Janapr2008.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Indiana Jew: Josh Bernstein Is "Digging for the Truth" January 17, 2007
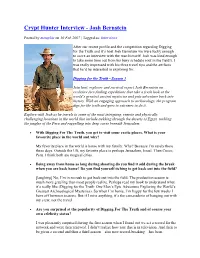
Indiana Jew: Josh Bernstein is "Digging for the Truth" January 17, 2007 Josh Bernstein is "Digging for the Truth." (PHOTO: Brendan Goeckel © Josh Bernstein) Josh Bernstein, the wide-brim hat-wearing, khaki-clad host of The History Channel’s hit television show “Digging for the Truth,” is chastising me. Skeptical, I am questioning the likelihood of a Manhattan-bred, Conservative Jew’s expertise in outdoor survival. “You know, at one point, we were all competent wilderness travelers,” he says good-naturedly. “I just reverted to an old-school Jewish lifestyle.” But these days his lifestyle is quite hectic. On this Friday afternoon in New York, Bernstein, 35, has some rare down time. Having recently completed the eight-month-long shoot of the DFT’s third season, he is gearing up for a book tour. In his new book, Digging for the Truth: One Man’s Epic Adventure Exploring the World’s Greatest Archaeological Mysteries, Bernstein goes behind-the-scenes, sharing “so much more than what you see during the 47 minutes of the show.” In it, he also dispenses practical adventure advice. Like for those inclined to build shelter in the snow, he provides instruction on “How to Build a Quinzhee.” And lest anyone think his globe-trotting job is all-glamour, Bernstein even writes about his lack of sleep, the itchy spider bites and the strange intestinal parasites he has picked up on location. So while his televised search for archeological adventure has brought comparisons to the movie hero “Indiana Jones,” his real-life story is more wandering Jew. -

48 Annual Daytime Emmy Awards NOMINATIONS – June 25Th
48th Annual Daytime Emmy Awards NOMINATIONS – June 25th Please read below and check your entries for the correct spelling, title, and to make sure nobody who is eligible is missing. This list marks everyone who is officially a Daytime Emmy nominee in these categories and is the list we will use to verify statue orders in the event of a win. To make changes to this list, please read below carefully for the instructions: Please send an email to Daytime Administration at [email protected] with the subject line “Nominee Corrections and Additions – June 25th” and list the following information in the body of the email: Category Show Title Entrant’s Name Entrant’s Title # of Episodes in 2020 (if a Series) Job Description (if an off-list title)** **All off-list titles, or individuals with less than the required minimum percentage of episodes, are subject to approval by the Awards Committee. All changes made prior to the ceremony on June 25th will be gratis for this year. We accept changes for $150 per change for 30 days after the ceremony. Changes beyond 30 days after the ceremony will not be accepted under any circumstances. Deadlines are established by the ceremony date in which that category is rewarded. This list will be updated with accepted changes once a week on Fridays at 5pm ET! OUTSTANDING DRAMA SERIES The Bold and the Beautiful CBS Bradley P. Bell, Executive Producer Edward J. Scott, Supervising Producer Casey Kasprzyk, Supervising Producer Cynthia J. Popp, Producer Mark Pinciotti, Producer Ann Willmott, Producer Days of Our Lives -

An Interview with Josh Bernstein
Digging for the Truth From K. Kris Hirst, Your Guide to Archaeology. FREE Newsletter. Sign Up Now! An Interview with Josh Bernstein The television program Digging for the Truth is a massively popular series broadcast by the History Channel, in which an intrepid fellow, Josh Bernstein, travels the world exploring archaeological sites and mysteries. In some archaeology circles, Digging for the Truth has raised some eyebrows, because of its glossy image, the emphasis on exciting frames of reference such as 'extreme archaeology', and the fact that the program attempts to solve complex archaeological problems in one or two hours. But the program I saw--the two hour premiere of Season 3, called "Atlantis: New Revelations"--was balanced and interesting, and put four of the current theories about the reality of Plato's legendary city under scientific scrutiny. Josh Bernstein is a New Yorker, with a BA in Anthropology from Cornell University. In addition, he has used much of his career as part of the Boulder Outdoor Survival School, where he has been CEO and President since 1997. His gig as host for Digging for the Truth began in 2004. In addition to being the host, Bernstein actively participates in the writing and producing of DFT, one of several for the History Channel's production team, JWM Productions. Recently, About.com reached Bernstein on location, where he took time out for an email interview. --- Digging for the Truth: Driven by Archaeology Mystery About.com: I know you're not an archaeologist by trade, so... What is that intrigues you about archaeology? What is it that makes you want to explore these topics? Josh Bernstein: I suppose I’ve always been fascinated by ancient cultures and people. -

