Nursing Home Compare Claims-Based Measures Technical
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

LLT 180 Lecture 22 1 Today We're Gonna Pick up with Gottfried Von Strassburg. As Most of You Already Know, and It's Been Alle
LLT 180 Lecture 22 1 Today we're gonna pick up with Gottfried von Strassburg. As most of you already know, and it's been alleged and I readily admit, that I'm an occasional attention slut. Obviously, otherwise, I wouldn't permit it to be recorded for TV. And, you know, if you pick up your Standard today, it always surprises me -- actually, if you live in Springfield, you might have met me before without realizing it. I like to cook and a colleague in the department -- his wife's an editor for the Springfield paper and she also writes a weekly column for the "Home" section. And so he and I were talking about pans one day and I was, you know, saying, "Well," you know, "so many people fail to cook because they don't have the perfect pan." And she was wanting to write an article about pans. She'd been trying to convince him to buy better pans. And so she said, "Hey, would you pose for a picture with pans? I'm writing this article." And so I said, "Oh, what the heck." And so she came over and took this photo. And a couple of weeks later, I opened Sunday morning's paper -- 'cause I knew it was gonna be in that week -- and went over to the "Home" section. And there was this color photo, about this big, and I went, "Oh, crap," you know. So whatever. Gottfried. Again, as they tell you here, we don't know much about these people, and this is really about love. -

Frequencies Between Serial Killer Typology And
FREQUENCIES BETWEEN SERIAL KILLER TYPOLOGY AND THEORIZED ETIOLOGICAL FACTORS A dissertation presented to the faculty of ANTIOCH UNIVERSITY SANTA BARBARA in partial fulfillment of the requirements for the degree of DOCTOR OF PSYCHOLOGY in CLINICAL PSYCHOLOGY By Leryn Rose-Doggett Messori March 2016 FREQUENCIES BETWEEN SERIAL KILLER TYPOLOGY AND THEORIZED ETIOLOGICAL FACTORS This dissertation, by Leryn Rose-Doggett Messori, has been approved by the committee members signed below who recommend that it be accepted by the faculty of Antioch University Santa Barbara in partial fulfillment of requirements for the degree of DOCTOR OF PSYCHOLOGY Dissertation Committee: _______________________________ Ron Pilato, Psy.D. Chairperson _______________________________ Brett Kia-Keating, Ed.D. Second Faculty _______________________________ Maxann Shwartz, Ph.D. External Expert ii © Copyright by Leryn Rose-Doggett Messori, 2016 All Rights Reserved iii ABSTRACT FREQUENCIES BETWEEN SERIAL KILLER TYPOLOGY AND THEORIZED ETIOLOGICAL FACTORS LERYN ROSE-DOGGETT MESSORI Antioch University Santa Barbara Santa Barbara, CA This study examined the association between serial killer typologies and previously proposed etiological factors within serial killer case histories. Stratified sampling based on race and gender was used to identify thirty-six serial killers for this study. The percentage of serial killers within each race and gender category included in the study was taken from current serial killer demographic statistics between 1950 and 2010. Detailed data -

The Knots Prayer UNDOING KNOTS
UNDOING KNOTS Debra Reyland was searching for a new parish home last year when The Knots Prayer she heard Fr. Jim describe St. Leo’s ministry. She decided to visit one Sunday and said that she immediately felt an attraction and Dear God, believed that God had led her here. A music teacher by background, please untie the knots she wanted to share her gifts and began a children’s choir. Soon she that are in my mind, realized that the children needed more and my heart, and my life. with the help of a group of faithful volunteers Remove the have nots, began the weekly Children’s Liturgy of the the can nots and the do nots Word program that reaches up to 50 children that I have in my mind. during Sunday Mass. It’s her own relationship with God that Erase the will nots, energizes her ministry with the children. She may nots, might nots grew up Protestant and converted to the that find a home in my heart. Catholic faith about 28 years ago. Like some Catholics she struggled with confession. Release me from the could nots, “But not fully understanding the sacramental blessing it offers us would nots, and should nots through God’s mercy and grace, I rationalized in my mind and in my that obstruct my life. heart that it was unnecessary. Besides, it would be so uncomfortable like an itchy, wool sweater and would be And most of all, Dear God, embarrassing to show my less than perfect and sinful self. What I ask that you remove from my mind difference would it make really? I confessed my sins to God all the my heart and my life all of the ‘am nots’ time and that should be enough, I would justify in my mind. -

