n Madurai-based son of Haassan, another film star, PTI n THIRUVANANTHAPURAM withdraws in which NCP is a partner, with Minister due to some misun- CHENNAI Karunanidhi, would react to who too had announced his a request for reinstating him in derstanding and she wanted the Stalin’s candidature. The DMK political plans is making nois- he CPI(M) on Friday the Cabinet. A judicial com- case to be withdrawn as a set- ith superstar Rajinikanth has not won any election with- es from the sidelines before he Taccused the BJP-led settlement plea mission which had looked into tlement had been reached out- Wdeclaring his political out the cooperation of Alagiri plunges into the arena. Haassan Government at the Centre of VR JAYARAJ n KOCHI the matter had already exon- side the court. She had dreams on the New Year Eve, who wields considerable influ- too has not announced the using the triple talaq bill for erated him effectively. approached the High Court Tamil Nadu politics which had ence in southern Tamil Nadu. details of the political outfit to “political gains”. Prime Minister he dreams of Kerala NCP’s In fact, Friday’s develop- after the Chief Judicial moved around former Chief Anbumani Ramadoss, son be launched by him. -

The Minister of Health and Family Welfare (Dr
LOK SABHA ___ SYNOPSIS OF DEBATES (Proceedings other than Questions & Answers) ______ Thursday, October 23, 2008 /Kartika 1, 1930 (Saka) ______ STATEMENT BY THE MINISTER Re. The National Land Records Modernization Programme (NLRMP) THE MINISTER OF RURAL DEVELOPMENT (DR. RAGHUVANSH PRASAD SINGH): The National Common Minimum Programme (NCMP) of the UPA Government envisages that “Revenue Administration will be thoroughly modernized and clear land titles will be established.” Following up on this mandate, the National Land Records Modernization Programme (NLRMP) was formulated after extensive and in- depth consultations with the States and UTs, the concerned Ministries/Departments of the Government of India and expert agencies. The NLRMP was approved by the Cabinet in its meeting held on 21st August, 2008. The main objective of the NLRMP is to develop a modern, comprehensive and transparent land records management system with the ultimate aim of implementing the conclusive land-titling system with title guarantee. The Programme will be implemented as a Centrally-sponsored scheme with various components with the following assistance: (i) Computerisation of land records including digitization of cadastral maps, integration of textual and spatial data, data centres at Tehsil and State level, inter-connectivity among revenue offices. (100% by Government of India) (ii) Survey/resurvey and updating of the survey & settlement records (including ground control network and ground trulting) using modern technology options. (50% by Government of India) (iii) Computerization of Registration including connectivity to SROs with revenue offices. (25% by Government of India) (iv) Modern record rooms/land records management centres at Tehsil level. (50% by Government of India) (v) Training & capacity building (100% by Government of India) (vi) Core GIS (100% by Government of India) The total capital cost of the NLRMP (Central and State shares) has been estimated as Rs. -
C on T E N T S
C ON T E N T S Fourteenth Series, Vol. XXXVI, Fourteenth Session (Part-II), 2008/1930 (Saka) No.14, Wednesday, December 17, 2008/ Agrahayana 26, 1930 (Saka) S U B J E C T P A G E S ORAL ANSWERS TO QUESTIONS *Starred Question Nos.261 to 265 1-50 WRITTEN ANSWERS TO QUESTIONS Starred Question Nos. 266 to 280 51-93 Unstarred Question Nos.2683-2912 94-455 * The sign + marked above the name of a Member indicates that the Question was actually asked on the floor of the House by that Member. PAPERS LAID ON THE TABLE 456-491 MESSAGES FROM RAJYA SABHA 492-493 ESTIMATES COMMITTEE 19th and 20th Reports 494 PUBLIC ACCOUNTS COMMITTEE 78th to 80th Reports 494 COMMITTEE ON PETITIONS 43rd to 45th Reports 495 STANDING COMMITTEE ON HUMAN RESOURCE