Download File
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Second Health Care in the Central Highlands Project
Social Monitoring Report Project Number: 44265-013 Semi-annual Report (January-June 2018) July 2018 VIE: Second Health Care in the Central Highlands Project Prepared by the Ministry of Health, Central Project Management Unit for the Asian Development Bank. This social monitoring report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. Your attention is directed to the “terms of use” section of this website. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. Abbreviations ADB Asian Development Bank CHS Commune health stations CPC Commune People’s Committee CPMU Central Project Management Unit CRC Compensation and Resettlement Committee DNRE Department of Natural Resources and Environment DOF Department of Finance DPs Displaced Persons DPC District People’s Committee GOV Government of Vietnam ICP Inter-communal polyclinics LURC Land Use Right Certificate MOF Ministry of Finance MOH Ministry of Health SPS Safeguard Policy Statement PAH Project Affected Households PPC Provincial People’s Committee PPMU Provincial Project Management Unit PRB Provincial Resettlement Board RP Resettlement Plan RPF Resettlement Policy framework ToR Term of Reference USD US Dollar VND Viet Nam Dong Content ABBREVIATIONS I. INTRODUCTION 1 1.1. Project Introduction 1 1.2. Introduction of Semi- annual social monitoring report 2 II. -

Gia-Lai-Electricity-Joint-Stock-Company
2018 ANNUAL REPORT ABBREVIATIONS AGM : Annual General Meeting BOD : Board Of Directors BOM : Board Of Management CAGR : Compounded Annual Growth Rate CEO : Chief Executive Officer COD : Commercial Operation Date CG : Corporate Governance CIT : Corporate Income Tax COGS : Cost Of Goods Sold EBIT : Earnings Before Interest and Taxes EBITDA : Earnings Before Interest, Taxes, Depreciation And Amortization EGM : Extraordinary General Meeting EHSS : Enviroment - Health - Social Policy - Safety EPC : Engineering Procurement and Construction EVN : Viet Nam Electricity FiT : Feed In Tariff FS : Financial Statement GEC : Gia Lai Electricity Joint Stock Company HR : Human Resources JSC : Joint Stock Company LNG : Liquefied Natural Gas M&A : Mergers and Acquisitions MOIT : Ministry Of Industry and Trade NPAT : Net Profit After Taxes SG&A : Selling, General And Administration PATMI : Profit After Tax and Minority Interests PBT : Profit Before Tax PPA : Power Purchase Agreement R&D : Research and Development ROAA : Return On Average Assets ROAE : Return On Average Equity YOY : Year On Year GEC's Head Office 2 2018 ANNUAL REPORT www.geccom.vn 3 TABLE OF CONTENTS CÔNG TY CP ĐIN GIA LAI 02 ABBREVIATIONS 04 TABLE OF CONTENTS 06 REMARKABLE FIGURES 10 COMMITMENTS AND RESPONSIBILITIES 12 Vision - Mission - Core value 13 17 sustainable development goals of United Nations 18 Commitments to the truth and fairness the 2018 Annual Report 20 Interview with Chairman of the Board 24 Profile of the Board of Directors 28 Letter to Shareholders from the CEO 32 Profile -
CROPWAT Model (Calculate at District Scale) the Amount of Water Demand
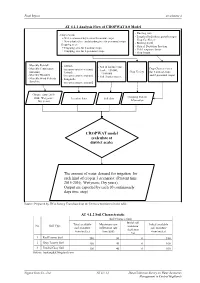