Mexico: the Vatos Locos Gang, Including Its
Responses to Information Requests - Immigration and Refugee Board of C... http://www.irb-cisr.gc.ca/Eng/ResRec/RirRdi/Pages/index.aspx?doc=45... Home > Research Program > Responses to Information Requests Responses to Information Requests (RIR) respond to focused Requests for Information that are submitted to the Research Directorate in the course of the refugee protection determination process. The database contains a seven-year archive of English and French RIRs. Earlier RIRs may be found on the UNHCR's Refworld website. 13 July 2012 MEX104133.FE Mexico: The Vatos Locos gang, including its organizational structure, areas of influence and activity; information on detention of gang members in 2007 Research Directorate, Immigration and Refugee Board of Canada, Ottawa 1. Origin and Organizational Structure The information presented in this section is coming from a correspondence sent the Research Directorate on the 18 June 2012 by an associate researcher at the Chihuahua College (Colegio de Chihuahua), also member of the UNESCO Chair on drugs in Mexico. Based on his database consisting of around 3,500 archives on gangs in the Americas, the associate researcher indicated that the gang Vatos Locos was created during the 1940s in Los Angeles by Mexicans and Mexican-Americans. During the 1970s and 1980s the gang was partly consolidated in prison, extending its alliances and mode of recruitment. Recent recruits include ex-military personnel returning from Afghanistan and Iraq. Some gangs outside the US probably took the Vatos Locos name from the 1993 film Blood In, Blood Out. Members of Vatos Locos refer to themselves as a "nation" that shares common aspects but still allows each individual gang a certain degree of autonomy. -

City of Walnut Creek
C I T Y 0 F WALNUT CREEK. STANDARD PLANS PUBLIC SERVICES DEPARTMENT 1666 NORTH MAIN STREET WALNUT CREEK, CA 94596 AUGUST 2013 STANDARD PLANS CONTENTS DESCRIPTION DETAIL NO. Storm Drain Details Type 1 Catch Basin SD-1 (Sheets 1-4) Catch Basin on Manhole Base SD-2 Catch Basin Gutter Warping Details SD-3 Storm Drain Manholes SD-4 (Type A, B, C, & D) Manhole Frame and Cover SD-5 Reinforced Concrete Pipe Collar SD-6 Sidewalk Cross Drain SD-7 (Sheets 1-4) Side Connection SD-8 NPDES Medallion SD-9 Concrete Construction Standard Curb, Gutter and Sidewalk CC-1 Residential Driveway Approach CC-2 Commercial Driveway Approach CC-3 Concrete Valley Gutter CC-4 Construction Joints CC-5 Weakened Plane Joints and Score Lines CC-6 Curb Ramp Details CC-7 (Sheets 1-2) Curb Ramp and Island Passageway Details CC-8 (Sheets 1-2) Truncated Domes CC-9 H:\STDPLNS\Standard Plans TOC 2013.doc Page I of3 Traffic Details Pavement Undulation Standards TS-1 Standard Median Tapers TS-2 Standard Median Flares TS-3 Standard Steel Beam Barricade TS-4 Traffic Sign Mounting TS-5 Street Name Sign Location TS-6 Parking Meter Pole Installation TS-7 Street Name Signs TS-8 Sign Installation TS-9 Large Street Name Signs TS-10 Mast Arm Sign Mounting Bracket TS-11 Warning Sign Size Chart TS-12 Typical Lane Closure TS-13-1 Typical Lane Closure (Left Turn Lanes) TS-13-2 Types of Tapers and Buffer Spaces TS-13-3 Typical Lane Closure (Notes) TS-13-4 Typical Lane Closure (Legends and Notes) TS-13-5 Type P and Type M TS-14-1 Traffic Signal Controller Cabinet Signal Pull Box TS-14-2 Traffic -

