Health Services Utilization Under Qassam Rocket Attacks
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Yeshivat Derech Chaim Kiryat Gat American Friends of Sderot Amutat Lapid the Max & Ruth Schwartz Hesder Institutions Mission Statement
ech Chaim er K i D r t y a a v t i G h s a e t Y The Friedberg Community Initiative Program The Yedidut-Toronto Foundation Yeshivat Derech Chaim Kiryat Gat American Friends of Sderot Amutat Lapid The Max & Ruth Schwartz Hesder Institutions Mission Statement Giving back to the community is no burden on our students – it is the direct, inescapable consequence of their studies here. It is not in vain that our Yeshiva is called "Derech Chaim" – the "Path of Life". We make every effort to make it clear to our students that the Torah that they study here is not theoretical – it is geared is to lead and direct them to take those same high ideals and put them into practice in their daily lives - in their hobbies, careers and life-choices. The Rashbi Study Partners Program Twice a week, Kiryat Gat Hesder students go to study Talmud and Parshat Shavua with young students at the nearby "Rashbi" Mamlachti Dati elementary school. Due to its proximity our students can now engage in this activity twice a week and the young children are in turn encouraged to visit the Yeshiva as well. In general, these children come from very economically and religiously challenged backgrounds. Having a "big brother" from the local Hesder Yeshiva is invaluable in building their respect for Torah and connecting them to proper role models. Community Rabbinate Program Amit L’Mishpacha A number of our Rabbis also serve as the beloved The Family Associate Program spiritual leaders of different local congregations. In this context, they are busy giving talks and lectures as well as helping families in their community in various ways. -

Emergency in Israel
Emergency in Israel Emergency Update on Jewish Agency Programming May 16, 2021 The recent violent events that have erupted across the country have left us all surprised and stunned: clashes with Palestinians in Jerusalem and on the Temple Mount; the deteriorating security tensions and the massive barrage of missiles from Gaza on southern and central Israel; and the outbreak of unprecedented violence, destruction, and lynching in mixed cities and Arab communities. To say that the situation is particularly challenging is an understatement. We must all deal with the consequences of the current tensions. Many of us are protecting family, coworkers, or people under our charge while missiles fall on our heads night and day, forcing us to seek shelter. We have all witnessed the unbearable sights of rioting, beating, and arson by Arab and Jewish extremists in Lod, Ramla, Acre, Kfar Qassem, Bat Yam, Holon, and other places. As an organization that has experienced hard times of war and destruction, as well as periods of prosperity and peace, it is our duty to rise up and make a clear statement: we will support and assist populations hit by missile fire as we did in the past, after the Second Lebanon War and after Operations Cast Lead and Protective Edge. Together with our partners, we will mobilize to heal and support the communities and populations affected by the fighting. Our Fund for Victims of Terror is already providing assistance to bereaved families. When the situation allows it, we will provide more extensive assistance to localities and communities that have suffered damage and casualties. -

The Regional Council of Yoav Photo: Lotem Friedland | Design: Kachald
The Regional Council of Yoav Photo: Lotem Friedland | Design: KachalD Tourism Our Vision Hot Springs > Hamei-Yoav Hot Springs is a natural thermo mineral spa. A Municipality composed of multi-generational communities Bet Guvrin > a large national park, which encompasses the sites of an that prosper and renew themselves, maintaining a quality of ancient agricultural settlement of Maresha, and the ancient town of Bet life which guards their specific rural essence, lead by local Guvrin, including many historical caves. Caves of Maresha and Bet Guvrin leadership. recently has inscribed on the World Heritage list by UNESCO. Tending our open spaces and countryside, nature, and the Iron Age sites > One of the largest Iron Age sites in Israel is located in heritage that is special to the Yoav area. Kibbutz Revadim. More than 100 ancient oil presses were discovered there, Excellence in education, fostering culture and social welfare as well as an inscription that clearly identifies the site as Philistine Ekron. services for our residents. Tel Zafit > located inside Tel Zafit National Park. Recent ongoing excavations The joint responsibility of our population and communities for at this Biblical site have produced substantial evidence of siege and security, ecology, and quality of life. subsequent destruction of the site in the late 9th century BC. Fulfillment of our economic potential, and providing quality Sightseeing > Yoav’s magnificent landscapes provide the perfect setting for employment through the development of agriculture, a wide range of leisure activities, such as cycling, hiking, climbing, wine infrastructures, and country tourism, in cooperation with our tasting, gourmet and popular dining, and various festivals such as the neighbouring municipalities renowned Biblical festival. -