Final Report Attachment 4 AT 4.1.1 Analysis Flow of CROPWAT 8.0 Model - Planting date -Crop season: - Length of individual growth stages + Wet season and dry season for annual crops - Crop Coefficient + New planted tree and standing tree for perennial crops - Rooting depth - Cropping area: - Critical Depletion Fraction + Cropping area for 8 annual crops - Yield response factor + Cropping area for 6 perennial crops - Crop height - Monthly Rainfall - Altitude - Soil & landuse map - Monthly Temperature Crop Characteristics (in representative station) (scale: 1/50.000; (max,min ) Crop Variety (for 8 annual crops - Latitude 1/100.000) - Monthly Humidity and 6 perennial crops) (in representative station) - Soil characteristics. - Monthly Wind Velocity - Longitude - Sunshine (in representative station) Climate data ( 2015- Cropping Pattern 2016; Wet years; Location data Soil data Dry years) Information CROPWAT model (calculate at district scale) The amount of water demand for irrigation for each kind of crop in 3 scenarios: (Present time 2015-2016; Wet years; Dry years). Output are exported by each 10 continuously days time step) Source: Prepared by JICA Survey Team based on the Decrees mentioned in the table. AT 4.1.2 Soil Characteristic Soil Characteristic Initial soil Total available Maximum rain Initial available No Soil Type moisture soil moisture infiltration rate soil moisture depletion (mm/meter) (mm/day) (mm/meter) (%) 1 Red Loamy Soil 180 30 0 180 2 Gray Loamy Soil 160 40 0 160 3 Eroded Gray Soil 100 40 0 100 Source: baotangdat.blogspot.com Nippon Koei Co., Ltd. AT 4.1.1-1 Data Collection Survey on Water Resources Management in Central Highlands Final Report Attachment 4 AT 4.1.3 Soil Type Distribution per District Scale No. -
Final Report of Douc Langur
Final Report Prepared by Long Thang Ha A field survey for the grey-shanked douc langurs (Pygathrix cinerea ) in Vietnam December/2004 Cuc Phuong, Vietnam A field survey on the grey-shanked douc langurs Project members Project Advisor: Tilo Nadler Project Manager Frankfurt Zoological Society Endangered Primate Rescue Centre Cuc Phuong National Park Nho Quan District Ninh Binh Province Vietnam 0084 (0) 30 848002 [email protected] Project Leader: Ha Thang Long Project Biologist Endangered Primate Rescue Centre Cuc Phuong National Park Nho Quan District Ninh Binh Province Vietnam 0084 (0) 30 848002 [email protected] [email protected] Project Member: Luu Tuong Bach Project Biologist Endangered Primate Rescue Centre Cuc Phuong National Park Nho Quan District Ninh Binh Province Vietnam 0084 (0) 30 848002 [email protected] Field Staffs: Rangers in Kon Cha Rang NR And Kon Ka Kinh NP BP Conservation Programme, 2004 2 A field survey on the grey-shanked douc langurs List of figures Fig.1: Distinguished three species of douc langurs in Indochina Fig.2: Map of surveyed area Fig.3: An interview in Kon Cha Rang natural reserve area Fig.4: A grey-shanked douc langur in Kon Cha Rang natural reserve area Fig.5: Distribution of grey-shanked douc in Kon Cha Rang, Kon Ka Kinh and buffer zone Fig.6: A grey-shanked douc langur in Kon Ka Kinh national park Fig.7: Collecting faeces sample in the field Fig.8: A skull of a douc langur collected in Ngut Mountain, Kon Ka Kinh NP Fig.9: Habitat of douc langur in Kon Cha Rang Fig.10: Habitat of douc langur in Kon Ka Kinh Fig.11: Stuffs of douc langurs in Son Lang village Fig.12: Traps were collected in the field Fig.13: Logging operation in the buffer zone area of Kon Cha Rang Fig.14: A civet was trapped in Kon Ka Kinh Fig.15: Illegal logging in Kon Ka Kinh Fig.16: Clear cutting for agriculture land Fig.17: Distribution of the grey-shanked douc langur before survey Fig.18: Distribution of the grey-shanked douc langur after survey Fig.19: Percentage of presence/absence in the surveyed transects. -

