Quantitative Assessment of Population Variability in Hepatic Drug Metabolism Using a Perfused Three-Dimensional Human Liver Microphysiological System S
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Extraction and Evaporation: Experiment 1 Separating the Components of a Mixture1 Week 1
Organic Chemistry I Laboratory Extraction and Evaporation: Experiment 1 Separating the Components of a Mixture1 Week 1 Background Reading Zubrick, J. W. The Organic Chem Lab Survival Manual, 4th edition, Wiley & Sons, Inc., New York, 1997. Keeping a Notebook: Pg 12-24. Interpreting Handbooks: Pg 26-31, 34-44. Extraction and Washing: Pg 148-168. Background Senario One of the many places organic chemists are employed is in private laboratories associated with consulting firms. The purpose of these labs is generally to provide chemical analysis or synthesis of material for customers. The first few labs in CHM 220 will teach you the basic techniques needed to analyze and purify mixtures to determine the individual components. This first lab will involve determining the composition of a possible pharmaceutical preparation. Watchdog agencies exist which monitor the pharmaceuticals sold over the counter in the United States. These agencies will use private laboratory firms to analyze products suspected of violating enforced standards. For example, a new brand of analgesic may appear on drugstore shelves at a low price. The label indicates that the tablets were manufactured in the United States by a legitimate pharmaceutical company. However, the labels may reveal discrepancies and the appearance/quality of the tablets could lead an investigator to suspect that they might be counterfeit. Such knockoffs of a domestic product can be manufactured cheaply elsewhere and smuggled into the US, where they are sold for high profits. This laboratory exercise places you in the position of analyzing a suspected counterfeit analgesic preparation. The label on the suspected bottle lists the ingredients per tablet as aspirin (200 mg), acetaminophen (250 mg), and sucrose (50 mg). -

Metabolism of Phenacetin in the Rat
METABOLISM OF PHENACETIN IN THE RAT CONRAD AGNELLO D'SOUZA B.Pharm. submitted in partial fulfilment of the requirements for the degree of Master of Pharmacy UNIVERSITY OF TASMANIA HOBART SEPTEMBER 1983. ‘, r \ytTL- cua biA-- 11\esi5 ekci tr vv. t1, PJiar,c\ b'Souz4 THE UNIVERSITY Of TASMANIA' LIBRARY 11L4 VI I SUMMARY The abuse of phenacetin-containing analgesic mixtures has been linked epidemiologically with nephrotoxicity and carcinogenicity in man. In addition, clinical and histopathological tests after chronic administration of phenacetin in man and animals have indicated that it is nephrotoxic and carcinogenic. Furthermore, it has a chemical similarity to other known carcinogenic arylamides. However, the induction of toxicity with phenacetin remains a controversial subject. A number of chronic dosing studies with phenacetin have been carried out to demonstrate the ability of the drug to induce carcinogenesis and nephropathy. However, none have sought to explain the reasons for the chronic nature of phenacetin toxicity on the basis of the increased formation of toxic metabolites after continued administration of the drug. In the present chronic daily-dosing study with phenacetin in the rat, the metabolism of the drug was monitored by analysing urine samples at regular weekly intervals. Particular attention was paid to the formation of N-hydroxyphenacetin, which has been implicated in phenacetin carcinogenicity. The metabolism of phenacetin was monitored in five groups of Hooded Wistar rats. Each group was subjected to a different treatment. The purpose was to elucidate the effects of the size of the dose, duration of treatment, influence of commonly co- administered drugs (aspirin, caffeine) and the influence of a sulfation inhibitor (pentachlorophenol) on the metabolism of phenace tin. -