Immigration Report 9/1/11 12:51 PM Page 1
September2011_Immigration Report 9/1/11 12:51 PM Page 1 Obama Administration Declares Inside . Administrative Amnesty for Illegal Aliens Cases Against Non-Criminal Aliens to be Dropped Unilaterally MEDIA RELIES ON FAIR FOR RESPONSE TO ADMINISTRATION PAGE 2 n a policy statement posted on the categories of illegal aliens whose cases are White House website and in letters to likely to be dismissed under the new policy. 9/11: TENTH ANNIVERSARY REPORT PAGE 2 Ileading members of Congress, the Simultaneously, in letters to Majority Obama administration declared what Leader Harry Reid (D-Nev.) and other FEDS SUE ALABAMA TO BLOCK amounts to an administrative amnesty for Senate Democrats who support the IMMIGRATION ENFORCEMENT PAGE 4 nearly all illegal aliens without criminal DREAM Act, Department of Homeland records. Under the guise of setting enforce - Security (DHS) Secretary Janet Napolitano BLACK ANGELINOS ORGANIZE ment priorities, the administration an - stated that potential DREAM Act ON IMMIGRATION PAGE 5 nounced that it would review some beneficiaries would no longer be subject to 300,000 pending cases against deportable removal. ARIZONA ASKS SUPREME COURT TO aliens, with the intent of dropping the The August 18th policy announce - RULE ON S.B. 1070 cases, and would cease to initiate new pro - ment takes dead aim not just at the integri - PAGE 5 ceedings against illegal aliens without crim - ty of U.S. immigration law, but on the con - SECURE COMMUNITIES WILL inal convictions. stitutional separation of powers. Under our CONTINUE (SO ADMINISTRATION CAN The statement, posted on the White constitution, Congress has the exclusive CLAIM IT ’S ENFORCING IMMIGRATION ) PAGE 6 House website by Intergovernmental authority to make immigration policies. -

Alumni Magazine C2-C4camjf07 12/21/06 2:50 PM Page C2 001-001Camjf07toc 12/21/06 1:39 PM Page 1
c1-c1CAMJF07 12/22/06 1:58 PM Page c1 January/February 2007 $6.00 alumni magazine c2-c4CAMJF07 12/21/06 2:50 PM Page c2 001-001CAMJF07toc 12/21/06 1:39 PM Page 1 Contents JANUARY / FEBRUARY 2007 VOLUME 109 NUMBER 4 alumni magazine Features 52 2 From David Skorton Residence life 4 Correspondence Under the hood 8 From the Hill Remembering “Superman.” Plus: Peres lectures, seven figures for Lehman, a time capsule discovered, and a piece of Poe’s coffin. 12 Sports Small players, big win 16 Authors 40 Pynchon goes Against the Day 40 Going the Distance 35 Camps DAVID DUDLEY For three years, Cornell astronomers have been overseeing Spirit 38 Wines of the Finger Lakes and Opportunity,the plucky pair of Mars rovers that have far out- 2005 Atwater Estate Vineyards lived their expected lifespans.As the mission goes on (and on), Vidal Blanc Associate Professor Jim Bell has published Postcards from Mars,a striking collection of snapshots from the Red Planet. 58 Classifieds & Cornellians in Business 112 46 Happy Birthday, Ezra 61 Alma Matters BETH SAULNIER As the University celebrates the 200th birthday of its founder on 64 Class Notes January 11, we ask: who was Ezra Cornell? A look at the humble Quaker farm boy who suffered countless financial reversals before 104 Alumni Deaths he made his fortune in the telegraph industry—and promptly gave it away. 112 Cornelliana What’s your Ezra I.Q.? 52 Ultra Man BRAD HERZOG ’90 18 Currents Every morning at 3:30, Mike Trevino ’95 ANATOMY OF A CAMPAIGN | Aiming for $4 billion cycles a fifty-mile loop—just for practice. -