An Investment Plan for Kon Ka Kinh Nature Reserve, Gia Lai Province, Vietnam
BirdLife International Vietnam Programme and the Forest Inventory and Planning Institute with financial support from the European Union An Investment Plan for Kon Ka Kinh Nature Reserve, Gia Lai Province, Vietnam A Contribution to the Management Plan Conservation Report Number 11 BirdLife International European Union FIPI An Investment Plan for Kon Ka Kinh Nature Reserve, Gia Lai Province, Vietnam A Contribution to the Management Plan by Le Trong Trai Forest Inventory and Planning Institute with contributions from Le Van Cham, Tran Quang Ngoc and Tran Hieu Minh Forest Inventory and Planning Institute and Nguyen Van Sang, Alexander L. Monastyrskii, Benjamin D. Hayes and Jonathan C. Eames BirdLife International Vietnam Programme This is a technical report for the European-Union-funded project entitled: Expanding the Protected Areas Network in Vietnam for the 21st Century. (Contract VNM/B7-6201/IB/96/005) Hanoi May 2000 Project Coordinators: Nguyen Huy Phon (FIPI) Vu Van Dung (FIPI) Ross Hughes (BirdLife International) Field Survey Team: Le Trong Trai (FIPI) Le Van Cham (FIPI) Tran Quang Ngoc (FIPI) Tran Hieu Minh (FIPI) Nguyen Van Sang (BirdLife International) Alexander L. Monastyrskii (BirdLife International) Benjamin D. Hayes (BirdLife International) Jonathan C. Eames (BirdLife International) Nguyen Van Tan (Gia Lai Provincial Forest Protection Department) Do Ba Khoa (Gia Lai Provincial Forest Protection Department) Nguyen Van Hai (Gia Lai Provincial Forest Protection Department) Maps: Mai Ky Vinh (FIPI) Project Funding: European Union and BirdLife International Cover Illustration: Rhacophorus leucomystax. Photo: B. D. Hayes (BirdLife International) Citation: Le Trong Trai, Le Van Cham, Tran Quang Ngoc, Tran Hieu Minh, Nguyen Van Sang, Monastyrskii, A. -

Download 6.09 MB
Initial Environmental Examination June 2021 Viet Nam: Climate Adaptation through Irrigation Modernization Project Prepared by the Ministry of Agriculture and Rural Development for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 23 June 2021) Currency unit – dong (D) D1.00 = $0.000043 $1.00 = D23,017 ABBREVIATIONS ADB – Asian Development Bank AH – affected household AP – affected person CAIMP – Climate Adaptation through Irrigation Modernization Project CaCO3 – calcium carbonate CHR – central highland region CO – carbon monoxide CPO – Central Project Office CRVA – Climate Risk and Vulnerability Assessment DARD – Department of Agriculture and Rural Development DONRE – Provincial Department of Natural Resources and Environment EA – executing agency EHS – Environment, Health and Safety EIA – environmental impact assessment EMP – environmental management plan EPA – Environmental Police Agency ERP – Emergency Response Plan FS – feasibility study FY – fiscal year GAP – good agricultural practices GDP – gross domestic product GOV – Government of Viet Nam GRM – grievance redress mechanism HDPE – high-density polyethylene HH – household IA – implementing agency IBAT – Integrated Biodiversity Assessment Tool ICM – Integrated Crop Management IEE – initial environmental examination IMC – Irrigation Management Company IPM – integrated pest management IS – irrigation system IUCN – International Union for the Conservation of Nature KBA – key biodiversity areas LEP – Law on Environmental Protection MARD – Ministry of Agriculture and Rural Development -

List of Districts of Vietnam