Sderot – the Central Hesder Yeshiva and the “Shluchot” Revolution!
Sderot – The Central Hesder Yeshiva and the “Shluchot” Revolution! The Torah Revolution in Sderot The Central Max and Ruth Schwartz Hesder Yeshiva of Sderot was founded over 15 years ago and now has more than 400 students. The rapid growth of the Yeshiva despite the thousands of missiles aimed at Sderot, together with the construction of a magnificent campus has served to strengthen the spirit of all the residents and uplift the status of Torah throughout the region. Over the years Sderot has become just about the largest Hesder Yeshiva in Israel and is blessed with a very high religious and scholastic level. 400 strong in the main study hall Unique Outreach Affiliate Institutions The Rosh Yeshiva, Rabbi David Fendel, a literal powerhouse behind so many local projects - both spiritual and material – came on Aliyah from the United States to build both his home and a world of Torah in Sderot. In addition to building our main Hesder institution, Rabbi Fendel led a true revolution in the yeshiva world when he insisted on establishing and receiving official recognition for 2 affiliate institutions (“Shluchot” in Hebrew) serving a more varied clientele than other Hesder Yeshivot. Rav Fendel believed that with the right approach, with a warm and unique staff it would be possible to reach out and attract graduates of regular religious high schools and turn them into proud Torah-true Jews and soldiers imbued with deep faith and self- sacrifice. To achieve this goal Sderot has established two affiliates– Yeshivat Lev La’Daat also in Sderot led by Rabbi Shlomo Binyamin now numbering about 130 students and Yeshivat Derech Chaim in Kiryat Gat headed by Rabbi Amir Maman with over 70 students. -

CERTIFICATE This Is to Certify That the Information Security Management System of HP INDIGO LTD
CERTIFICATE This is to certify that the Information Security Management System of HP INDIGO LTD. 10, Einstein St. , Ness Ziona , Israel Has been assessed and complies with the requirements of : ISO/IEC 27001:2013 This Certificate is Applicable to Business processes: Development, manufacturing and technical support of HP Indigo products. System/products: The HP indigo information systems and services required to deliver and support HP Indigo digital presses, HP Production Pro servers (DFE) and software solutions. According to Statement of Applicability: Version: 2.0, Date: Jannuary 20th 2019 Certificate No.: 101898 Certificate Issue Date: 05/02/2019 Initial Certification Date: 05/02/2019 Certification Expiry Date: 04/02/2022 SII-QCD assumes no liability to any party other than the client, and then only in accordance with the agreed upon Certification Agreement. This certificate’s validity is subject to the organization maintaining their system in accordance with SII-QCD requirements for system certification. The continued validity may be verified via scanning the code with a smartphone, or via website www.sii.org.il. This certificate remains the property of SII-QCD. Ilan Carmit Avital Weinberg Acting Director General R.N 511468464 Director, Quality & Certification Division Page 1 of 2 Our Vision: To Enhance Both Global Competitiveness of our Services, with our Uncompromised Quality and Integrity Annex to Certificate of Registration no. 101898 HP INDIGO LTD. 10, Einstein St. , Ness Ziona , Israel With Additional Sites At: HP Indigo Ltd. -
H. Res. 951 in the House of Representatives, U
H. Res. 951 In the House of Representatives, U. S., March 5, 2008. Whereas more than 4,000 rockets and mortar shells have been fired at Israel from the Gaza Strip by Hamas and other terrorist organizations since Israeli forces withdrew from there in 2005; Whereas, since January 1, 2008, terrorists have fired nearly a thousand rockets and mortar shells into Israel; Whereas the near-daily rocket fire has been targeted pri- marily and intentionally at civilian communities in Israel, such as Sderot and Ashkelon, making life in such areas agonizing; Whereas the terrorist rockets have hit homes, schools, build- ings, roads, power lines, and other such infrastructure in Israel; Whereas these unprovoked rocket and mortar attacks have murdered over a dozen Israelis, inflicted hundreds of cas- ualties, produced thousands of cases of shock and post- traumatic stress, especially among children, and caused severe disruption of daily life; Whereas these deliberate cross-border rocket and mortar at- tacks on civilian populations constitute a blatant violation of human rights and international law; 2 Whereas those responsible for launching rocket attacks against Israel routinely embed their production facilities and launch sites amongst the Palestinian civilian popu- lation, utilizing them as human shields; Whereas intentionally targeting civilian populations and the use of human shields violates international humanitarian and human rights law; Whereas numerous reports have cited the copious amounts of sophisticated weapons, small arms, and weapons manu- -