Drug-Induced Immune Hemolytic Anemia: the Last 30 Years of Changes P
George Garratty 1935–2014 Journal of Blood Group Serology and Molecular Genetics VOLUME 30, N UMBER 2, 2014 Immunohematology Journal of Blood Group Serology and Molecular Genetics Volume 30, Number 2, 2014 CONTENTS Introduction to Immunohematology Special Edition on 43 Drug-Induced Immune Cytopenias P.A. Arndt and R.M. Leger R EPORT 44 Drug-induced immune hemolytic anemia: the last 30 years of changes P. A . A r ndt R EPORT 55 Drug-induced immune thrombocytopenia: incidence, clinical features, laboratory testing, and pathogenic mechanisms B.R. Curtis R EPORT 66 Drugs that have been shown to cause drug-induced immune hemolytic anemia or positive direct antiglobulin tests: some interesting findings since 2007 G. Garratty and P.A. Arndt C A SE R EPORT 80 Diagnostic pitfalls of drug-induced immune hemolytic anemia A. Salama and B. Mayer R EPORT 85 How we investigate drug-induced immune hemolytic anemia R.M. Leger, P.A. Arndt, and G. Garratty R EPORT 95 Drug-induced immune neutropenia/agranulocytosis B.R. Curtis 102 A NNOUNCEMENTS 105 A DVERT I SEMENTS 109 I NSTRUCT I ONS FOR A UTHORS E D I TOR - I N -C H I EF E D I TOR ia L B OA RD Sandra Nance, MS, MT(ASCP)SBB Philadelphia, Pennsylvania Patricia Arndt, MT(ASCP)SBB Thierry Peyrard, PharmD, PhD Pomona, California Paris, France M A N AG I NG E D I TOR Barbara J. Bryant, MD Mark Popovsky, MD Cynthia Flickinger, MT(ASCP)SBB Milwaukee, Wisconsin Braintree, Massachusetts Philadelphia, Pennsylvania Lilian Castilho, PhD S. Gerald Sandler, MD Campinas, Brazil Washington, District of Columbia TECHN I C A L E D I TORS Christine Lomas-Francis, MSc Martha R. -

Acute Spinal Cord Injury Changes the Disposition of Some, but Not All Drugs Given Intravenously
Spinal Cord (2007) 45, 603–608 & 2007 International Spinal Cord Society All rights reserved 1362-4393/07 $30.00 www.nature.com/sc Original Article Acute spinal cord injury changes the disposition of some, but not all drugs given intravenously P Garcı´ a-Lo´ pez*,1, A Martı´ nez-Cruz2, G Guı´ zar-Sahagu´ n2,3 and G Castan˜ eda-Herna´ ndez4 1Laboratorio de Farmacologı´a, Subdireccio´n de Investigacio´nBa´sica, Instituto Nacional de Cancerologı´a, Me´xico, DF, Me´xico; 2Laboratorio de Morfologı´a, Proyecto Camina A.C., Me´xico, DF, Me´xico; 3Unidad de Investigacio´nMe´dica en Enfermedades Neurolo´gicas, Centro Me´dico Nacional Siglo XXI, IMSS, Me´xico, DF, Me´xico; 4Departamento de Farmacologı´a, CINVESTAV-IPN, Me´xico, DF, Me´xico Study design: Experimental laboratory investigations in paraplegic rats. Objective: In order to understand why acute spinal cord injury (SCI) changes the disposition of some, but not all drugs given intravenously (i.v.), pharmacokinetic parameters of drugs with different pharmacological properties were evaluated to determine the influence of SCI on physiological processes such as distribution, metabolism and excretion. Setting: Mexico City, Mexico. Methods: Rats were subjected to severe SCI (contusion) at T-9 level; pharmacokinetic studies of phenacetin, naproxen or gentamicin were performed 24h after. These drugs were not chosen as markers because of their therapeutic properties, but because of their pharmacokinetic characteristics. Additional studies including plasma proteins, liver and renal function tests, and micro-vascular hepatic blood flow, were also performed at the same time after injury. Results: Acute SCI significantly reduced distribution of drugs with intermediate and low binding to plasma proteins (phenacetin 30% and gentamicin 10%, respectively), but distribution did not change when naproxen – a drug highly bound to plasma proteins (99%) – was used, in absence of changes in plasma proteins. -