S.No Province Name of District 1 An Giang Province An Phú 2 An Giang Province Châu Đốc 3 An Giang Province Châu Phú 4 An Giang Province Châu Thành 5 An Giang Province Chợ Mới 6 An Giang Province Long Xuyên 7 An Giang Province Phú Tân 8 An Giang Province Tân Châu 9 An Giang Province Thoại Sơn 10 An Giang Province Tịnh Biên 11 An Giang Province Tri Tôn 12 Bà Rịa–Vũng Tàu Province Bà Rịa 13 Bà Rịa–Vũng Tàu Province Châu Đức 14 Bà Rịa–Vũng Tàu Province Côn Đảo 15 Bà Rịa–Vũng Tàu Province Đất Đỏ 16 Bà Rịa–Vũng Tàu Province Long Điền 17 Bà Rịa–Vũng Tàu Province Tân Thành 18 Bà Rịa–Vũng Tàu Province Vũng Tàu 19 Bà Rịa–Vũng Tàu Province Xuyên Mộc 20 Bắc Giang Province Bắc Giang 21 Bắc Giang Province Hiệp Hòa 22 Bắc Giang Province Lạng Giang 23 Bắc Giang Province Lục Nam 24 Bắc Giang Province Lục Ngạn 25 Bắc Giang Province Sơn Động 26 Bắc Giang Province Tân Yên 27 Bắc Giang Province Việt Yên 28 Bắc Giang Province Yên Dũng 29 Bắc Giang Province Yên Thế 30 Bắc Kạn Province Ba Bể 31 Bắc Kạn Province Bắc Kạn 32 Bắc Kạn Province Bạch Thông 33 Bắc Kạn Province Chợ Đồn 34 Bắc Kạn Province Chợ Mới 35 Bắc Kạn Province Na Rì 36 Bắc Kạn Province Ngân Sơn 37 Bắc Kạn Province Pác Nặm 38 Bạc Liêu Province Bạc Liêu 39 Bạc Liêu Province Đông Hải 40 Bạc Liêu Province Giá Rai 41 Bạc Liêu Province Hòa Bình 42 Bạc Liêu Province Hồng Dân 43 Bạc Liêu Province Phước Long 44 Bạc Liêu Province Vĩnh Lợi 45 Bắc Ninh Province Bắc Ninh 46 Bắc Ninh Province Gia Bình www.downloadexcelfiles.com 47 Bắc Ninh Province Lương Tài 48 Bắc Ninh Province Quế Võ 49 Bắc Ninh Province Thuận -

(Pygathrix Cinerea) at Kon Ka Kinh National Park, Vietnam
Vietnamese Journal of Primatology (2012) vol. 2 (1), 25-35 The feeding behaviour and phytochemical food content of grey-shanked douc langurs ( Pygathrix cinerea ) at Kon Ka Kinh National Park, Vietnam Nguyen Thi Tinh, Ha Thang Long, Bui Van Tuan, Tran Huu Vy and Nguyen Ai Tam Frankfurt Zoological Society, Vietnam Primate Conservation Programme, K83/10D Trung Nu Vuong Street, Hai Chau, Danang, Vietnam Corresponding author: Ha Thang Long <[email protected]> Key words: Pygathrix cinerea , grey-shanked douc langur, feeding behaviour, diet, nutrition, Kon Ka Kinh National Park Summary The grey-shanked douc langur 1 is a critically endangered and endemic leaf-eating primate to Vietnam. The population of the species is decreasing and highly fragmented due to hunting pressure and loss of habitat. The species is restricted to several provinces in the Central Highlands. Kon Ka Kinh National Park is home of less than 250 individuals. Currently, there is insufficient understanding about the feeding behaviour and phytochemical content in food selection among the species. This study was conducted in Kon Ka Kinh National Park from February 2009 to June 2010. We collected 212 hours of feeding behaviour data. Grey schanked douc langurs ate 135 plant species of 44 plant families during the study period. The plant species Pometia pinnata is the most preferred item. We collected 33 plant samples from eaten species for phytochemical analysis which revealed that protein comprised of 11.4% of dry matter, lipids 2.6%, minerals 5.0%, sugar 4.9%, starch 12.8%, and Neutral Detergent Fiber (NDF) 40.8%. Protein in leaves is higher than in whole fruits: 12.8% and 8.3% respectively. -

CO2 Sequestration in Agroforesrty Litsea and Cassava