Advertise in the CBS Newsletter
Advertise in the CBS Newsletter Monthly Ad rates Contact Sue Prousa Size Monthly [email protected] Half Page $72 or 630-961-1818 Quarter page $36 Please send payment made out to Eighth page $18 Congregation Beth Shalom to: Congregation Beth Shalom (Attention Newsletter Editor) 772 W. 5th Avenue Naperville, IL 60563 Staff Rabbi Marc Rudolph - [email protected] Cantor Hasha Musha Perman - [email protected] Education and Early Learning Director: Barbara Bernstein- [email protected] Facilities and Office Manager: Sue Prousa – [email protected] Secretary: Dorothy Battle – [email protected] Custodial support: Maureen Brown Inside this issue From the editor .............................................................................................................. 1 From The Desk Of The Rabbi ..................................................................................... 2 Domestic abuse doesn’t just impact adults ............................................................... 3 A note from our cantor ................................................................................................. 4 Prayers for daily occurences ....................................................................................... 5 WITH MANY THANKS (from Dorothy Battle) ........................................................... 9 Religious School News .............................................................................................. 10 JUF Right Start Grant ................................................................................................ -
Crypt Hunter Interview - Josh Bernstein
Crypt Hunter Interview - Josh Bernstein Posted by memphis on 10 Feb 2007 | Tagged as: Interviews After our recent profile and the competition regarding Digging for the Truth and it’s host Josh Bernstein we were lucky enough to score an interview with the man himself! Josh was kind enough to take some time out from his busy schedule (out in the field!). I was really impressed with his three travel tips and the artifacts that he’d be interested in exploring for. Digging for the Truth - Season 3 Join host, explorer and survival expert Josh Bernstein on exclusive fact-finding expeditions that take a fresh look at the world’s greatest ancient mysteries and puts adventure back into history. With an engaging approach to archaeology, the program digs for the truth and goes to extremes to do it. Explore with Josh as he travels to some of the most intriguing, remote and physically challenging locations in the world that include trekking through the deserts of Egypt, tackling the jungles of the Peru and rappelling into deep caves beneath Jerusalem. • With Digging For The Truth, you get to visit some exotic places. What is your favourite place in the world and why? My favorite place in the world is home with my family. Why? Because I’m rarely there these days. Outside the US, my favorite place is perhaps Jerusalem, Israel. Then Cusco, Peru. I think both are magical cities. • Being away from home so long during shooting do you find it odd during the break when you are back home? Do you find yourself itching to get back out into the field? [laughing] No, I’m in no rush to get back out into the field. -

Make the Dream a Reality: Why Passing the Dream Act Is the Logical First Step in Achieving Comprehensive Immigration Reform, 41 J
UIC Law Review Volume 41 Issue 4 Article 12 Summer 2008 Make the Dream a Reality: Why Passing the Dream Act is the Logical First Step in Achieving Comprehensive Immigration Reform, 41 J. Marshall L. Rev. 1251 (2008) Aimee Deverall Follow this and additional works at: https://repository.law.uic.edu/lawreview Part of the Administrative Law Commons, Courts Commons, Human Rights Law Commons, Immigration Law Commons, Juvenile Law Commons, Law and Politics Commons, Law and Race Commons, Law and Society Commons, Legislation Commons, and the Social Welfare Law Commons Recommended Citation Aimee Deverall, Make the Dream a Reality: Why Passing the Dream Act is the Logical First Step in Achieving Comprehensive Immigration Reform, 41 J. Marshall L. Rev. 1251 (2008) https://repository.law.uic.edu/lawreview/vol41/iss4/12 This Comments is brought to you for free and open access by UIC Law Open Access Repository. It has been accepted for inclusion in UIC Law Review by an authorized administrator of UIC Law Open Access Repository. For more information, please contact [email protected]. MAKE THE DREAM A REALITY: WHY PASSING THE DREAM ACT IS THE LOGICAL FIRST STEP IN ACHIEVING COMPREHENSIVE IMMIGRATION REFORM AIMEE DEVERALL* I. INTRODUCTION Dan-el Padilla endured a childhood that included living in homeless shelters, being abandoned by his father and thirteen separate moves from one slum apartment to another.1 So it was all the more commendable when, after maintaining a 3.9 grade- point average, Dan-el was named the salutatorian of his class at Princeton and delivered a commencement address in Latin. -
FALL 2020 DE DE DE DE = Digital Exclusive 16
FALL 2020 DE = Digital Exclusive 1. From the Rabbi’s Desk 2. A Message From Our Parnas 4. Announcements 12. Spring Fundraiser Sponsors 16. Reflections on Shearith Israel’s 2020 Fundraiser 18. Shearith Israel Has Gone Virtual CONTENTS 19. Programming DE 20. Writing Contest Winners: “My Jewish Life In the Time of Corona” 31. Jewish Education Our seasonal bulletins usually offer an abundance of upcoming programs as well 33. Spotlight on the Sisterhood as a few articles and retrospectives. This Fall, 35. Megillah Readings while still fraught with uncertainty as to what Gone Virtual programs will be possible – whether in-person or virtually – and which programs will be 36. Virtual Second Annual suitable given the ever changing circumstances, Smash the Stigma: presented our team with unique challenges... A Panelist’s Reflections and opportunities. 37. Culinary Corner The Fall Bulletin on your screen is lengthier DE 39. Retrospective: and more content-rich than ever, so much so Memorial Day 2020 that we have created this first-ever Expanded Digital Edition, which, as you can see, includes DE 42. Retrospective: even more expansive and colorful content, with Azharot Webcast: World- more articles and images. It is dedicated to Wide Virtual Reading everyone who has made our community more vital than ever during these past months: our 45. Hesed in Times of Corona intrepid leadership, our unflagging clergy, our 46. Services industrious staff, our dedicated facilities team, our passionate volunteers, and every congregant 50. Stay Connected and friend who has called in, logged in, or showed up (and supported us) during these 51. -