Judge, Jury, and Executioner: Why Private Parties Have Standing to Challenge an Executive Order That Prohibits ICTS Transactions with Foreign Adversaries
American University Law Review Volume 69 Issue 6 Article 4 2020 Judge, Jury, and Executioner: Why Private Parties Have Standing to Challenge an Executive Order That Prohibits ICTS Transactions with Foreign Adversaries Ari K. Bental American University Washington College of Law Follow this and additional works at: https://digitalcommons.wcl.american.edu/aulr Part of the Law and Politics Commons, and the President/Executive Department Commons Recommended Citation Bental, Ari K. (2020) "Judge, Jury, and Executioner: Why Private Parties Have Standing to Challenge an Executive Order That Prohibits ICTS Transactions with Foreign Adversaries," American University Law Review: Vol. 69 : Iss. 6 , Article 4. Available at: https://digitalcommons.wcl.american.edu/aulr/vol69/iss6/4 This Comment is brought to you for free and open access by the Washington College of Law Journals & Law Reviews at Digital Commons @ American University Washington College of Law. It has been accepted for inclusion in American University Law Review by an authorized editor of Digital Commons @ American University Washington College of Law. For more information, please contact [email protected]. Judge, Jury, and Executioner: Why Private Parties Have Standing to Challenge an Executive Order That Prohibits ICTS Transactions with Foreign Adversaries Abstract On May 15, 2019, President Donald Trump, invoking his constitutional executive and statutory emergency powers, signed Executive Order 13,873, which prohibits U.S. persons from conducting information and communications technology and services (ICTS) transactions with foreign adversaries. Though the executive branch has refrained from publicly identifying countries or entities as foreign adversaries under the Executive Order, observers agree that the Executive Order’s main targets are China and telecommunications companies, namely Huawei, that threaten American national security and competitiveness in the race to provide the lion’s share of critical infrastructure to support the world’s growing 5G network. -

The Walking Dead
THE WALKING DEAD "Episode 105" Teleplay by Glen Mazzara PRODUCERS DRAFT - 7/03/2010 SECOND PRODUCERS DRAFT - 7/09/2010 REV. SECOND PRODUCERS DRAFT - 7/13/2010 NETWORK DRAFT - 7/14/2010 REVISED NETWORK DRAFT - 7/20/2010 Copyright © 2010 TWD Productions, LLC. All rights reserved. No portion of this script may be performed, published, sold or distributed by any means, or quoted or published in any medium including on any web site, without prior written consent. Disposal of this script 2. copy does not alter any of the restrictions set forth above. TEASER FADE IN: No clue where we are. A dark, mysterious shot: TIGHT ANGLE: The back of a MAN'S (Jenner's) head rises into shot, rimmed by top-light. He brings a breather helmet to his unseen face, slips it on over his head. As he tightens the enclosures at the back, a VOICE speaks from everywhere and nowhere, soothing and surreal: VOX Good morning, Dr. Jenner. JENNER Good morning, Vox. VOX How are you feeling this morning? JENNER A bit restless, I have to admit, Vox. A bit...well...off my game. Somewhat off-kilter. VOX That's understandable. JENNER Is it? I suppose it is. I fear I'm losing perspective on things. On what constitutes kilter versus off- kilter. VOX I sympathize. EDWIN JENNER turns to camera, his BUBBLE FACE-SHIELD kicking glare from the overhead lighting, the inside of his mask fogging badly and obscuring his face, as: JENNER Vox, you cannot sympathize. Don't patronize me, please. It messes with my head. -