DEVELOPMENT 212th Report 496 STATEMENT BY MINISTERS 497-508 (i) Status of implementation of the recommendations contained in the 70th Report of the Standing Committee on Finance on Demands for Grants (2008-09), pertaining to the Ministry of Statistics and Programme Implementation. Shri G.K. Vasan 497-499 (ii) Status of implementation of the recommendations contained in the 204th Report of the Standing Committee on Human Resource Development on Demands for Grants (2007-08), pertaining to the Ministry of Youth Affairs and Sports. Dr. M.S. Gill 500 (iii) Status of implementation of the (a) recommendations contained in the 23rd Report of the Standing Committee on Personnel, Public Grievances, Law and Justice on the Government's policy of appointment on compassionate ground, pertaining to the Ministry of Personnel, Public Grievances and Pensions (b) Status of implementation of the recommendations contained in the 189th Report of the Standing Committee on Science and Technology, Environment and Forests on Demands for Grants (2008-09), pertaining to the Department of Space. -

ANSWERED ON:07.07.2004 CHILDREN INFECTED by FLOUROSIS Pateriya Smt
GOVERNMENT OF INDIA HEALTH AND FAMILY WELFARE LOK SABHA STARRED QUESTION NO:42 ANSWERED ON:07.07.2004 CHILDREN INFECTED BY FLOUROSIS Pateriya Smt. Neeta Will the Minister of HEALTH AND FAMILY WELFARE be pleased to state: (a) whether the Government is aware that thousands of children are suffering from flourosis due to drinking of fluoride contaminated drinking water in some of the States; (b) if so, the details thereof; (c) whether thousands of children residing in Shivni, Jabalpur, Narsingpur etc. districts of Madhya Pradesh are also similarly affected; (d) if so, the details thereof; and (e) the corrective steps taken/proposed to be taken by the Government in this regard? Answer THE MINISTER OF HEALTH AND FAMILY WELFARE (DR. ANBUMANI RAMADOSS) (a)to(e): A statement is laid on the Table of the House. STATEMENT REFERRED TO IN REPLY TO LOK SABHA STARRED QUESTION NO. 42 FOR 7TH JULY, 2004 Based on the UNICEF Report of 1999 on fluorine content of the drinking water in the country, fluorosis is a problem in 19 States which are Andhra Pradesh, Gujarat, Rajasthan, Karnataka, Orissa, Punjab, Maharasthra, Madhya Pradesh, Haryana, Bihar, Tamil Nadu, Uttar Pradesh, West Bengal, Kerala, Assam, Delhi, Jammu & Kashmir, Jharkhand and Chhattisgarh. It is estimated that 6 million children below the age of 14 years are at risk. 14 districts of Madhya Pradesh including Seoni district are endemic for fluorosis due to fluoride content in drinking water. The Government of Madhya Pradesh has denied the reports that thousands of children are suffering from fluorisis in various districts such as Seoni, Jabalpur and Narsingpur. -
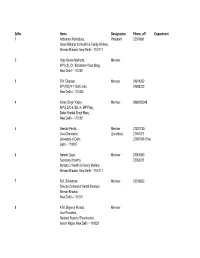
Directory As on 28-12-2007
SrNo. Name Designation Phone_off Department 1 Anbumani Ramadoss, President 23010661 Union Minister for Health & Family Welfare, Nirman Bhawan, New Delhi – 110 011 2 Vijay Kumar Malhotra, Member MP (LS), Dr. Bishamber Dass Marg, New Delhi – 110 001 3 R.K. Dhawan, Member 24614262 MP (RS)141, Golf Links, 24693223 New Delhi – 110 003 4 Karan Singh Yadav, Member 9868180348 MP (LS)C-6, Blk.-A, MP Flats, Baba Khadak Singh Marg, New Delhi – 110 001 5 Deepak Pental, Member 27257725/ Vice Chancellor, (Ex-officio) 27667011 University of Delhi 27667049 (Fax) Delhi – 110007 6 Naresh Dayal, Member 23061863 Secretary (Health), 23063221 Ministry of Health & Family Welfare, Nirman Bhawan, New Delhi – 110 011 7 R.K. Srivastava Member 23019063 Director General of Health Services, Nirman Bhawan, New Delhi – 110 011 8 K.M. Shyama Prasad, Member Vice President, National Board of Examination, Ansari Nagar, New Delhi – 110029 9 S.S. Agarwal, Member 0522-2612411-18 Central Drug Research Institute, 9935643480 Chattar Manzil Palace, Post Box No. 173, Lucknow – 226001 10 B.P. Chatterjee, Member 033-4734971 Prof., Deptt. of Biological Chemistry, Indian Association for the Cultivation of Sciences, Kolkatta – 700 032 11 R.P. Agarwal Member 23386451 Secretary, Department of Secondary Education and Higher Education, Ministry of Human Resource Development (HRD), Shastri Bhawan New Delhi – 110 001. 12 K.K. Talwar Member 0172-2745062 Director, Postgraduate Institute of Medical Education & Research, Chandigarh 13 Kartar Singh Member Director, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow 14 R. Surendran, Member 9841042227 Prof. & Head, Surgical Gastroenterology, Govt. Stanley Hopsital, Chennai *15. B.P. Agarwal, Member 23386451 Sec. -