30 October 2020 SDEROT Shabbat Greetings to Everyone, I Feel That The
Friday Evening Message – 30 October 2020 SDEROT Shabbat greetings to everyone, I feel that the Friday night message is a great idea by the community and hopefully it will continue beyond this time of craziness. I have recently started a new project myself which is reconnecting with friends who I haven’t spoken to for a while, there is nothing as nice as getting a message from someone who we haven’t heard from in ages, especially during these difficult days. So I have started to contact someone every week just to wish them Shabbat Shalom and check in with them. One of those who I have recently reconnected with was a dear friend Stewart Ganullin who happens to be the CEO of an organisation who I volunteered with on my many trips to Israel. Stewart is the amazing head of Hope for Sderot based in what is sadly known as the rocket capital of the world. The small “museum” of Kassam, Grad and Kadyusha rockets in the cities police station is a reminder of the over 16000 rockets to be fired from the nearby Gaza Strip to the civilian population 2km away in Sderot. The “rocket museum” located at Sderot police station. In the year preceding, to the year following, the Gush Katif disengagement rocket attacks on Sderot and surrounding Western Negev increased by ten-fold. Even though those who could afford to flee reducing the city population to less than 20000 it was allowed to retain city status and at the last year’s census had risen to almost 28000. -

Excluded, for God's Sake: Gender Segregation and the Exclusion of Women in Public Space in Israel
Excluded, For God’s Sake: Gender Segregation and the Exclusion of Women in Public Space in Israel המרכז הרפורמי לדת ומדינה -לוגו ללא מספר. Third Annual Report – December 2013 Israel Religious Action Center Israel Movement for Reform and Progressive Judaism Excluded, For God’s Sake: Gender Segregation and the Exclusion of Women in Public Space in Israel Third Annual Report – December 2013 Written by: Attorney Ruth Carmi, Attorney Ricky Shapira-Rosenberg Consultation: Attorney Einat Hurwitz, Attorney Orly Erez-Lahovsky English translation: Shaul Vardi Cover photo: Tomer Appelbaum, Haaretz, September 29, 2010 – © Haaretz Newspaper Ltd. © 2014 Israel Religious Action Center, Israel Movement for Reform and Progressive Judaism Israel Religious Action Center 13 King David St., P.O.B. 31936, Jerusalem 91319 Telephone: 02-6203323 | Fax: 03-6256260 www.irac.org | [email protected] Acknowledgement In loving memory of Dick England z"l, Sherry Levy-Reiner z"l, and Carole Chaiken z"l. May their memories be blessed. With special thanks to Loni Rush for her contribution to this report IRAC's work against gender segregation and the exclusion of women is made possible by the support of the following people and organizations: Kathryn Ames Foundation Claudia Bach Philip and Muriel Berman Foundation Bildstein Memorial Fund Jacob and Hilda Blaustein Foundation Inc. Donald and Carole Chaiken Foundation Isabel Dunst Naomi and Nehemiah Cohen Foundation Eugene J. Eder Charitable Foundation John and Noeleen Cohen Richard and Lois England Family Jay and Shoshana Dweck Foundation Foundation Lewis Eigen and Ramona Arnett Edith Everett Finchley Reform Synagogue, London Jim and Sue Klau Gold Family Foundation FJC- A Foundation of Philanthropic Funds Vicki and John Goldwyn Mark and Peachy Levy Robert Goodman & Jayne Lipman Joseph and Harvey Meyerhoff Family Richard and Lois Gunther Family Foundation Charitable Funds Richard and Barbara Harrison Yocheved Mintz (Dr. -