Do-Gooders and Go-Getters: Selection and Performance in Public Service
DO-GOODERS AND GO-GETTERS: SELECTION AND PERFORMANCE IN PUBLIC SERVICE DELIVERYú Nava Ashraf Oriana Bandiera Scott S. Lee June 12, 2016 Abstract State capacity to provide public services depends on the motivation of the agents recruited to deliver them. We design an experiment to quantify the effect of agent selection on service effectiveness. The experiment, embedded in a nationwide recruitment drive for a new govern- ment health position in Zambia, shows that agents attracted to a civil service career have more skills and ambition than those attracted to “doing good”. Data from a mobile platform, ad- ministrative records, and household surveys show that they deliver more services, change health practices, and produce better health outcomes in the communities they serve. JEL classification: J24, 015, M54, D82. úAshraf: Department of Economics, LSE, [email protected]. Bandiera: Department of Economics and STICERD, LSE, [email protected]. Lee: Harvard Medical School and Harvard Business School, [email protected]. We thank the Ministry of Health of Zambia and especially Mrs. Mutinta Musonda for partnership on this project. We thank the IGC, JPAL Governance Initiative, USAID and HBS DFRD for financial support. We also thank Robert Akerlof, Charles Angelucci, Tim Besley, Robin Burgess, Paul Gertler, Edward Glaeser, Kelsey Jack, Giacomo Ponzetto, Imran Rasul, Jonah Rockoffand seminar participants at several institutions for useful comments. Adam Grant, Amy Wrzesniewski, and Patricia Satterstrom kindly provided guidance on psychometric scales. We thank Kristin Johnson, Conceptor Chilopa, Mardieh Dennis, Madeleen Husselman, Alister Kandyata, Allan Lalisan, Mashekwa Maboshe, Elena Moroz, Shotaro Nakamura, Sara Lowes, and Sandy Tsai, for the excellent research assistance and the Clinton Health Access Initiative in Zambia for their collaboration. -

Publication 523 Reminders
Userid: CPM Schema: tipx Leadpct: 100% Pt. size: 10 Draft Ok to Print AH XSL/XML Fileid: … tions/P523/2020/A/XML/Cycle04/source (Init. & Date) _______ Page 1 of 22 12:06 - 1-Mar-2021 The type and rule above prints on all proofs including departmental reproduction proofs. MUST be removed before printing. Department of the Treasury Contents Internal Revenue Service Future Developments ....................... 1 Publication 523 Reminders ............................... 1 Cat. No. 15044W Introduction .............................. 2 Does Your Home Sale Qualify for the Exclusion of Gain? .............................. 2 Selling Eligibility Test ........................... 3 Does Your Home Qualify for a Partial Your Home Exclusion of Gain? ...................... 6 Figuring Gain or Loss ....................... 7 For use in preparing Basis Adjustments—Details and Exceptions ..... 8 Business or Rental Use of Home ............ 11 Returns 2020 How Much Is Taxable? ..................... 14 Recapturing Depreciation ................. 15 Reporting Your Home Sale .................. 15 Reporting Gain or Loss on Your Home Sale .... 16 Reporting Deductions Related to Your Home Sale ............................... 17 Reporting Other Income Related to Your Home Sale .......................... 17 Paying Back Credits and Subsidies .......... 18 How To Get Tax Help ...................... 18 Index .................................. 22 Future Developments For the latest information about developments related to Pub. 523, such as legislation enacted after it was published, go to IRS.gov/Pub523. Reminders Photographs of missing children. The IRS is a proud partner with the National Center for Missing & Exploited Children® (NCMEC). Photographs of missing children se- lected by the Center may appear in this publication on pa- ges that would otherwise be blank. You can help bring these children home by looking at the photographs and calling 800-THE-LOST (800-843-5678) if you recognize a child. -