SOUTHEAST ASIAN NETWORK FOR AGROFORESTRY EDUCATION – SEANAFE VIETNAM NEWORK FOR AGROFORESTRY EDUCATION - VNAFE CO2 SEQUESTRATION ESTIMATION FOR THE LITSEA-CASSAVA AGROFORESTRY MODEL IN MANG YANG DISTRICT, GIA LAI PROVINCE IN THE CENTRAL HIGHLANDS OF VIETNAM Assoc. Prof. Dr. BAO HUY This research was sponsored by the Swedish International Development Cooperation Agency (Sida) through the World Agroforestry Center (ICRAF) and SEANAFE 2010 LIST OF PARTICIPANTS IN THE RESEARCH No. Name Academic Responsibility Organization title, degree 1 Bao Huy Assoc. Prof. Author Department of Forest Resource and Dr. Environmental Management , Agricultural and Forest Faculty, Tay Nguyen University 2 Vo Hung Dr. Member. Silvicultural Department, Agricultural Collection and and Forest Faculty, Tay Nguyen analysis of University intermediate data 3 Pham Doan Quoc Student Field data Forestry course of K2004, Agricultural Vuong collection and Forest Faculty, Tay Nguyen University 4 Ho Dinh Bao Student Field data Forest Resource and Environmental collection Management course of K2004, Agricultural and Forest Faculty, Tay Nguyen University 5 Staff of District Bachelor Field data People’s committee of Mang Yang People’s Committee collection District, Gia Lai province and Department of Agricultural and Rural Development of Mang Yang district (Mr. Loi, Mr. Kinh, and Mr. Quyen 6 Famers who own the Provide Villages of H’Lim and Groi belong to agroforestry model: information. communes of Lơ Pang and Kon Thụp, Kai, Tuch, Lap, Ybyưk Field data Mang Yang district, Gia Lai province collection 2 ACKNOWLEDGEMENTS In completing this research, we are grateful to: The Leaders of the People’s Committee of Mang Yang District of Gia Lai province, and the two communes of Lơ Pang and Kon Thụp that supported us in approaching the farmers, and providing information and the database on socio-economic aspects of the area. -

Viet Nam: Emergency Appeal N° MDRVN006 GLIDE N° FL-2009-000207-VNM Floods and Typhoons 2 March 2011
Final report Viet Nam: Emergency appeal n° MDRVN006 GLIDE n° FL-2009-000207-VNM Floods and typhoons 2 March 2011 Period covered by this Final Report: 2 October 2009 to 30 November 2010 Appeal target (current): CHF 4,464,332 (USD.3.9 million or EUR 3.22 million) Final appeal coverage: This appeal is 101 per cent covered. <view the final financial report, or contact details> Appeal history: • Operations update no. 9 extended the period of this appeal by two months to 30 November 2010. • A second revised emergency appeal was launched on 12 June 2010 for CHF 4,466,630 (USD 3.9 million or EUR 3.23 million) to assist 60,000 families (approximately 270,000 people) for 12 months. • The initial revised emergency appeal was launched on 19 October 2009 for CHF 5,571,176 (USD 5.47 million or EUR 3.67 million) to assist 60,000 families (approximately 270,000 people) for 12 months. • This emergency appeal was initially launched on a preliminary basis on 2 October 2009 for CHF 4,939,626 (USD 4.75 million or EUR 3.25 million) to assist 50,000 families (approximately 210,000 people) for 12 months. • Disaster Relief Emergency Fund (DREF): CHF 314,064 (USD 324,167 or EUR 214,633) was allocated from IFRC’s DREF to support the national society in its initial emergency response. Summary: The Viet Nam Red Cross (VNRC) received constant support from IFRC and partner national societies in-country throughout this operation. This covered support for both service delivery and for technical support which was conveyed in a manner to ensure the expansion of the national society’s capacities. -

Climate Change and Sustainable