The Bedouin Population in the Negev
T The Since the establishment of the State of Israel, the Bedouins h in the Negev have rarely been included in the Israeli public e discourse, even though they comprise around one-fourth B Bedouin e of the Negev’s population. Recently, however, political, d o economic and social changes have raised public awareness u i of this population group, as have the efforts to resolve the n TThehe BBedouinedouin PPopulationopulation status of the unrecognized Bedouin villages in the Negev, P Population o primarily through the Goldberg and Prawer Committees. p u These changing trends have exposed major shortcomings l a in information, facts and figures regarding the Arab- t i iinn tthehe NNegevegev o Bedouins in the Negev. The objective of this publication n The Abraham Fund Initiatives is to fill in this missing information and to portray a i in the n Building a Shared Future for Israel’s comprehensive picture of this population group. t Jewish and Arab Citizens h The first section, written by Arik Rudnitzky, describes e The Abraham Fund Initiatives is a non- the social, demographic and economic characteristics of N Negev profit organization that has been working e Bedouin society in the Negev and compares these to the g since 1989 to promote coexistence and Jewish population and the general Arab population in e equality among Israel’s Jewish and Arab v Israel. citizens. Named for the common ancestor of both Jews and Arabs, The Abraham In the second section, Dr. Thabet Abu Ras discusses social Fund Initiatives advances a cohesive, and demographic attributes in the context of government secure and just Israeli society by policy toward the Bedouin population with respect to promoting policies based on innovative economics, politics, land and settlement, decisive rulings social models, and by conducting large- of the High Court of Justice concerning the Bedouins and scale social change initiatives, advocacy the new political awakening in Bedouin society. -

THE CHALLENGE of GAZA: Policy Options and Broader Implications
BROOKINGS 1775 Massachusetts Ave., NW Washington, D.C. 20036-2103 www.brookings.edu ANALYSIS PAPER Number 23, July 2011 THE CHALLENGE OF GAZA: Policy Options and Broader Implications Daniel Byman Gad Goldstein ANALYSIS PAPER Number 23, July 2011 THE CHALLENGE OF GAZA: Policy Options and Broader Implications Daniel Byman Gad Goldstein The Brookings Institution is a private non-profit organization. Its mission is to conduct high-quality, independent research and, based on that research, to provide innovative, practical recommendations for policymakers and the public. The conclusions and recommendations of any Brookings publication are solely those of its author(s), and do not reflect the views of the Institution, its management, or its other scholars. Brookings recognizes that the value it provides to any supporter is in its absolute commitment to quality, independence and impact. Activities supported by its donors reflect this commitment and the analysis and recommendations are not determined by any donation. Copyright © 2011 1775 Massachusetts Avenue, N.W., Washington, D.C. 20036 www.brookings.edu Table of Contents Executive Summary . iv Acknowledgements . ix The Authors . x Introduction . 1 The Nature of the Challenge in Gaza . 3 Factors Beyond Gaza to Consider . 18 Policy Options . 24 THE CHALLENGE OF GAZA: Policy Options and Broader Implications The Saban Center at BRooKings iii Executive Summary lthough both the United States and Israel Hamas draws on many resources to stay in power . devote tremendous attention to the Middle Most notably, Hamas has long exploited its infra- East peace process, the Gaza Strip and its structure of mosques, social services, and communi- HamasA government have continued to vex Ameri- ty organizations to raise money and attract recruits . -