Renal Accumulation of Salicylate and Phenacetin: Possible Mechanisms in the Nephropathy of Analgesic Abuse
Renal accumulation of salicylate and phenacetin: possible mechanisms in the nephropathy of analgesic abuse Lewis W. Bluemle Jr., Martin Goldberg J Clin Invest. 1968;47(11):2507-2514. https://doi.org/10.1172/JCI105932. Research Article Since either aspirin or phenacetin might be causative in the nephropathy of analgesic abuse, studies were designed to examine the renal accumulation and distribution of the major metabolic products of these compounds, salicylate and N- acetyl-p-aminophenol (APAP) respectively, in dogs. Nineteen hydropenic animals were studied, of which seven were given phenacetin, nine received acetyl salicylic acid, two were given both aspirin and phenacetin, and one received APAP directly. Two of three hydrated animals were given phenacetin and one was given aspirin. During peak blood levels of salicylate and (or) APAP, the kidneys were rapidly removed, frozen, sliced from cortex to papillary tip, and analyzed for water, urea, APAP, and salicylate. No renal medullary gradient for salicylate was demonstrable during both hydropenic and hydrated states. In contrast, both free and conjugated APAP concentrations rose sharply in the inner medulla during hydropenia, reaching a mean maximal value at the papillary tip exceeding 10 times the cortical concentration (P < 0.001), a distribution similar to that of urea. Salicylate had no effect on the APAP gradient, but hydration markedly reduced both the APAP and urea gradients in the medulla. The data indicate that APAP probably shares the same renal mechanisms of transport and accumulation as urea and acetamide, and that papillary necrosis from excessive phenacetin may be related to high papillary concentration of APAP. Find the latest version: https://jci.me/105932/pdf Renal Accumulation of Salicylate and Phenacetin: Possible Mechanisms in the Nephropathy of Analgesic Abuse LEWIS W. -

Development and Validation of a UPLC-MS/ MS Method for the Quantification of Aceta- Minophen in Human Plasma and Its Application
2016;24(1):30-36 TCP Transl Clin Pharmacol http://dx.doi.org/10.12793/tcp.2016.24.1.30 Development and validation of a UPLC-MS/ MS method for the quantification of aceta- minophen in human plasma and its application to pharmacokinetic studies Jaemin Cha1, Bo Kyung Kim1, Mi-Ri Gwon1, Joomi Lee1, Boram Ohk1, Woo Youl Kang1, Mi-sun Lim2, Sook Jin Seong1, Hyun-Ju Kim1, Hae Won Lee1 and Young-Ran Yoon1* 1Department of Biomedical Science, BK21 Plus KNU Bio-Medical Convergence Program for Creative Talent and Clinical Trial Cen- ter, Kyungpook National University Graduate School and Hospital, Daegu 41944, Korea, 2College of Pharmacy, Yeungnam University, Daegu 38541, Korea *Correspondence: Y. R. Yoon; Tel: +82-53-420-4950, Fax: +82-53-426-4944, E-mail: [email protected] ORIGINAL ARTICLE Received 8 Oct 2015 We developed an ultra-performance liquid chromatography-tandem mass spectrometry (UPLC- Revised 23 Nov 2015 MS/MS) method for the determination of acetaminophen concentration in human plasma. Fol- Accepted 25 Nov 2015 lowing protein precipitated extraction, the analytes were separated and analyzed using an UPLC- Keywords MS/MS in the multiple reaction monitoring (MRM) mode with the respective [M+H]+ ions, m/z Acetaminophen, Human plasma, 152.06 → 110.16 for acetaminophen and m/z 180.18 → 138.12 for phenacetin (internal standard, IS). UPLC-MS/MS, The method showed a linear response from 1 to 100 µg/mL (r > 0.9982). The limit of quantitation Validation, for acetaminophen in plasma was 1 µg/mL. The intra- and inter-day accuracy ranged in the ranges Pharmacokinetic study of 94.40–99.56% and 90.00–99.20%, respectively. -