Marquette University the Law School Experience Student
MARQUETTE UNIVERSITY THE LAW SCHOOL EXPERIENCE WHAT DO YOU WANT FROM YOUR LAW SCHOOL EXPERIENCE? A mastery of knowledge. Sharpened critical-thinking skills. Real-world practical experience. Professional connections. The tools to land your dream job. Of course, you should expect this from any fine law school. So what sets Marquette Law School apart? Our commitment to you is the Marquette difference. To care for you as a whole person. To help you develop as a well-rounded individual. To do everything we can to help you succeed. In our experience, that will make you the best lawyer you can be. STUDENT The comforts of home “One of the most important things to ECKSTEIN HALL | 4 me about my law school experience was that it would feel like a community, A strong foundation in where my classmates were colleagues fundamental skills CURRICULUM | 6 rather than competitors.” — Josh Bernstein CLASS OF 2020 A path to pursue my passion SPECIALIZATION | 11 Innovative classes taught by experts FACULTY | 12 Professors invested in my success MENTORS | 14 Supportive classmates STUDENT LIFE | 16 A vibrant city and legal community MILWAUKEE | 20 Practical, real-world experience EXPERIENTIAL LEARNING | 22 The opportunity to make a difference PUBLIC SERVICE | 26 The right connections NETWORKING | 28 Help finding a job CAREER PLACEMENT | 30 Exceeding your expectations There are as many unique expectations for law school as there are prospective law students. Our goal is to exceed your expectations. We can succeed at this because, at Marquette University Law School, our commitment is not only to your legal education generally, but to you as an individual. -

PLEASE DELIVER TO: Published by Access Intelligence, LLC, Tel: 301-354-2101
URGENT! PLEASE DELIVER TO: www.cablefax.com, Published by Access Intelligence, LLC, Tel: 301-354-2101 5 Pages Today Friday — August 15, 2008 Volume 19 / No. 158 EBIF-errific: FiOS TV Launches 1st Major EBIF Trial Verizon FiOS TV subs in Portland, OR, are getting a little more out of this year’s Summer Games. The telco has launched its 1st EBIF trial in the city, teaming with Ensequence for an interactive Olympics application. The Port- land test is signifi cant for more than just Verizon, as it marks the 1st time an EBIF application has made its way to US consumers, according to Aslam Khader , Ensequence’s chief product officer. EBIF, or the Enhanced Television Binary Interchange Format, is a standard developed by CableLabs. Until tru2way is fully implemented in the cable industry, EBIF can be used to offer basic interactive applications on currently deployed/less advanced set-tops. While smaller EBIF trials have been underway with cable operators, the FiOS launch is the 1st to go out widely to consumers, explained Khader. “The implications are that all this work that has gone into EBIF over the last 3 years—starting with CableLabs working with various vendors like ourselves to put the standard in place and then the various MSOs taking the standard and beginning to implement it in their plant—this shows that it is real. EBIF can be used to do the kinds of things the standard was put in place to do,” he said. The Ensequence Olympics app on FiOS is running on MSNBC and CNBC. -

Q+A: Digging for the Truth Host Josh Bernstein Insights from the City Kid Who Uses His Outdoor Ingenuity to Show Armchair Travelers the World's Greatest Mysteries
Q+A: Digging for the Truth Host Josh Bernstein Insights from the city kid who uses his outdoor ingenuity to show armchair travelers the world's greatest mysteries. Text by Ryan Bradley Photograph courtesy of The History Channel NEW INDY: Digging for the Truth host Josh Bernstein seeks out the world's most intriguing ancient mysteries. The show's new season premieres on The History Channel on Monday, January 22, at 9 p.m. When he's not traveling the world unraveling ancient mysteries as host of The History Channel's Digging for the Truth (DFT), Josh Bernstein finds the time to run Boulder Outdoor Survival School, keep residences in New York City and Utah, become an author, and even sleep. Bernstein, 35, has just released a book by the same name as his popular television show (Gotham, $27.50). The travelogue shares behind-the-scenes stories and photos from some of the program's greatest moments—discovering Inca treasures in the Amazon, moving a megalith, and building a Viking ship, among others. Adventure tracked down a busy Bernstein (currently on a national book tour) to find out about the upcoming third season of DFT, the new book, and his iconic hat(s). Let's get all Indian Jones comparisons out of the way: Tell me about your hat. I've had several hats over the past 20-plus years, all named Henry (it's a long story). Henry I and II were Akubras, while Henry III through V were custom made for me by Steve King of Bounty Hunter Hats (III) in Telluride, Colorado, and Nathaniel Funmaker of Nathaniel's of Colorado (IV and V) in Mancos, Colorado.