67% Turnout in Second Phase of LS Poll Govt
https://t.me/TheHindu_Zone_official follow us: friday, april 19, 2019 Delhi City Edition thehindu.com 36 pages ț ₹10.00 facebook.com/thehindu twitter.com/the_hindu If they are chaiwale, William Barr defends Jet employees take to Mumbai Indians post we are doodhwale, Trump ahead of release the streets after airline a convincing win says Akhilesh Yadav of Mueller probe report shuts operations over Delhi Capitals page 11 page 12 page 13; Editorial: page 8 page 15 Printed at . Chennai . Coimbatore . Bengaluru . Hyderabad . Madurai . Noida . Visakhapatnam . Thiruvananthapuram . Kochi . Vijayawada . Mangaluru . Tiruchirapalli . Kolkata . Hubballi . Mohali . Malappuram . Mumbai . Tirupati . lucknow . cuttack . patna NEARBY 67% turnout in second phase of LS poll Govt. suspends cross-LoC trade after ‘misuse by Highest polling of 78% recorded in Puducherry; 71% exercise franchise in T.N. Assembly bypolls Special Correspondent Speaker M. Thambi Durai arms, drugs smugglers’ NEW DELHI (AIADMK); former Union Mi Shoe hurled at BJP The second phase of the Lok nisters A. Raja, T.R. Baalu, ‘Routes being used to move fake currency’ spokesman at press meet Sabha election on Thursday Dayanidhi Maran and S. Ja NEW DELHI for 95 constituencies regis gathrakshakan (all DMK); BJP MP and spokesperson tered a tentative voter tur Anbumani Ramadoss (PMK); G.V.L. Narasimha Rao was at nout of 67.6% across 11 States and E.V.K.S. Elangovan the receiving end of a shoe and one Union Territory, (Congress). thrown at him by a man with sporadic incidents of Election to the Tripura identified as Shakti Bhargava, violence. (East) seat was postponed to while he was addressing a The overall figure was April 23 because of security press conference at the party 69.62% in 2014. -

4 (16Th LOK SABHA )
Election Commission of India, General Elections, 2014 (16th LOK SABHA ) 4 - LIST OF SUCCESSFUL CANDIDATES CONSTITUENCY Category WINNER Social Category PARTY PARTY SYMBOL MARGIN Andaman & Nicobar Islands 1 Andaman & GEN Bishnu Pada Ray GEN BJP Lotus 7812 Nicobar Islands ( 4.14 %) Andhra Pradesh 2 Adilabad ST Godam Nagesh ST TRS Car 171290 ( 16.65 %) 3 Amalapuram SC Dr Pandula Ravindra SC TDP Bicycle 120576 Babu ( 10.82 %) 4 Anakapalli GEN Muttamsetti Srinivasa GEN TDP Bicycle 47932 Rao (Avanthi) ( 4.21 %) 5 Anantapur GEN J.C. Divakar Reddi GEN TDP Bicycle 61991 ( 5.15 %) 6 Aruku ST Kothapalli Geetha ST YSRCP Ceiling Fan 91398 ( 10.23 %) 7 Bapatla SC Malyadri Sriram SC TDP Bicycle 32754 ( 2.78 %) 8 Bhongir GEN Dr. Boora Narsaiah GEN TRS Car 30544 Goud ( 2.54 %) 9 Chelvella GEN Konda Vishweshwar GEN TRS Car 73023 Reddy ( 5.59 %) 10 Chittoor SC Naramalli Sivaprasad SC TDP Bicycle 44138 ( 3.70 %) 11 Eluru GEN Maganti Venkateswara GEN TDP Bicycle 101926 Rao (Babu) ( 8.54 %) 12 Guntur GEN Jayadev Galla GEN TDP Bicycle 69111 ( 5.59 %) 13 Hindupur GEN Kristappa Nimmala GEN TDP Bicycle 97325 ( 8.33 %) 14 Hyderabad GEN Asaduddin Owaisi GEN AIMIM Kite 202454 ( 20.95 %) 15 Kadapa GEN Y.S. Avinash Reddy GEN YSRCP Ceiling Fan 190323 ( 15.93 %) 16 Kakinada GEN Thota Narasimham GEN TDP Bicycle 3431 ( 0.31 %) 17 Karimnagar GEN Vinod Kumar GEN TRS Car 204652 Boinapally ( 18.28 %) 18 Khammam GEN Ponguleti Srinivasa GEN YSRCP Ceiling Fan 12204 Reddy ( 1.04 %) 19 Kurnool GEN Butta Renuka GEN YSRCP Ceiling Fan 44131 ( 4.18 %) 20 Machilipatnam GEN Konakalla Narayana GEN TDP Bicycle 81057 Rao ( 7.15 %) 21 Mahabubabad ST Prof.