NATIONAL ECONOMICS UNIVERSITY Taiwan Studies Project INTERNATIONAL CONFERENCE Climate Change and Sustainability Management in Vietnam and Taiwan ICCSM-2020 Hanoi, 28th October 2020 LABOUR - SOCIAL PUBLISHING HOUSE INTERNATIONAL CONFERENCE Climate Change and Sustainability Management in Vietnam and Taiwan ICCSM-2020 Steering Committee 1. Tran Tho Dat (Prof., PhD), Head of Steering Committee 2. Bui Duc Tho (Assoc. Prof., PhD), Deputy Head of Steering Committee 3. Dinh Duc Truong (Assoc. Prof., PhD), Member Organizing Committee 1. Bui Duc Tho (Assoc. Prof., PhD), Head of Organizing Committee 2. Dinh Duc Truong (Assoc. Prof., PhD), Deputy Head of Organizing Committee 3. Vu Thi Hoai Thu (Assoc. Prof., PhD), Member 4. Pham Thi Bich Chi (Assoc. Prof., PhD), Member 5. Trinh Mai Van (PhD), Member 6. Pham Sy Long (MA), Member 7. Bui Duc Dung (MA), Member 8. Vu Trong Nghia (PhD), Member 9. Nguyen Cong Thanh (PhD), Member 10. Nguyen Dieu Hang (PhD, Member 11. Nguyen Linh Dan (PhD), Member 12. Nguyen Thuy Linh (MSc), Member 13. Tran Ngoc Thuy (MA), Member 14. Bui Huy Hoan (BA), Member Editorial Board 1. Vu Thi Hoai Thu (Assoc. Prof., PhD), Head of Editorial Board 2. Nguyen Cong Thanh (PhD), Deputy Head of Editorial Board 3. Nguyen Dieu Hang (PhD), Member 4. Nguyen Linh Dan (PhD), Member 5. Nguyen Thuy Linh (MSc), Member No. Topic/Authors Page PART I: CLIMATE CHANGE ICCSM-01 The Relationship between Carbon Dioxide Emissions, Energy 1 Consumption, Economic Growth, and Urbanization in Vietnam Nguyen Anh Tru ICCSM-02 Ethnic Minority Farmers’ Perception -

New Archaeological Discoveries in the Geological Formations and Heritages Along the Ba River Ancient Valley
VNU Journal of Science: Earth and Environmental Sciences, Vol. 36, No. 3 (2020) 55-69 Original Article New Archaeological Discoveries in The Geological Formations and Heritages along the Ba River Ancient Valley La The Phuc1, Luong Thi Tuat1, Bui Van Thom2, Nguyen Khac Su3, Vu Tien Duc4, Bui Quang Anh1, Nguyen Trung Minh1, Dang Thi Hai Yen1 1Vietnam National Museum of Nature, Vietnam Academy of Science and Technology, 18 Hoang Quoc Viet, Ha Noi, Vietnam 2Institute of Geological Sciences, Vietnam Academy of Science and Technology, 84 Chua Lang, Dong Da, Hanoi, Vietnam 3Vietnam Archaeological Association, 61 Phan Chu Trinh, Hoan Kiem, Hanoi, Vietnam 4Institute of Social Sciences of Central Highlands, 1A Nguyen Van Linh, Buon Ma Thuot, Dak Lak, Vietnam Received 28 April 2020 Revised 08 September 2020; Accepted 14 September 2020 Abstract: In dry season of 2019, a series of new mix-heritages containing both of natural/geological and prehistoric archaeological values were discovered along the Ba river ancient valley by the field survey team of the project TN17/T06. The archaeological relics were uncovered right in the geological heritage sites such as: waterfalls, fossil sites, ancient terraces, and low mountain slopes along the Ba river ancient valley, which belong to eluvial, deluvial, proluvial and alluvial formations of Pleistocene age. Hundreds of stone tools, including dozens of petrified wood tools were collected, such as: uni-facial and bi-facial tools, end-chooper, side-chopper, scraper, spearhead tool, flake and core tools, etc. The materials of the tools were made of quartz, quartzite, siliceous stone, opal- chalcedony, petrified wood and basalt, which were recognized as geological heritages (A type: Paleontology; D type: Rock; F type: Minerals, according to the classification in the Circular 50/2017-TT-BTNMT of MONRE) of the heritage region.