Paracetamol and Phenacetin
Drugs 32 (Suppl. 4): 46-59 (1986) OOI2-6667/86/040<MJ046/$7.00/0 © ADIS Press Limited All rights reserved. Paracetamol and Phenacetin Stephen P. Clissold ADIS Drug Information Services, Auckland Summary Since their synthesis in the late l800s paracetamol (acetaminophen) and phenacetin have followed divergent pathways with regard to their popularity as mild analgesic/anti pyretic drugs. Initially, paracetamol was discarded in favour of phenacetin because the latter drug was supposedly less toxic. Today the opposite is true. and paracetamol. along with aspirin. has become one ofthe two most popular 'over-the-counter' non-narcotic anal gesic agents. This marked increase in the wide approval attained by paracetamol has been accompanied by the virtual commercial demise of phenacetin because of its role, albeit somewhat circumstantial. in causing analgesic nephropathy. Both paracetamol and phenacetin are effective mild analgesics, suitable for treating mild to moderate pain. and their actions are broadly comparable with those of aspirin and related salicylates. although they do not appear to possess significant anti-inflam matory activity. Since a major portion of a dose of phenacetin is rapidly metabolised to paracetamol. it seems possible that phenacetin owes some of its therapeutic activity to its main metabolite. paracetamol. whereas its most troublesome side effect (methaemoglo binaemia) is due to another metabolite. p-phenetidine. The mechanism of action of para cetamol is poorly defined. although it has been speculated that it may selectively inhibit prostaglandin production in the central nervous system. which would account for its anal gesic/antipyretic properties. The lack of any significant influence on peripheral cyclo oxygenase would explain the absence of anti-inflammatory activity. -

Thermodynamic Characteristics of Phenacetin in Solid State and Saturated Solutions in Several Neat and Binary Solvents
molecules Article Thermodynamic Characteristics of Phenacetin in Solid State and Saturated Solutions in Several Neat and Binary Solvents Maciej Przybyłek 1 , Anna Kowalska 1, Natalia Tymorek 1, Tomasz Dziaman 2 and Piotr Cysewski 1,* 1 Department of Physical Chemistry, Pharmacy Faculty, Collegium Medicum of Bydgoszcz, Nicolaus Copernicus University in Toru´n,Kurpi´nskiego5, 85-950 Bydgoszcz, Poland; [email protected] (M.P.); [email protected] (A.K.); [email protected] (N.T.) 2 Department of Clinical Biochemistry, Pharmacy Faculty, Collegium Medicum of Bydgoszcz, Nicolaus Copernicus University in Toru´n,Karłowicza 24, 85-950 Bydgoszcz, Poland; [email protected] * Correspondence: [email protected] Abstract: The thermodynamic properties of phenacetin in solid state and in saturated conditions in neat and binary solvents were characterized based on differential scanning calorimetry and spectroscopic solubility measurements. The temperature-related heat capacity values measured for both the solid and melt states were provided and used for precise determination of the values for ideal solubility, fusion thermodynamic functions, and activity coefficients in the studied solutions. Factors affecting the accuracy of these values were discussed in terms of various models of specific heat capacity difference for phenacetin in crystal and super-cooled liquid states. It was concluded that different properties have varying sensitivity in relation to the accuracy of heat capacity values. The values of temperature-related excess solubility in aqueous binary mixtures were interpreted using the Jouyban–Acree solubility equation for aqueous binary mixtures of methanol, DMSO, DMF, Citation: Przybyłek, M.; Kowalska, A.; Tymorek, N.; Dziaman, T.; 1,4-dioxane, and acetonitrile. -