An Archaeology of Walls in the Walking Dead
Undead Divides: An Archaeology of Walls in The Walking Dead Howard Williams In 2010, the zombie horror genre gained even greater popularity than the huge following it had previously enjoyed when AMC’s The Walking Dead (TWD) first aired. The chapter surveys the archaeology of this fictional post-apocalyptic material world in the show’s seasons 1–9, focusing on its mural practices and environments which draw upon ancient, biblical, medieval and colonial motifs. The study identifies the moralities and socialities of wall-building, dividing not only survivors aspiring to re-found civilization from the wilderness and manifesting the distinctive identities of each mural community, but also distinguishing the living from the undead. The roles of the dead and the undead in mural iterations are also explored. As such, dimensions of past and present wall-building practices are reflected and inverted in this fictional world. As part of a broader ‘archaeology of The Walking Dead’, the chapter identifies the potentials of exploring the show’s physical barriers within the context of the public archaeology of frontiers and borderlands. Andrea: What’s your secret? The Governor: Really big walls. Andrea: That soldier had walls too and we all know how that turned out, so. The Governor: I guess we do. The real secret is what goes on within these walls. It’s about getting back to who we were, who we really are, not just waiting to be saved. You know people here have homes, medical care, kids go to school. Adults have jobs to do. It’s a sense of purpose. -
Mary-Undoer-Of-Knots Overview-1.Pdf
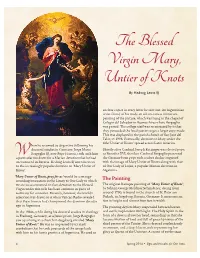
By Hedwig Lewis SJ enclose copies in every letter he sent out. An Argentinian artist-friend of his made an oil-on-canvas miniature painting of the picture, which was hung in the chapel of Colegio del Salvador in Buenos Aires where Bergoglio was posted. The college staff was so attracted by it that they persuaded the local pastor to get a larger copy made. This was displayed in the parish church of San Jose del Talar, in 1996. Eventually, devotion to Mary under the title ‘Untier of Knots’ spread across Latin America. hen he returned to Argentina following his doctoral studies in Germany, Jorge Mario Shortly after Cardinal Joseph Ratzinger was elected pope, Bergoglio SJ, now Pope Francis, took with him as Benedict XVI, the then-Cardinal Bergoglio presented a particular fondness for a Marian devotion that he had the German-born pope with a silver chalice engraved encountered in Bavaria. Hedwig Lewis SJ introduces us with the image of Mary Untier of Knots along with that to the increasingly popular devotion to ‘Mary Untier of of Our Lady of Lujan, a popular Marian devotion in Knots’. Argentina. ‘Mary Untier of Knots, pray for us’ would be a strange- sounding invocation in the Litany to Our Lady to which The Painting we are so accustomed. In fact, devotion to the Blessed The original Baroque painting of ‘Mary Untier of Knots’, Virgin under this title has been common in parts of by Johann George Melchior Schmidtner, dating from Germany for centuries. Recently, however, the world’s around 1700, is found in the church of St. -

Enforcement Discretion at the SEC
FIRST TEXAS EDIT DZ RESPONSE (DO NOT DELETE) 2/21/2016 6:25 PM6:24 PM Enforcement Discretion at the SEC David Zaring* The Dodd Frank Wall Street Reform Act allowed the Securities & Exchange Commission to bring almost any claim that it can file in federal court to its own Administrative Law Judges. The agency has since taken up this power against a panoply of alleged insider traders and other perpetrators of securities fraud. Many targets of SEC ALJ enforcement actions have sued on equal protection, due process, and separation of powers grounds, seeking to require the agency to sue them in court, if at all. This article evaluates the SEC’s new ALJ policy both qualitatively and quantitatively, offering an in-depth perspective on how formal adjudication—the term for the sort of adjudication over which ALJs preside—works today. It argues that the suits challenging the SEC’s ALJ routing are without merit; agencies have almost absolute discretion as to who and how they prosecute, and administrative proceedings, which have a long history, do not threaten the Constitution. The controversy illuminates instead dueling traditions in the * Associate Professor, the Wharton School. Thanks to Vince Buccola, Peter Conti- Brown, Nico Cornell, Bill Fisher, David Law, Jerry Mashaw, Nicolas Parrillo, Andrew Tuch, Urska Velikonja, and Daniel Walfish for comments and discussion, to Kevin Hoagland-Hanson and Yanni Chen for research assistance, and to feedback at presentations at the Academy of Legal Studies in Business and at the National Business Law Scholars Conference. FIRST TEXAS EDIT DZ RESPONSE (DO NOT DELETE) 2/21/2016 6:25 PM6:24 PM 102 Texas Law Review [Vol.