Table of Contents
Table of Contents Page V. The Threat to Israel’s Civilian Population and Israel’s Civil Defense Measures ............106 A. Life under the Threat of Terrorist Rocket Fire and Cross-Border Tunnel Attacks .................................................................................................................106 B. Israel’s Civil Defence Measures against Rocket and Mortar Attacks .................107 1. Passive Defence Measures .......................................................................107 2. Active Defence Measures (the Iron Dome System) ................................111 C. Harm Caused to Israel’s Civilian Population by Rocket and Mortar Attacks .................................................................................................................112 1. Civilian Deaths and Injuries.....................................................................112 2. Effects on Children, Teenagers and College Students .............................118 3. Effect on the Elderly and People with Disabilities ..................................121 4. Internal Displacement ..............................................................................122 5. Psychological Damage .............................................................................125 6. Economic Damage ...................................................................................132 D. Conclusion ...........................................................................................................136 i V. The Threat to Israel’s Civilian Population -
List of All the 122 Burial Societies (Hevra Kadisha- HK) Locality Name of the HK Name of the Addres Zip Phone No
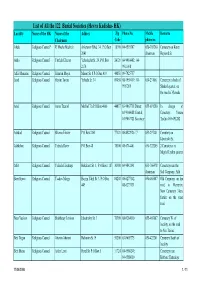
List of All the 122 Burial Societies (Hevra Kadisha- HK) Locality Name of the HK Name of the Addres Zip Phone No. Mobile Remarks Chairman Code phone no. Afula Religious Council* R' Moshe Mashiah Arlozorov Blvd. 34, P.O.Box 18100 04-6593507 050-303260 Cemetery on Keren 2041 chairman Hayesod St. Akko Religious Council Yitzhak Elharar Yehoshafat St. 29, P.O.Box 24121 04-9910402; 04- 2174 9911098 Alfei Menashe Religious Council Shim'on Moyal Manor St. 8 P.O.Box 419 44851 09-7925757 Arad Religious Council Hayim Tovim Yehuda St. 34 89058 08-9959419; 08- 050-231061 Cemetery in back of 9957269 Shaked quarter, on the road to Massada Ariel Religious Council Amos Tzuriel Mish'ol 7/a P.O.Box 4066 44837 03-9067718 Direct; 055-691280 In charge of 03-9366088 Central; Cemetery: Yoram 03-9067721 Secretary Tzefira 055-691282 Ashdod Religious Council Shlomo Eliezer P.O.Box 2161 77121 08-8522926 / 7 053-297401 Cemetery on Jabotinski St. Ashkelon Religious Council Yehuda Raviv P.O.Box 48 78100 08-6714401 050-322205 2 Cemeteries in Migdal Tzafon quarter Atlit Religious Council Yehuda Elmakays Hakalanit St. 1, P.O.Box 1187 30300 04-9842141 053-766478 Cemetery near the chairman Salt Company, Atlit Beer Sheva Religious Council Yaakov Margy Hayim Yahil St. 3, P.O.Box 84208 08-6277142, 050-465887 Old Cemetery on the 449 08-6273131 road to Harzerim; New Cemetery 3 km. further on the same road Beer Yaakov Religious Council Shabbetay Levison Jabotinsky St. 3 70300 08-9284010 055-465887 Cemetery W.