5,8,10,14-Icosatetraenoic Acid Peroxidase Sensitive to Anti-Inflammatory Drugs (Aspirin/Salicylate/Indomethacin/Acetaminophen/Human Platelets) MARVIN I
Proc. Natl. Acad. Sci. USA Vol. 77, No. 1, pp. 308-312, January 1980 Biochemistry Arachidonate metabolism via lipoxygenase and 12L-hydroperoxy- 5,8,10,14-icosatetraenoic acid peroxidase sensitive to anti-inflammatory drugs (aspirin/salicylate/indomethacin/acetaminophen/human platelets) MARVIN I. SIEGEL*, RANDY T. MCCONNELL*, NED A. PORTERt, AND PEDRO CUATRECASAS* *Molecular Biology Department, The Wellcome Research Laboratories, Research Triangle Park, North Carolina 27709; and the tPaul M. Gross Chemical Laboratories, Duke University, Durham, North Carolina 27706 Communicated by George H. Hitchings, October 29, 1979 ABSTRACT The enzymes of arachidonate metabolism via inhibit the formation of prostacyclin via prostacyclin synthetase the lipoxygenase pathway in human platelet cytosol have been in porcine aorta (11) and other tissues (12). characterized and partially purified. The lipoxygenase activity The anti-inflammatory, analgesic, and antipyretic drugs has a pH optimum of 7.3 and reaches half-maximal activity at an arachidonate concentration of 80 ,sM. The oxidation of aspirin and indomethacin inhibit cyclo-oxygenase in vitro (13, arachidonate by these enzymes is inhibited by reagents that 14) whereas sodium salicylate does not (13, 15, 16) despite the modify sulfhydryl groups. Two separable lipoxygenase activities fact that it is an active drug when administered in vivo (17-21). can be detected by chromatography of platelet cytosol on However, all three drugs have recently been shown to interfere Sephadex G-150 and of partially purified preparations on with arachidonate metabolism via lipoxygenase in various cell DEAE-Sephadex. One of these has an apparent Mr of 100,000. types by reversibly inhibiting the conversion of HPETE to A second enzyme species behaves as a M, 160,000 entity con- HETE (22), suggesting that this effect may contribute to the taining, in addition to lipoxygenase, a peroxidase activity that catalyzes the conversion of 12L-hydroperoxy-5,8,10,14-icosa- mechanism of action of these drugs. -

Mutagenicity of Analgesics, Their Derivatives, and Anti-Inflammatory Drugs with S-9 Mix of Several Animal Species
J. Nihon Univ. Sch. Dent., Vol. 34. 183-195, 1992 Mutagenicity of Analgesics, Their Derivatives, and Anti-inflammatory Drugs with S-9 Mix of Several Animal Species Noboru KUBOYAMA and Akira FUJII (Received9 December1991 and accepted 2 March 1992) Key words: mutagenicity, analgesics, anti-inflammatory drugs, DNA damage, Ames test, Rec-assay Abstract An investigation was undertaken to determine whether analgesics and their derivatives (13 compounds), and anti-inflammatory drugs (4 compounds) had mutagenicity. Rec-assay was used to clarify specific DNA-damaging properties, and the Ames test was used to find back-mutations, using S-9 fractions obtained from the liver of 4 animal species pretreated with polychlorobiphenyl. In the Rec-assay, salicylic acid (2 mg), aspirin (5 mg), benzoic acid (4 mg), sulpyrine (0.4 mg), indomethacin (0.1 mg), oxyphenbutazone (0.1 mg) and di- clofenac sodium (0.1 mg) showed a DNA-damaging tendency. In the Ames test, mutagenicity of methyl salicylate was demonstrated using the Salmonella typhimurium TA98 strain upon addition of hamster S-9 mixture. Weak mutagenicity was also found using the TA100 strain with rat S-9 mixture for salicylic acid, sulpyrine, indomethacin and oxyphenbutazone, and with hamster S-9 mixture for methyl salicylate, acetaminophen and phenacetine. Introduction The mechanism of cancer induction has long been considered to be mutation caused by alteration of the primary structure of DNA [1,2].In recent years, an almost linear relationship has been obtained between mutagenic potency determined by the Ames test and carcinogenic potency in animals. It has also been demonstrated by Ames and his colleagues that 90% of known human carcinogens are mutagenic[3,4]. -
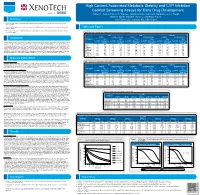
High Content Automated Metabolic Stability and CYP Inhibition Cocktail Screening Assays for Early Drug Development a DIVISION of Robert T
High Content Automated Metabolic Stability and CYP Inhibition Cocktail Screening Assays for Early Drug Development A DIVISION OF Robert T. Grbac, Forrest A. Stanley, Tomoko Ambo, Joanna E. Barbara, Lois J. Haupt, Brian D. Smith, David B. Buckley, and Faraz Kazmi Overview XenoTech, LLC, Lenexa, KS, USA 66219 • The purpose of this study was to develop higher throughput methods to determine metabolic stability and CYP inhibition for drug discovery groups. • Automated liquid handlers, substrate cocktails, and generic LC/MS/MS methods were used to determine metabolic stability and CYP Tables and Figures inhibition endpoints. • The metabolic stability and CYP inhibition profiles of the compounds studied were consistent with known data, indicating the utility of both screening assays. Table 1. Summary of metabolic stability endpoints in liver microsomes from three species Rat Dog Human Introduction NADPH NADPH+UDPGA NADPH NADPH+UDPGA NADPH NADPH+UDPGA Compound CLint CLint CLint CLint CLint CLint t1/2 (min) (μl/min/mg t1/2 (min) (μl/min/mg t1/2 (min) (μl/min/mg t1/2 (min) (μl/min/mg t1/2 (min) (μl/min/mg t1/2 (min) (μl/min/mg Metabolic stability and cytochrome P450 (CYP) inhibition are important parameters to determine earlier in the drug development process and are now increasingly assessed during early drug discovery. The evaluation of metabolic stability is important because the parameters of protein) protein) protein) protein) protein) protein) 7-HC >120 ND 19.6 70.8 >120 ND 3.70 376 >120 ND 2.73 508 half-life (t1/2) and the elimination rate constant (kel) can be used to determine in vitro intrinsic clearance (CLint) which can then be scaled to estimate in vivo intrinsic clearance. -

Modulation of Rat Hepatic CYP1A and 2C Activity by Honokiol and Magnolol: Differential Effects on Phenacetin and Diclofenac Pharmacokinetics in Vivo
molecules Article Modulation of Rat Hepatic CYP1A and 2C Activity by Honokiol and Magnolol: Differential Effects on Phenacetin and Diclofenac Pharmacokinetics In Vivo Sang-Bum Kim 1,2, Kyu-Sang Kim 2, Heon-Min Ryu 2, Seong-Ho Hong 3, Bo-Kyoung Kim 1, Dae-Duk Kim 2, Jin Woo Park 4,* and In-Soo Yoon 5,* ID 1 New Drug Development Center, Daegu-Gyeongbuk Medical Innovation Foundation, Daegu 41061, Korea; [email protected] (S.-B.K.); [email protected] (B.-K.K.) 2 College of Pharmacy and Research Institute of Pharmaceutical Sciences, Seoul National University, Seoul 08826, Korea; [email protected] (K.-S.K.); [email protected] (H.-M.R.); [email protected] (D.-D.K.) 3 Biomedicine Lab, CKD Research Institute, Gyeonggi 16995, Korea; [email protected] 4 Department of Pharmacy, College of Pharmacy and Natural Medicine Research Institute, Mokpo National University, Jeonnam 58554, Korea 5 Department of Manufacturing Pharmacy, College of Pharmacy, Pusan National University, Busan 46241, Korea * Correspondence: [email protected] (J.W.P.); [email protected] (I.-S.Y.); Tel.: +82-61-450-2704 (J.W.P.); +82-51-510-2806 (I.-S.Y.) Received: 24 April 2018; Accepted: 16 June 2018; Published: 17 June 2018 Abstract: Honokiol (2-(4-hydroxy-3-prop-2-enyl-phenyl)-4-prop-2-enyl-phenol) and magnolol (4-Allyl-2-(5-allyl-2-hydroxy-phenyl)phenol) are the major active polyphenol constituents of Magnolia officinalis (Magnoliaceae) bark, which has been widely used in traditional Chinese medicine (Houpu Tang) for the treatment of various diseases, including anxiety, stress, gastrointestinal disorders, infection, and asthma.